 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
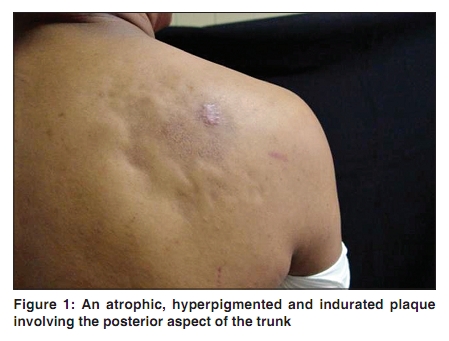
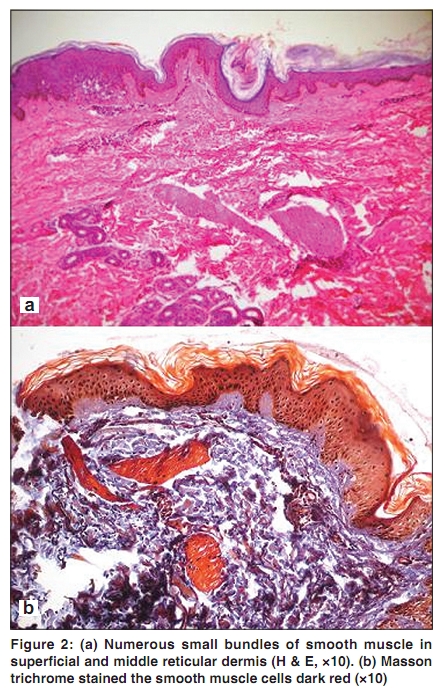
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 290-291 Letter to the Editor Smooth muscle hamartoma presenting as a morphea-like plaque Andrés Tirado-Sánchez, Aleida Santamaría-Román, Rosa María Ponce-Olivera Servicio de Dermatología, Hospital General de México, O.D., México, D.F. Correspondence Address: Dr. Andrés Tirado Sánchez, Servicio de Dermatología, Hospital General de México, O.D., Dr. Balmis 148, Col. Doctores, Deleg. Cuauhtemoc, México, D.F., C.P. 06720, andrestiradosanchez@hotmail.com Code Number: dv10091 PMID: 20445308 DOI: 10.4103/0378-6323.62984 Sir, Smooth muscle hamartoma (SMH), first described by Stokes in 1923, [1] is a skin tumor, congenital or acquired, characterized by a proliferation of smooth muscle bundles within the reticular dermis. [2] Its clinical presentation is varied. It commonly occurs as a skin-colored or hyperpigmented plaque on the trunk or extremities, as a patch with follicular papules or even as a cause of Michelin tire syndrome. [3] We describe an unusual case of SMH resembling a morphea plaque. We report a 30-year-old man who had a depressed, hyperpigmented and infiltrated plaque involving the posterior aspect of the trunk. To our knowledge, this is the first report of an acquired SMH presenting as a morphea plaque. The lesion described was firm to palpation and the skin appeared somewhat atrophic and hyperpigmented [Figure - 1]. No hypertrichosis or pseudo-Darier (increased induration of a lesion induced by rubbing) [4] were noted. The lesion did not cause any discomfort to the patient. His medical history was uneventful and no family history of similar lesion was reported. An incisional biopsy was performed and analysis of the specimen showed no hyperkeratosis, papillomatosis or atrophic epidermis; only uniform hyperpigmentation of the basal layer. Numerous small bundles of smooth muscle were seen in superficial and middle portions of the reticular dermis [Figure - 2]a. Individual cells were in appearance with cigar-shaped nuclei and without atypical features. Masson trichrome stained the smooth muscle cells dark red [Figure - 2]b. Histologic examination was compatible with SMH. Acquired SMH is usually seen in association with Becker's nevus and is accompanied by hyperpigmentation and hypertrichosis. [5] However, acquired SMH has been reported as an independent entity. [6] The typical presentation of acquired SMH is that of a slightly hyperpigmented plaque, usually located on the trunk (lumbosacral area). [2],[3] Hyperpigmentation, induration, and localized hypertrichosis tend to diminish with time, in contrast with Becker's melanosis. Other clinical differential diagnosis include solitary mastocytoma, cafι au lait spot, pigmented hairy nevocellular nevus, Becker's nevus and myokymia. However, these diseases are either congenital or not indurated. [7] In our case, diagnosis of morphea should be included. [8] The histologic diagnosis is made by light microscopy of a skin biopsy specimen that shows a well-demarcated lesion composed of variable oriented smooth muscle bundles usually located within the reticular dermis. [9] The overlying epidermis frequently shows hyperpigmentation of the basal layer. [3] In addition to hyperpigmentation, about half of the patients have hyperkeratosis and papillomatosis, reminiscent of Becker's melanosis. It can be differentiated from the secondary smooth muscle hyperplasia that may be seen in Becker's nevus, by the degree of muscle proliferation, which is more pronounced in SMH. [9] We are reporting this case of acquired SMH, that presented as a morphea-like plaque, with hyperpigmentation and without hypertrichosis and pseudo-Darier sign. To our knowledge, this is the first description of such presentation in an acquired SMH. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10091f2.jpg] [dv10091f1.jpg] |
| |||||||||


{kind=link}
{kind=link}