 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
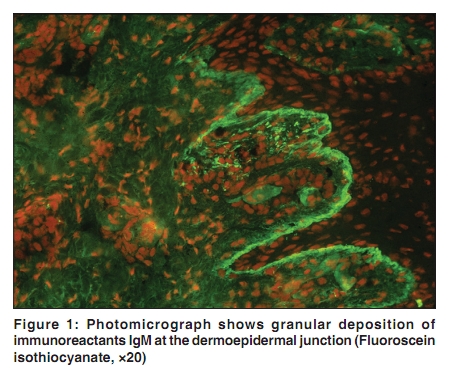
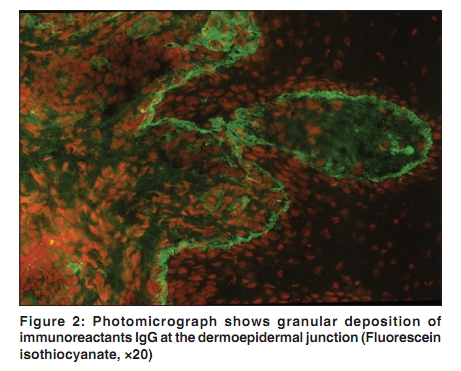
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 298-300 Resident's Page Lupus band test Vandana Mehta, Aarti Sarda, C. Balachandran Department of Skin & STD, Kasturba Medical College, Manipal, Karnataka, India Correspondence Address: Dr. Vandana Mehta, Department of Skin &STD, Kasturba Medical College, Manipal 576104, Karnataka, India, vandanamht@yahoo.com Code Number: dv10095 PMID: 20445312 DOI: 10.4103/0378-6323.62983 Introduction Systemic lupus erythematosus is a heterogenous chronic autoimmune disease affecting one or more organ systems and is characterized by the production of various autoantibodies, complement consumption and the presence of circulating immune complexes. In the diseased tissue of SLE and DLE, liquefactive degeneration of the basal cells with edematous changes and thickened subepidermal basement membrane are characteristic features. In 1953, Burnham et al, found conspicuous deposits of immunoglobulins and complement at the dermo-epidermal junction in accord with the thickened PAS positive basement membranes. [1] Cormane et al, demonstrated similar deposits in clinically normal skin of SLE, but not in that of DLE. [1] This deposition of immunoglobulins and complement components in the skin of patients with lupus erythematosus, demonstrable as a linear band at the basement membrane zone was named Lupus Band Test. All three major immunoglobulin classes (IgG, IgM and IgA) and a variety of complement components including constituents of the membrane attack complex have been identified in these DEJ deposits. [2] Definition Deposition of immunoglobulins and complement components in the skin of patients with lupus erythematosus (LE), demonstrable as a linear band at the basement membrane zone (BMZ) by direct immunofluorescence, is termed Lupus band test (LBT). [3] The test is considered positive when one or more immunoreactants (IgG, IgA, IgM, C3) are found at the DEJ. [4] When three or more immunoreactants are present in the nonlesional LBT, the diagnostic specificity for SLE is very high. The presence of membrane attack complex at the DEJ is relatively sensitive and specific for LE. When one refers to LBT, the exact site of biopsy whether involved or uninvolved, light exposed or light protected,should be specified. The terms lesional LBT and non-lesional LBT are therefore used to denote biopsy from involved and uninvolved skin respectively. Sensitivity and specificity LBT is a very sensitive and specific test for LE. Apppoximately 90-95% of the patients with systemic or discoid lupus erythematosus have positive LBT in involved skin. In SLE, the sensitivity was 95% and specificity 87%. Positive predictive value was 64% and negative predictive value 98%. [5] There is general agreement that the LBT is very specific with less than 1% false positive reactions. [6] It also has considerable value as a prognostic indicator in a patient with an established diagnosis of LE. On comparision of effects of cyclophosphamide (CY) and 6-mercaptopurine (6-MP) on the accumulation of subepidermal immunoglobulins and glomerular immunoglobulins in the female mice, subepidermal immunoglobulins were present in 30% of the untreated animals, in none of the cyclophosphamide treated mice, and in 83% of the 6-MP treated mice. [7] Staining patterns of LBT The immunoglobulin staining pattern of immunoreactants in nonlesional LE skin under low power generally is described as being granular [Figure - 1],[Figure - 2]. Under high power, the patterns of immunoglobulin deposition at the dermo-epidermal junction have been described as homogenous, fibrillar, stippled, shaggy, lumpy-bumpy, linear or thready. [3] All of these are seen in a continuous fashion. Discontinuous or interrupted LBT can be seen in a number of other disorders such as actinic keratosis, polymorphic light eruption, rosacea and in 80% of nonlesional sun exposed skin and thus is much less specific for LE. [1] Ultrastructurally, these immunoreactants are seen to be deposited on or below lamina densa of the DEJ. A stippled pattern of LBT consisting of multiple small round points of fluorescence is the type most commonly seen in clinically normal skin of SLE. In some patients, sparser, more elongated and threadlike stipples can be seen. [8] A homogenous or solid band of well demarcated, bright fluorescence is seen mostly in chronic atrophic and hypertrophic skin lesions. A thready pattern consisting of short, closely set, bright threads or fibrils is seen in more acute erythematous, edematous lesions. Shaggy, fibrillar, lumpy-bumpy and granular patterns have also been seen, usually in a continuous pattern along the DEJ. [8] Uses The value of LBT as a diagnostic tool is well established. Its primary use is in diagnosing LE in patients with cutaneous lesions. The test in involved skin is a very sensitive indicator of LE. The sensitivity of the lupus band test for active disease is higher than that of other laboratory variables such as serum C3 and C4 levels, anti-DNA antibody, LE cell test, lymphocyte count and ESR. The diagnostic specificity of LBT is also very high in differentiating LE from other cutaneous disorders that are clinically similar such as polymorphic light eruption, benign lymphocytic infiltrate of Jessner's, lymphocytoma cutis, etc. A positive non-lesional LBT in fully protected skin from buttocks or inner aspect of upper arm that consists of three or more immunoglobulins or complement components might have the highest specificity for SLE. Its second diagnostic value is in the differential diagnosis of systemic from discoid LE. Studies have shown immunoglobulin and complement at the dermal-epidermal junction in systemic LE in both involved and uninvolved skin and only in involved skin in discoid LE. It is thus essential that appropriate skin site be selected for biopsy, be it involved or uninvolved skin, light exposed or light protected skin. The third diagnostic value is in making a diagnosis of systemic LE in patients without cutaneous lesions. A positive band test in clinically normal skin provides early confirmation of SLE even in patients without LE lesions where neither a biopsy nor band test can be performed on a skin lesion. The fourth diagnostic value is in the diagnosis of SLE from other antinuclear-antibody positive diseases like drug induced LE, rheumatoid arthritis, scleroderma, dermatomyositis and mixed connective tissue diseases. LBT also has prognostic significance. Positive LBT from sun protected normal skin indicates decreased long term survival. It helps in assessing the severity of the disease and correlates positively with risk of developing nephritis. [9] Biopsy specimens taken for prognostic purposes must come from clinically normal, light protected skin such as the medial flexor forearm, medial upper arm and buttocks. Davis and Gilliam studied these deposits in a prospective follow up study spread over 10 years, and found that the patients with positive LBT of the IgG class had poorer prognosis than LBT-negative patients. [10] However, LBT is subjective and requires long experience to achieve consistency and reliability of results. Also negative test does not rule out SLE. False positive LBT is seen in:
False negative LBT False Negative non lesional LBT is seen when high levels of extra vascular dermal IgG is present. [2] Considerable anatomic regional variation also occurs in positive lesional LBT with a cephalocaudal gradient, with lesions on the head more often being positive than those on the trunk. [12] Conclusion The interpretation of a positive lupus band requires detailed knowledge of several correlates, such as site of the biopsy (lesional or normal skin), composition, morphology and brightness of the immunofluorescence band, other associated serologic findings and response to treatment. A positive LBT on sun-protected non-lesional skin (if showing the presence of only one immunoreactant at the DEJ) represents a useful and specific criterion for identifying patients with LE. [13] LBT on sun-protected normal skin may be useful in diagnosing SLE in patients with inconclusive clinical and serological profiles and may be also of prognostic significance, particularly if three immunoglobulins are found at the DEJ. LBT is a laboratory procedure and therefore should be used in conjunction with clinical findings and other serological and immunopathological tests to arrive at a final diagnosis. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10095f1.jpg] [dv10095f2.jpg] |
| |||||||||

{kind=link}
{kind=link}