 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
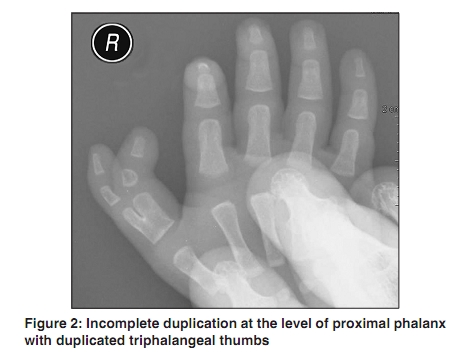
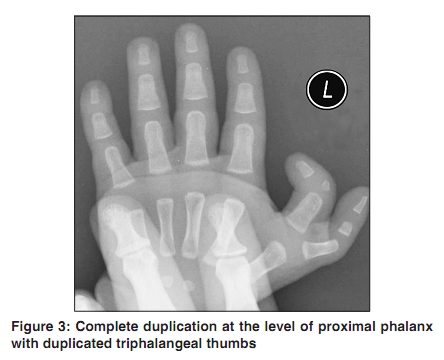
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 307 Net letter Polydactyly of triphalangeal thumb Sanjay Saraf, Ravi Singh Parihar Department of Plastic Surgery, NMC Specialty Hospital, Dubai, UAE Correspondence Address: Dr. Sanjay Saraf, Department of Plastic Surgery, NMC Specialty Hospital Dubai, U.A.E., drsaraf@hotmail.com Code Number: dv10099 PMID: 20445317 DOI: 10.4103/0378-6323.62986 Sir, A two-month-old, full term normally delivered infant presented to us with bilateral duplication of thumbs. The antenatal history was not significant with no exposure to any viral infection, drugs, alcohol, or radiation. There were no similar anomalies in the feet, no positive sibling or family history and no associated cardiovascular, gastrointestinal, musculo-skeletal or genitourinary system anomalies. On examination, the child was found to have bilateral preaxial polydactyly with duplicated thumbs. [Figure - 1] The radial duplicates were well formed but less developed than normal with ulnar divergence. The duplicated thumb had well developed bones, soft tissue with well-formed nails. Mild movements were observed at the meta-carpo phalangeal and interphalangeal joints of the hypoplastic thumb as compared to the larger thumb. The X-rays revealed incomplete duplication at the level of proximal phalanx with duplicated triphalangeal thumbs on the right side [Figure - 2] and complete duplication at the level of proximal phalanx with duplicated triphalangeal thumbs on the left side. [Figure - 3] The metacarpals bilaterally were grossly normal. Congenital hand anomalies have prevalence at birth of about 5:1000 [1] and preaxial polydactyly (radial polydactyly) is the most common anomaly occurring in 1:3000 births. Triphalangeal thumb (TPT) is regarded as a subtype of preaxial polydactyly with reported prevalence as 1:25,000. [2] According to one estimate, the TPT polydactyly combination accounts for two per cent of congenital malformations of the upper extremities. [3] The classification of pre-axial polydactyly is complex and many attempts have been made to develop an adequate classification system. The most widely accepted classification for categorizing polydactyly of the thumb is the classification described by Wassel based on the skeletal morphology, particularly the level of duplication. [4] The Wassel type IV deformity is usually the most common followed by Wassel type II. The presented case falls in Wassel type VII thumb duplication. The Wassel classification system Wassel type description
The exact cause of pre-axial polydactyly is not known. Most cases occur sporadically without any defined inheritance pattern or known genetic association. However, in most instances the TPT-polydactyly combination is inherited as an autosomal dominant trait and genetic analysis of multiple Dutch pedigrees with triphalangeal thumbs has localized this genetically transmitted malformation to the long arm of chromosome 7 (7q). [6] Pre-axial polydactyly tends to occur more frequently in Caucasians, Asians, and Native Americans. In general, males are more commonly affected than females and usually one hand is involved. TPT may occur as an isolated defect, in combination with other malformations of the hands, or as a feature of a syndrome or sequence. [7] The isolated triphalangeal thumb usually presents as a long fingerlike thumb with deviation in the same plane as the fingers. Most of the TPT-polydactyly thumbs have their level of duplication at or proximal to the MP joint. The accessory thumb may be hypoplastic to various extents and the lesser ones should be clearly differentiated from skin adnexal tumors. In TPT, apart from the morphological forms, the involved ligaments, muscles, tendons and joints of the duplicated thumb from distal interphalangeal joint to radiocarpal joint can be hypoplastic, malformed, or absent with varying degrees of stiffness or instability. Also, the first web can be insufficient with deformities in the other hand. In cases of duplicated triphalangeal thumb, additionally, the clinical presentation can further vary depending upon the shape (wedge to rectangular) and consequent angular deviation (clinodactyly). There is no standard surgical procedure for correcting polydactyly of TPT. The aim of the treatment is to achieve a single, functioning thumb with acceptable appearance. Usually the thumb that is retained is the one with anatomic features that will give better stability, strength and mobility. [8] This is usually, but not invariably, the ulnar thumb. Typically, surgery is performed around one year of age, before the development of pinch and fine motor function. The surgical treatment usually entails preservation of the larger thumb with excision of the smaller one with removal of the bony elements of the smaller thumb and reconstructing the remaining skin, tendons, ligaments, joints, and fingernails to form a well functioning thumb. For TPT correction, operations vary from removal of the delta phalanx with ligament reconstruction to multiple osteotomies and rebalancing. The knowledge of the complex underlying anatomy is an essential prerequisite for rewarding results. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10099f1.jpg] [dv10099f3.jpg] [dv10099f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}