 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
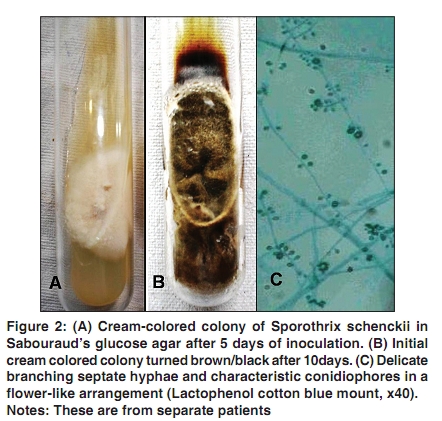
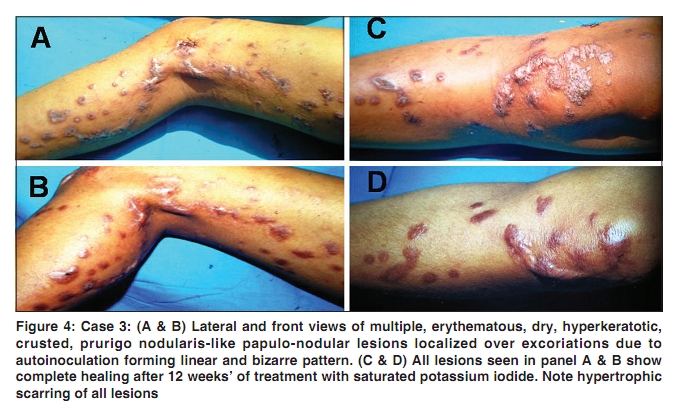
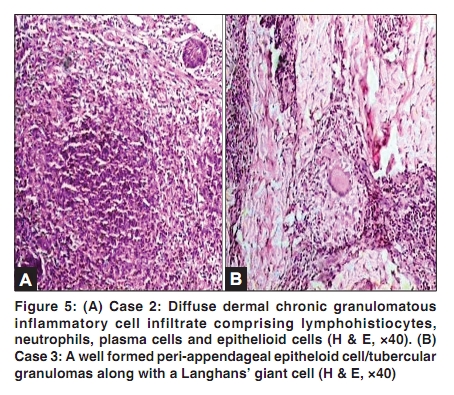
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 276-280 Case Report Cutaneous sporotrichosis: Unusual clinical presentations Vikram K. Mahajan, Nand Lal Sharma, Vinay Shanker1 , Poonam Gupta2 , Kavita Mardi 3 Department of Dermatology, Venereology and Leprosy, Dr. R. P. Govt. Medical College, Kangra (Tanda), Correspondence Address: Dr. Vikram K. Mahajan, Department of Dermatology, Venereology and Leprosy, Dr. R. P. Govt. Medical College, Kangra (Tanda)-176 001, Himachal Pradesh, India, vkm1@rediffmail.com Code Number: dv10084 PMID: 20445301 DOI: 10.4103/0378-6323.62974 Abstract Three unusual clinical forms of sporotrichosis described in this paper will be a primer for the clinicians for an early diagnosis and treatment, especially in its unusual presentations. Case 1, a 52-year-old man, developed sporotrichosis over pre-existing facial nodulo-ulcerative basal cell carcinoma of seven-year duration, due to its contamination perhaps from topical herbal pastes and lymphocutaneous sporotrichosis over right hand/forearm from facial lesion/herbal paste. Case 2, a 25-year-old woman, presented with disseminated systemic-cutaneous, osteoarticular and possibly pleural (effusion) sporotrichosis. There was no laboratory evidence of tuberculosis and treatment with anti-tuberculosis drugs (ATT) did not benefit. Both these cases were diagnosed by histopathology/culture of S. schenckii from tissue specimens. Case 3, a 20-year-old girl, had multiple intensely pruritic, nodular lesions over/around left knee of two-year duration. She was diagnosed clinically as a case of prurigo nodularis and histologically as cutaneous tuberculosis, albeit, other laboratory investigations and treatment with ATT did not support the diagnosis. All the three patients responded well to saturated solution of potassium iodide (SSKI) therapy. A high clinical suspicion is important in early diagnosis and treatment to prevent chronicity and morbidity in these patients. SSKI is fairly safe and effective when itraconazole is not affordable/ available.Keywords: Extracutaneous (systemic) sporotrichosis, fixed cutaneous sporotrichosis, lymphocutaneous sporotrichosis, multifocal (disseminated) cutaneous sporotrichosis, Sporothrix schenckii Introduction Sporotrichosis is a chronic granulomatous subcutaneous mycotic infection caused by Sporothrix schenckii, a common saprophyte of soil, plant detritus and sphagnum moss. The disease is almost endemic in tropics/subtropics. Agriculturists, foresters, gardeners, florists and nursery workers handling plants or plant material are particularly at risk. Traumatic inoculation is the typical mode for acquisition of skin infection in immunocompetent hosts. S. schenckii exhibits temperature dimorphism; it exists as a mold at room temperature (26°C) and as yeast in the host tissues (37°C). Culture of S. schenckii from tissue specimens on Sabouraud's dextrose agar (SDA) or Mycosel at 25°C and colony characteristics, demonstration of temperature dimorphism, delicate branching septate hyphae, and typical conidiophores in a flower-like arrangement (in lactophenol cotton blue preparation) remain gold standard to identify S. schenckii. Its identification by animal inoculation, histochemical or immunohistochemical studies, and detection by PCR [1],[2] is rarely needed for routine diagnosis. Clinically sporotrichosis manifests as: 1) lymphocutaneous, 2) fixed cutaneous, 3) multifocal or disseminated cutaneous, and 4) extracutaneous or systemic sporotrichosis. Diagnosis of cutaneous sporotrichosis is usually clinical and relatively easy in lymphocutaneous variety which accounts for 70-80% of the cases. [1],[3] It is characterized by a nodulo-ulcerative lesion (sporotrichotic chancre) at inoculation site and strings of similar lesions along the lymphatics proximal to the initial lesion. Fixed cutaneous sporotrichosis is less common and occurs as localized, asymptomatic, erythematous, papulo-plaque, papulo-pustule, nodule or verrucous plaque and occasionally, a non-healing ulcer or a small abscess at the inoculation site. Multifocal (disseminated) cutaneous sporotrichosis (≥3 lesions involving two different anatomical sites) and extracutaneous (systemic, osteoarticular, pulmonary, meningeal) forms are very rare. While high cost preclude use of itraconazole in most resource poor countries, treatment with saturated solution of potassium iodide (SSKIΊ1gm/ml) is inexpensive, fairly safe and has been consistently effective. [4],[5] However, making a diagnosis itself is difficult especially in non-endemic areas for lack of clinical suspicion and variable morphology resulting in significant morbidity/scarring. The described three unusual clinical forms highlight the importance of high clinical suspicion in early diagnosis and treatment of this not so uncommon deep mycosis. Case Reports Case 1 A 52-year-old male agriculturist presented with a crusted ulcer over right cheek of 7-year duration. It had started spontaneously as a small asymptomatic, pigmented nodule over right infraorbital region. He frequently used topical application of herbal pastes/ointments but denied any prior injury/thorn prick. Progressively enlarging, it became ulcerated with sero-sanguineo-purulent discharge and crusting which had increased in last 6 months or so. During this period he also noticed asymptomatic multiple crusted plaques over right hand. Cutaneous examination [Figure - 1] showed a well defined, crusted ulcer having erythematous, pigmented and at places rough surfaced margins involving inner canthus, right side of the nasal bridge and right maxillary area. There were also multiple crusted plaques of variable size over right wrist, dorsal hand, middle and little fingers. He had no significant lymphadenopathy. Systemic examination and routine laboratory investigations including complete blood counts, serum biochemistry, urinalysis, and chest x-ray films were essentially normal. With the clinical diagnosis of rodent ulcer/basal cell carcinoma (BCC) skin biopsy from ulcer margin was submitted for histopathology. It revealed epidermal hyperplasia, keratotic plugging and acanthosis. Dermis showed nests/islands of cells with large oval to elongated nuclei and scanty cytoplasm with peripheral palisading, and fibroblastic proliferation of stromal tissue. The chronic granulomatous inflammatory infiltrate comprised of lymphocytes, neutrophils, eosinophils, epitheloid cells and Langhans' giant cells. Overall features were of BCC and deep fungal infection. A skin biopsy specimen from the wrist lesion showed pseudoepitheliomatous hyperplasia, intraepidermal abscesses and extensive inflammatory cell infiltrate of neutrophils, lympho-histiocytes and plasma cells in the dermis suggestive of deep fungal infection. Periodic acid Schiff (PAS) and Ziehl-Neelsen (Z-N) staining for both the biopsy tissues were negative. Biopsy specimens were also inoculated on Sabouraud's dextrose agar (SDA) without antibiotics and Lowenstein-Jensen (L-J) media. Cultures on SDA at 25°C grew characteristic colonies of S. schenckii, the initial cream-colored colonies turned brown/black after a few weeks and showed hyphae on incubation at 37°C in blood glucose-cystene agar (temperature dimorphism) [Figure - 2]. With the diagnosis of BCC having superadded cutaneous sporotrichosis and lymphocutaneous sporotrichosis right upper limb, he was given SSKI orally in a dose starting with 5 drops t.i.d. increasing to a maximum of 30 drops t.i.d. All lesions showed regression when he returned after 4 weeks. He was advised to continue SSKI and after 12 weeks of treatment wide surgical excision and grafting for BCC lesion was performed. There was no clinical evidence of recurrence at last visit after 20 weeks of SSKI treatment. Case 2 A 25-year-old female was hospitalized with erythematous painful ulcerated swelling over the base of right middle finger of 2 months' duration causing painful and restricted hand movements. Similar lesions had also developed over right wrist, forearm and elbow, right buttock, thigh and left leg during this period. Starting spontaneously as erythematous nodular lesions few of them burst in next 5-7 days discharging sero-sanguineo-purulent material. Historically, she was taking anti-tuberculosis treatment (ATT) comprising rifampicin (450 mg/d), isoniazid (300 mg/d), ethambutol (800 mg/d) and pyrazinamide (1,200 mg/d) for suspected tubercular minimal pleural effusion diagnosed 5 months back. She had also under gone incision and drainage 2 months back for suspected tubercular right knee effusion. On cutaneous examination [Figure - 3] lesions were multiple, erythematous to violaceous, nodulo-ulcerative swellings. They were warm to touch, tender and boggy in consistency. Some of them had serosanguineous discharge or crusting, and a puckered scar over right knee. There was no regional lymphadenopathy and other systemic examination was normal. She was investigated with the clinical diagnosis of disseminated tuberculosis. Routine laboratory investigations including pus culture (aerobic and anaerobic), chest X-ray, Mantoux test and HIV serology showed no abnormality. She had no other predisposing factors for immune suppression. Repeated microscopy of pus in potassium hydroxide (KOH) mounts or Z-N staining showed no grains or acid fast bacilli (AFB). X-ray films of right hand showed osteopenia of underlying bones and an osteolytic lesion in proximal phalanx of right middle finger. Biopsy from finger lesion revealed focal epithelial hyperplasia and acanthosis, vacuolar degeneration of basal layer and exocytosis, perivascular mononuclear cell infiltrate in the upper dermis, lymphohistiocytes, neutrophils, plasma cells and epithelioid cell infiltrate in the mid and lower dermis. PAS and Z-N staining was noncontributory. Culture of biopsy specimens on L-J media was negative while growth of S. schenckii was obtained on SDA (identified as in case 1). Healing of all skin lesions was observed after 12 weeks' treatment with SSKI. She did not follow up further. Case 3 A 20-year-old girl presented with multiple intensely pruritic lesions over left knee of 2-year duration. To start with she had developed a pruritic, erythematous papular lesion over anterio-lateral aspect of left knee just in front of head of fibula. She denied any history of prior injury at the site. Over the next few months new lesions kept appearing over and around the knee which were intensely itchy. Treatment from local practitioners provided no relief. Cutaneous examination [Figure - 4] showed multiple, erythematous, dry, hyperkeratotic, excoriated and crusted, prurigo nodularis-like lesions in linear and bizarre pattern over and around the left knee. Systemic examination and routine laboratory investigations were essentially normal. A lesional biopsy was submitted for histology with the clinical diagnosis of nodular prurigo. Histopathology of skin biopsy revealed well formed peri-appendageal epitheloid cell granulomas along with Langhans' giant cells in the papillary and reticular dermis, the features suggestive of lupus vulgaris [Figure - 5]. PAS and Z-N staining was noncontributory. Mantoux test was negative. No growth was obtained in culture of biopsy specimens on SDA and L-J media. She was put on ATT as in case 2 and asked to return after 4 weeks. However, she did not show any response to this treatment. Empirical treatment with SSKI started in view of endemicity of cutaneous sporotrichosis in the region. There was significant decrease in itching and lesion size within 4 weeks. Complete healing of all lesions with hypertrophic scarring was observed after 12 weeks' treatment. She was advised to continue SSKI for another 4 weeks. Discussion Sporotrichosis primarily involves the skin and surrounding lymphatics following traumatic inoculation of S. schenckii. The lesion at inoculation site can be multiple, may remain as such or nodules appear along the lymphatics. The histopathology is usually non-specific and variable. [4] Demonstration of cigar-shaped, oval to round or single budding forms of the yeast is diagnostic but is rarely possible due to their scanty presence. [6] Clinicopathologic correlation is thus important for diagnosis in most cases while culture of S. schenckii will be confirmatory. The initial diagnosis in our patients was mainly clinical correlating with histology/culture. Hematogenous spread or multiple traumatic implantations of the fungus is perhaps responsible for cutaneous dissemination and may even be seen in individuals apparently without any predisposing factors for immunosuppression. [1],[7] Although inoculation of the infected material usually occurs after thorn pricks, cuts or blunt injuries, contamination of a pre-existing wound with infected material is perhaps more important for clinical development of the disease. [4] This is also evident in our case 1 who had multifocal or disseminated cutaneous sporotrichosis. He primarily started with noduloulcerative BCC (rodent ulcer) which got contaminated possibly following frequent topical application of herbal pastes perhaps infected with causative fungus. He also developed clinicopathologically typical lymphocutaneous sporotrichosis involving right upper limb apparently from contamination of some innocuous occupational injury over hand most likely from facial lesion/herbal pastes. Extracutaneous disseminated sporotrichosis can present as sinusitis, osteoarticular, pulmonary, ocular or central nervous system disease. Although osteoarticular sporotrichosis is an uncommon manifestation of systemic disease, it remains the most common extracutaneous presentation and has been reported in immunocompetent as well as in immunocompromised patients. [8],[9],[10] Pulmonary disease is rare and occurs following inhalation of conidia. Clinically cough, low grade fever, weight loss, mediastinal lymphadenopathy, cavitation resembling tuberculosis, and fibrosis are usual. [11] Our case 2, an otherwise immunocompetent patient, perhaps started with pulmonary disease that was mistaken for pulmonary tuberculosis. She developed disseminated systemic sporotrichosis in the form of multiple skin lesions, osteomyelitis of a phalanx and most likely effusion of a knee joint. Skin lesions when developed provided prima facie evidence of systemic disease, later confirmed mycologically. Although treatment with SSKI benefited her, only amphotericin B or itraconazole should be preferred for extracuateous sporotrichosis. [6],[9],[12] Skin lesions are mostly asymptomatic, rarely mildly pruritic or painful. Apart from classic cutaneous sporotrichosis uncommon lesional morphology mimicking facial cellulitis, erysipelas, rosacea, sarcoidosis, BCC, keratoacanthoma, soft tissue sarcoma and pyoderma gangrenosum has been described. [13] To the best of our knowledge intensely pruritic, nodular prurigo-like lesions as seen in our case 3 are not reported hitherto in the literature. Trauma from repeated scratching apparently contributed in formation and spread of new lesions due to autoinoculation along excoriations resulting in linear and bizarre configuration. Although granulomatous histology was suggestive of mycobacterial (typical or atypical) infection, there was no response to ATT while favorable response to SSKI was suggestive as well as curative in her. Despite being from this high endemic region all our patients remained undiagnosed before dermatological consultation was sought. To overcome the problem of delayed or no diagnosis, importance of a strong clinical suspicion thus needs be emphasized. Timely initiation of an effective treatment is imperative to prevent chronicity and morbidity. A favorable response to SSKI is almost diagnostic especially in the absence of mycological support. [4],[5],[14] Response is usually evident within 2 weeks and healing occurs in 4-8 weeks. [4] However, the duration of therapy remains uncertain and treatment must be continued for another 4-8 weeks after the clinical cure for mycological cure. All our patients showed clinical cure with SSKI in 12 weeks. However, when cost is not a consideration, itraconazole (100-200 mg/d) given for 3-6 months is the drug of choice in all forms of sporotrichosis as well as in patients intolerant to SSKI. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10084f5.jpg] [dv10084f2.jpg] [dv10084f4.jpg] [dv10084f1.jpg] [dv10084f3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}