 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
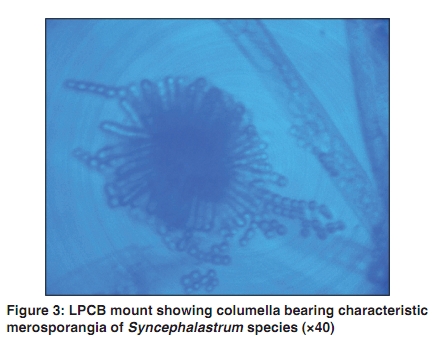
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 284-286 Letter to the Editor Syncephalastrum species producing mycetoma-like lesions Ritu Amatya, Basudha Khanal, Arpana Rijal 1 Departments of Microbiology and 1Dermatology, B.P. Koirala Institute of Health Sciences, Dharan, Nepal Correspondence Address: Dr. Ritu Amatya, Department of Microbiology, B.P. Koirala Institute of Health Sciences, Dharan, Nepal, ritu484@yahoo.co.in Code Number: dv10087 PMID: 20445304 DOI: 10.4103/0378-6323.62977 Sir, Syncephalastrum species is a fungus belonging to the class Zygomycetes and order Mucorale. [1] Despite their common occurrences in tropical soil, they rarely cause diseases. Unlike the pulmonary and central nervous system infections associated with other Zygomycetes, Syncephalastrum species is more likely to cause dermatomycoses and onychomycosis. We report a case of mycetoma-like lesions due to Syncephalastrum species. A 30-year-old immunocompetent, nonpregnant woman from the plains of eastern Nepal presented with multiple discharging lesions over the dorsum of her left foot. Six months prior to presentation, a bamboo stick accidentally pricked her foot while she was working in the field. A month later, she developed multiple nodules at the site of trauma. These gradually increased in size and ruptured, discharging sero-sanguinous fluid with no granules. Discharging sinuses were formed at these sites [Figure - 1]. The patient was treated elsewhere with antibiotics but did not respond. She also developed newer lesions extending up to the ankle of the left foot. History and examination revealed no other significant findings. A working diagnosis of mycetoma was made. Skin biopsies from different sites of the lesion were sent for histopathological examination and fungal culture. Histopathological report showed non specific inflammatory changes. Skin biopsies from the lesions were received in the Microbiology laboratory. The Gram stain and the KOH mounts revealed abundant hyaline, aseptate, broad and branching hyphae. Culture on Sabouraud's dextrose agar with chloramphenicol and gentamicin grew fluffy mould with grayish sporangium within 48 hours at 26°C [Figure - 2]. The reverse was pale yellow. Lactophenol cotton blue mount showed broad, aseptate, hyaline hyphae bearing erect sporangiophores terminating into globose columellae bearing the characteristic cylindrical merosporangia with rows of merosporangiospores [Figure - 3]. The isolate was identified as Syncephalastrum species. No other organisms were grown by bacterial and fungal cultures (including mycobacterial culture). This patient was however lost to follow-up. Syncephalastrum species is usually described as an opportunistic pathogen. [1] However, very few human cases are described. The first case with proven association was of cutaneous infection of thumb in an adult male suffering from diabetic ketosis. He was never treated for the mycoses and later succumbed to diabetes. [2] The second was a case of invasive infection of the anterior abdominal wall and omentum occurring after deep trauma to the abdomen in a previously well young man. He was successfully treated with partial surgical debridement and amphotericin B lipid complex. [3] The third proven case was of a big toe nail onychomycosis following nail trauma in an immunocompetent male. It was successfully treated with surgical nail avulsion and topical nystatin ointment. [4] Recently, a case of sino-orbital infection by Syncephalastrum racemosum in chronic hepatorenal disease patient who was successfully treated with partial surgical debridement followed by liposomal amphotericin B was reported by Baradkar et al.[5] Syncephalastrum species has been reported as a colonizer from healthy toe nails of students in Egypt. [1] However, the direct demonstration of fungal elements from biopsy specimens or from sterile sites; histopathological finding of tissue invasion, necrosis or vascular thrombi and repeated isolation of the fungi in multiple samples is conclusive of its being the pathogenic agent. [6] Rapid growth in SDA, the typical cultural characteristic and the microscopic morphology help to identify Syncephalastrum species. It must be differentiated from Aspergillus species. Cutaneous Zygomycetes may be very invasive locally involving the muscle and fascial layers beneath. [1] A combined approach of early diagnosis, aggressive, sometimes repeated surgical debridement, systemic antifungal and correction of the underlying condition where present should be the basis for treatment. [1] Amphotericin B is the only systemic antifungal that has clinically proven efficacy. Lipid formulations allows for higher doses up to 10-15mg/kg body weight/ day. However, the total dose and duration varies with the individual response. Combination of liposomal amphotericin B with posaconazole or caspofungin has been used in invasive zygomycosis as salvage therapy. [7] The importance of this case is that it describes a definitively proven case of human infection by Syncephalastrum species. Literature search could track only four other published reports of definitively proven human cases of zygomycosis by Syncephalastrum species. The lesions in this case resemble mycetoma, except for the absence of granules. The fungi could be demonstrated in multiple tissue biopsies in direct KOH mount and all specimens grew the characteristic fungi. Also, unlike the usual group of immunocompromised and diabetic patients where the Zygomycetes infections are usually encountered, this occurred in a healthy adult. She could have acquired the infection from the soil contaminated bamboo stick prick. This case should alert both clinicians and microbiologists to consider Syncephalastrum species a possible cause of such types of lesions. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10087f1.jpg] [dv10087f3.jpg] [dv10087f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}