 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
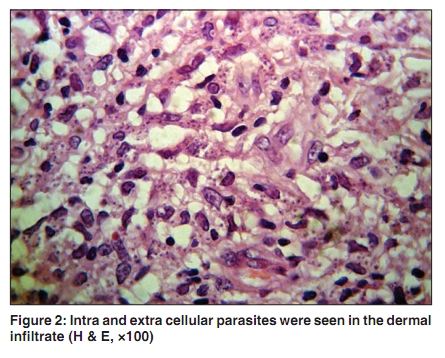
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 76, No. 3, May-June, 2010, pp. 307 Net letter Bilateral cutaneous leishmaniasis presenting as eczema-like eruptions on the hands Soheila Nasiri, Reza Mahmoud Robati, Afsaneh Marefat, Marjan Saeedi, Nima Sarrafi-rad Skin Research Center, Shahid Beheshti University, M.C. Shohada-e Tajrish Hospital, Tehran, Iran Correspondence Address: Dr. Mahmoud Robati, Skin Research Center, Shahid Beheshti University, M.C. Shohada-e Tajrish Hospital, Shahrdari St, Tehran, Iran, rmrobati@gmail.com Code Number: dv10100 PMID: 20445316 DOI: 10.4103/0378-6323.62987 Sir, Leishmania infection is caused by the protozoan leishmania and transmitted by the bite of infected phlebotomine sand flies. The clinical manifestation of leishmaniasis depends on the infecting leishmania species, and also on the host cellular immunity. Leishmania is a 2-5 micrometer parasite. [1],[2] The incubation period is one to three months with the appearance of skin lesions that progress from a papule to an ulcer. The ulcer spontaneously resolves over a 6-12 month period, leaving a scar. [3] Clinical differential diagnosis of localized cutaneous leishmaniasis (CL) may include fungal, bacterial or viral infections, sarcoidosis, basal and squamous cell carcinomas, cutaneous lymphoma, lupus vulgaris, discoid lupus erythematosus and cutaneous metastases. [1],[4] While cutaneous leishmaniasis frequently causes ulcerated papules or nodules, various unusual clinical presentations of leishmaniasis has been reported including impetiginized hyperkeratotic plaques, warty, zosteriform, erysipeloid or sporotrichoid forms. One of these bizarre manifestations of leishmaniasis could be eczematous lesions that we have reported in one case of this presentation here. [5],[6] A 40-year-old Iranian man presented with a one-year history of a pruritic erythematous, edematous, indurated plaques on the dorsal aspects of both hands [Figure - 1]. The patient had been treated with the clinical diagnosis of irritant contact dermatitis before we visited him, but there was no response to topical corticosteroid therapy. The history for atopic dermatitis and other disease was negative. On clinical examination, there were 20 to 25 cm crusted indurated erythematous plaques with surface scaling involving the dorsal surface of the hands. No palpable lymphatic node detected. Routine laboratory tests were normal including a negative HIV serology. A biopsy was obtained from these lesions. Histology demonstrated focal parakeratosis, focal hypergranulosis, mild spongiosis and acanthosis of epidermis and diffuse infiltration composed of histiocytes, lymphocytes and plasma cells throughout the entire dermis. Intra and extra cellular parasites were seen in the dermal infiltrate [Figure - 2]. The patient responded to parentral glucantim (20 mg/kg), with complete resolution of lesion after a 2-week treatment. The eczematoid form of CL seems not to be very common and its incidence is reported to be 2.3 % from a study in Iran. [5] In this report, the symmetrical distribution, the great size of the lesion and the absence of any primary plaque or nodule were atypical. The medical history of our patient had no significant points to account for the unusual clinical picture. Whether this was the consequence of multiple sandfly bites, a specific immune response or lack of response, from an atypical leishmania strain, is not clear. [2] We found only a few reports of cutaneous leishmaniasis with eczema-like eruption in the literature. [2],[7] We report here a very rare case of bilateral and symmetrical cutaneous leishmaniasis that was localized exclusively on dorsal aspect of both hands. So remember CL in the differential diagnosis of unresponsive eczematous eruptions especially in areas where CL is epidemic or endemic, such as our region. References
Copyright 2010 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv10100f1.jpg] [dv10100f2.jpg] |
| |||||||||


{kind=link}
{kind=link}