 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
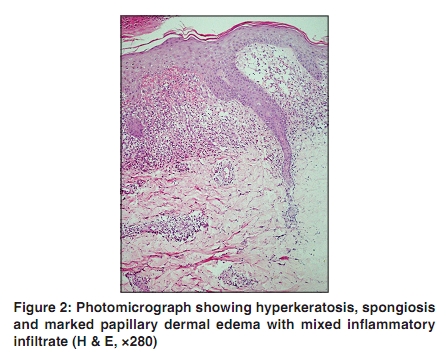
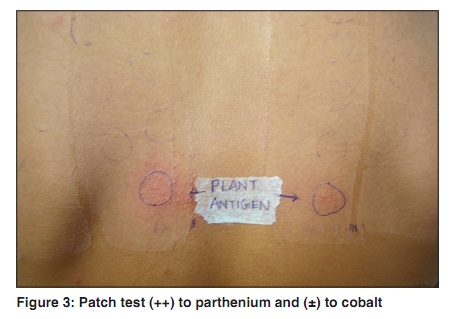
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 286-287 Letter to the Editor Contact dermatitis to parthenium simulating lichen nitidus Dipankar De, Rashmi Jindal, Amrinder J. Kanwar Department of Dermatology, Venereology & Leprology Postgraduate Institute of Medical Education and Research, Chandigarh, India Correspondence Address: Dr Amrinder J Kanwar, Department of Dermatology, Venereology & Leprology Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India, ajkanwar1948@gmail.com Code Number: dv10088 PMID: 20445305 DOI: 10.4103/0378-6323.62978 Sir, A 20-year-old male manual laborer sought dermatology consultation for itchy minimally red eruptions over dorsum of hands, elbows and feet, present for 2.5 years. The lesions started appearing on dorsum of hands and then progressed to other areas. They were itchy and non-oozy. There was no history of seasonal variation in severity of disease. He gave history of aggravation after work with cement, farming and exposure to sun. There was no personal or family history of atopy. On cutaneous examination, there were multiple well defined, discrete flat topped erythematous to skin colored papules with a shiny surface and the lesions were arranged in clusters [Figure - 1]. No lesion was present elsewhere including genitalia. Previous use of topical steroids, antihistamines and emollients was of some help. Based on the morphology of lesions, provisional diagnosis of lichen nitidus, polymorphous light eruptions and contact dermatitis was considered. A biopsy specimen was obtained from one of the papules, which on histopathological examination revealed hyperkeratosis, spongiosis and lymphocytic dermal infiltrate consistent with spongiotic dermatitis [Figure - 2]. Patch test was done with Indian standard series and plant antigens including parthenium. The patch test was positive for cobalt (±) and parthenium (++) on day 2 and day 4 [Figure - 3] according to the International Contact Dermatitis Research Group Criteria. Considering his occupation, we reached a diagnosis of contact dermatitis to parthenium. Temporary change in occupation along with a short course of oral prednisolone 40 mg/day, topical steroids (clobetasol propionate 0.05%), antihistamines and photo protection led to substantial recovery after four weeks of therapy. Parthenium hysterophorous, a member of the family compositae, is an exotic weed introduced accidentally in India in 1956 through imported wheat. Characteristically, parthenium causes air borne contact dermatitis (ABCD) which starts from the exposed sites of face, neck and flexures with erythema, papules, occasional blistering and intense pruritus resulting later in skin thickening, hyperpigmentation and development of leonine facies. Apart from ABCD, other patterns of manifestation are photodermatitis, atopic dermatitis, seborrheic dermatitis and photosensitive lichenoid dermatitis. [1] Hand dermatitis as a pattern of parthenium dermatitis has also been recorded especially in gardeners after contact with the weed. [2] Such wide varieties of patterns cannot be explained only on the basis of delayed type IV hypersensitivity. Therefore, combined type I and IV hypersensitivity to parthenium has been recently postulated. In case of atopic, Type I hypersensitivity mediated by IgE antibody is thought to initiate and perpetuate the dermatitis. [3] Parthenium hysterophorous may precipitate or exacerbate the atopic dermatitis which presents with photo aggravation, heat intolerance and flexural involvement. In atopics, apart from the usual patterns of parthenium induced dermatitis, prurigo nodularis and chronic actinic dermatitis can be observed. [4],[5] The morphology of lesions in our patient resembled lichen nitidus, which was excluded by histopathological examination and patch test. In case of non-eczematous contact dermatitis patch test reaction patterns are more often eczematous as was seen in our patient. It is important to consider a diagnosis of parthenium dermatitis in every patient who has occupational exposure to parthenium and present with eruptions in exposed parts of the body. This is imperative because parthenium contact dermatitis presents with widely variable morphology. Diagnosis should be substantiated by histopathology and patch test. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10088f2.jpg] [dv10088f3.jpg] [dv10088f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}