 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
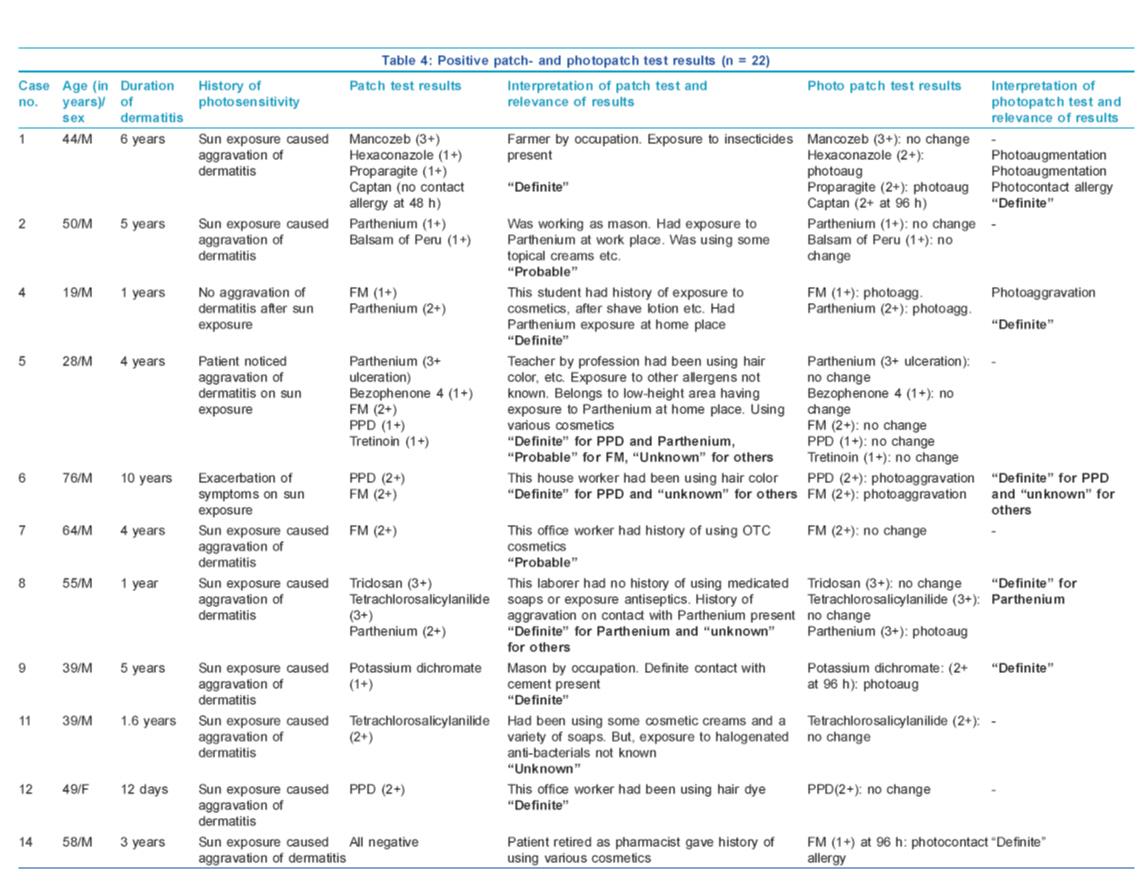
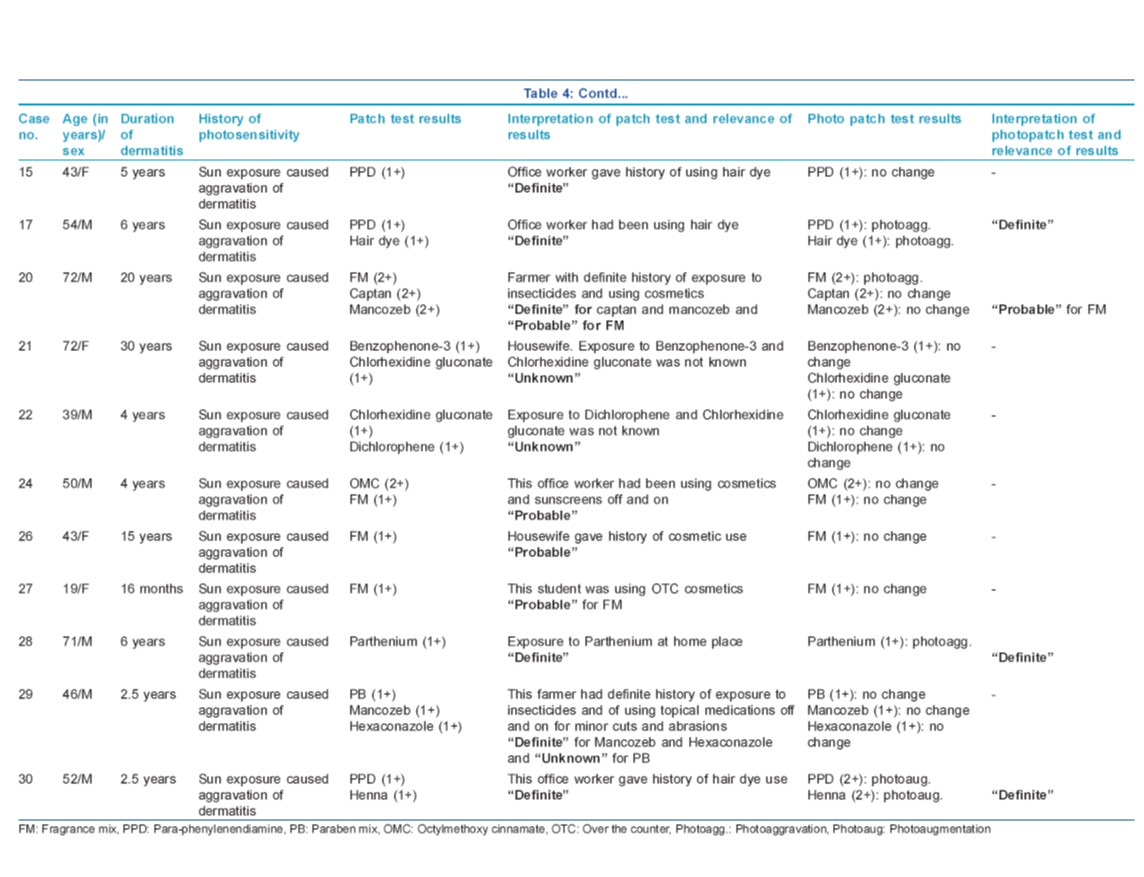
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 2, March-April, 2011, pp. 148-155 Original Article Evaluation of photopatch test allergens for Indian patients of photodermatitis: Preliminary results Nidhi Jindal1, Nand Lal Sharma2, Vikram Kumar Mahajan2, Vinay Shanker1, Gita Ram Tegta1, Ghanshyam Kumar Verma1 1 Department of Dermatology, Venereology and Leprosy, Indira Gandhi Medical College, Shimla, India Correspondence Address: Nand Lal Sharma, Department of Dermatology and Venereology, RPGMC, Kangra (Tanda), Himachal Pradesh, India, nandlals@hotmail.com Code Number: dv11043 PMID: 21393943 DOI: 10.4103/0378-6323.77453 Abstract Background: There is a strong need to develop a photopatch test tray suitable for Indian patients of photodermatitis as European/Scandinavian photopatch test trays may not be wholly relevant for them.Aim: We carried out this study using photoallergens relevant in the Indian context to determine their relevance in patients of photodermatitis. Methods: Thirty patients (M:F, 23:7) between 19 and 76 years of age of photodermatitis and 10 controls were patch- and photopatch tested with 20 common photoallergens. In addition, the patients were also (photo) patch tested with articles of daily use as and when these were suspected to be the cause. Results: Forty-three positive reactions to one or more antigens were seen in 22 (74%) patients. Fourteen positive photopatch tests to seven allergens were observed in 10 (33%) patients, and nine (30%) of them had a definite relevance. The most common contact allergen was fragrance mix (FM) (30%), followed by p-phenylenediamine (20%) and Parthenium hysterophorous (17%). The definite relevance of the patch- and photopatch tests could be correlated in 47% of these patients. Conclusions: FM is the most common contact and photocontact allergen among the various photopatch test antigens. Although differences in technique and evaluation make direct comparison between different centers difficult, still photopatch testing remains an integral part and gold standard for the work-up of the photosensitive patients. Keywords: Photo dermatitis, photopatch test, captan, fragrance mix Introduction Photosensitivity is a poorly understood cutaneous reaction to sunlight probably involving the immune system. Photoallergic dermatitis is caused by direct contact of skin with the causative agent and subsequent exposure to light of a certain wavelength. The common photosensitizing agents include chemicals used in sunscreens, antiseptic agents, fragrances and non-steroidal anti-inflammatory agents. A thorough history, especially of evolution of symptoms and of photoaggravation combined with photopatch testing, is an effective approach for the diagnosis of photodermatitis or unclear photoreactions that cannot be associated with genuine photodermatoses. Photopatch testing helps in determining the sensitizing potentials of commonly used agents. Recommendations differ widely across the various photodermatitis research groups, and include variations in test procedures and interpretation, the range of tests substances, the irradiation doses, the precise irradiating wavelengths, the timing of irradiation, the irradiance used and the delay before reading of results. [1],[2],[3] Despite these variations, approximately 4-20% of the patients who undergo photopatch testing have clinically relevant positive results, eventuating in the diagnosis of photoallergic contact dermatitis. [1],[4] There is no Indian standard photopatch test series available, and few studies carried out in India have used European/Scandinavian photo patch test trays, which may not be wholly relevant for Indian patients. Hence, there is a strong need to develop a photopatch test tray suitable for Indian patients of photodermatitis. In this study, we present the preliminary results of photopatch testing using allergens relevant in the Indian context and their relevance in the Indian patients of photodermatitis. Methods Thirty consecutive patients (excluding pregnant/lactating females and children aged <18 years) of clinically diagnosed photodermatitis attending the Outpatient Dermatology Department were patch tested between July 2008 and June 2009. Other exclusion criteria included any systemic or congenital disorder and idiopathic photodermatoses known for photosensitivity. Patients having acute dermatitis were enrolled after the acute episode subsided or when the dose of prednisolone was <20 mg/d. Clinical details regarding age, sex, occupation, duration and progress of dermatitis, aggravating factors for photoaggravation and treatment (topical or systemic, particularly photosensitizing drugs) taken were recorded and lesions were charted. Ten subjects were also selected as controls from patients having minor dermatoses other than dermatitis or photodermatitis. The patch test antigens comprising 20 common photoallergens [Table - 1] were photopatch tested by the Finn Chamber method after obtaining written consent. Para-phenylenediamine (PPD), balsam of Peru (BP), fragrance mix (FM), parthenium and paraben mix were taken from the Indian Standard Series [5] (Systopic India Ltd., New Delhi, India). Sulphacetamide (10% aqueous), chlorhexidine gluconate (0.2% aqueous) and tretinoin (0.025% cream) were tested as such from commercial preparations. The chemicals of other antigens were procured from Himedia Laboratories Pvt. Ltd. Mumbai India and oral drugs were taken from commercially available tablet forms. Antigens were then prepared in the departmental laboratory in standard concentrations with petrolatum as the vehicle. Paraben mix included in this series is used as a preservative in tretinoin cream. All the allergens were stored at 2-8ºC. In addition, the patients were also patch/photopatch tested with articles of daily use as and when these were suspected to have caused photodermatitis. The patch test units were applied as per the standard procedure in two sets and were kept covered with a radioopaque sheet. After 48 h, one set of patches was removed and exposed to 10 J/cm 2 of UVA (tubes from Philips Holland - TL/10R with dosimeter calibration). After irradiation, the other set of patches was also removed and both the sites were then covered again with the opaque sheet and the patient was asked to come after another 48 h for reading. Readings were taken at 48 and 96 h in all patients and, if needed, at 120 h for reading of the late reaction. Patch test results were graded according to the International Contact Dermatitis Research Group criteria. [5] Photopatch test results were interpreted according to the criteria shown in [Table - 2]. Photo-aggravated reactions are interpreted as contact allergy with photoaggravation while photo-augmented reactions signify both contact and photocontact allergy. The relevance of the patch and photopatch test results was defined as "definite" if the reaction is positive to the patch test allergen, object or product containing the suspected allergen; "probable" if the substance identified by the patch test could be verified as present in the known skin contactants; "possible" if the patient is exposed to circumstances in which skin contact with the material known to contain the putative allergen likely occurred; "past" if a positive patch test reaction could be explained by a previous and unrelated episode of contact dermatitis; and "unknown" if there is no evidence of relevance even after extensive investigations. Results These 30 patients (M:F, 23:7) were between 19 and 76 years of age, and the majority 16 (53%) were in the age group of 41-60 years [Table - 3]. All patients were engaged in various occupations that involved working outdoors some or the other time in the sun, and had a characteristic clinical picture of photodermatitis for the duration varying from 12 days to 30 years with remissions and relapses. Five (16.67%) patients showed generalized body involvement. Twenty-three (77%) patients presented within 5 years while seven (23%) patients had dermatitis for >5 years at the time of presentation. All patients except one had history of exacerbation of dermatitis few minutes to 4 h after sun exposure. The exacerbating factors were: summer season in 15 (50%) patients, insecticides spraying in three (10%) and exposure to parthenium plant in 10 (33.33%). History of drug intake prior to dermatitis was present in five (16.66%) patients (paracetamol, nimesulide, anti-tubercular drugs and tetracycline), although there was no definite history of aggravation of dermatitis with these drugs. Use of hair colorants and cement aggravated dermatitis in two (6.67%) and one (3.33%) patients, respectively. Forty-three positive test reactions were observed to 18 antigens in 22 (73.33%) subjects [Table - 4a & b]. FM was the most common contact allergen (nine patients). Of these nine patients, one showed photocontact allergy after 96 h while three showed photoaggravation. PPD was the next common allergen (six patients), with two patients showing photoaggravation and one exhibiting photoaugmentation. Parthenium hysterophorus showed positive patch test reactions in five (16.67%), with two and one patients exhibiting photo-aggravated and photo-augmented reactions, respectively. Among the pesticides/insecticides group, mancozeb, hexaconazole, captan and proparagite exhibited contact sensitivity in three, two, two and one patients, respectively. One patient exhibited a definite photoallergy to captan while one each showed photo-augmented reactions to hexaconazole and propargite. Positive photopatch tests were definitely relevant in nine (30%) patients and of probable relevance in one. Two controls, both females, were sensitive to tretinoin and FM, but exhibited no photosensitivity. Discussion The clinicodemographic profile of our patients of photodermatitis does not differ from what is already reported in the literature. [6],[7],[8],[9],[10],[11] Clinically relevant positive photopatch tests have been observed in 4-20% of the patients in previous studies [1],[4] as compared with 30% in our study. However, this being a small study, the overall prevalence of photoallergens in the population cannot be interpreted. Exposure to FM occurs commonly through cosmetics and toiletries, food items, other household products (room fresheners, waxes, polishes and insect repellents) and industrial products like metal working fluids. It was the most common contact allergen (30%) in our study, with one (3%) subject having definite photocontact allergy and three (10%) showing a photo-aggravated reaction. Various other studies have also documented positivity, varying from 2 to 21%. [3],[4],[6],[7],[11],[12] Establishing the relevance of FM sensitivity is a difficult task. Most of our patients were using a multitude of products like detergents, soaps and cosmetics, and had a fair chance of developing contact sensitivity to FM. BP is generally included in standard screening patch test series as an indicator of fragrance sensitivity, and shows positive reactions in about 50% of the cases of fragrance allergy when tested with both. [7],[13] Positive photopatch test (phototoxic and photoallergic) results due to BP were ranging from 1.2 to 10.2% in various studies [6],[7],[14] as compared with one (3.33%) patient in our study. However, none of our patients had a concurrent positive patch test to FM and BP. Six (20%) patients showed contact allergy to PPD, with one of them having photo augmentation and two (7%) having photo aggravation. PPD is a constituent of cosmetic hair colorants, pharmaceuticals and rubber and has been implicated for photocontact sensitivity or persistent light reactions in sensitive individuals. LeVine [15] demonstrated a positive photopatch test to caine mix and PPD and UVA photosensitivity in a 61-year-old man having a recurrent, summer-exacerbated chronic dermatitis. However, PPD is not included for photopatch testing in most standard series. Our patients perhaps developed contact dermatitis/photo contact dermatitis/photoaggravation to PPD from hair colorants. In India, Parthenium hysterophorus is perhaps the most common cause of contact dermatitis/airborne contact dermatitis, with an element of photosensitivity in some cases. Photo contact dermatitis secondary to P. hysterophorus too has been reported. [16] Understandably, sensitivity to Parthenium is expected to be high due to its profuse and widespread growth and its high sensitizing property. However, its photosensitizing potential remains debatable. While Sharma et al.[17] could correlate P. hysterophorus causing photo contact allergy in four and photoaggravation in six patients, Srinivas et al.[18] did not observe any photosensitivity. In the present study, P. hysterophorus showed a positive patch test reaction in five (16.67%) patients, with one patient having a photo-augmented reaction and two patients showing photo-aggravated reactions. This perhaps signifies that some of these patients of Parthenium sensitivity may show contact allergy with photoaggravation or both, i.e. contact allergy and photo contact allergy. The photo component of Parthenium sensitivity might possibly be due to some allergens of Parthenium hitherto unrecognized or to some other additional allergens unrelated to Parthenium. Two (6.67%) patients each showed a positive patch test reaction to tetrachlorosalicylanilide (TCSA) and chlorhexidine gluconate, respectively. Although during the 1960s various studies [19],[20] showed TCSA as an important photo contact sensitizer among soap dermatitis patients, Wilkinson [21] observed no reactions in normal persons. Withdrawal of TCSA from soaps subsequently resulted in a decline of the photosensitivity. Similarly, the incidence of contact sensitivity to chlorhexidine is quite low. [6],[7],[11] Contact sensitivity to octylmethoxy cinnamate, benzophenone-3, benzophenone-4, potassium dichromate, dicholorophene, triclosan, paraben mix and tretinoin was observed in one (3.33%) patient each. Among the various topical sunscreens, contact and photo contact allergy to para-aminobenzoic acid and its esters [2],[4],[22] has reduced considerably while benzophenone [9],[23],[24] is being observed as a frequent photoallergen. Only one patient each showed contact sensitivity to benzophenone-3, benzophenone-4 and octylmethoxy cinnamate without photoallergy or photoaggravation in the present study. Potassium dichromate is not a known photo contact sensitizer, [14],[25] although it is a common contact sensitizer. It gave a photo-augmented reaction in one of our patients, which needs to be emphasized. The incidence of photo contact allergy to dichlorophene, triclosan and parabens is infrequent, and so are our observations. Clinically, tretinoin often produces irritant reactions with photoaggravation, but is not a component of the standard photopatch test series. Not many studies on its photosensitizing potential are available. We had only one (3.33%) patient showing contact allergy to it without any photoaggravation. However, large studies are needed to determine its actual contact and photo contact sensitizing properties. [26],[27] Significant positive patch test reactions to the patient′s own articles/allergens were to mancozeb (three patients), hexaconazole and captan (two patients each) and proparagite (one patient). These were obtained in three farmers having a definite history of aggravation of their dermatitis after exposure to insecticides/pesticides. Photo contact allergy to captan in one patient and photo-augmented reaction to hexaconazole and proparagite in two other patients were significant observations in the present study. Although there is paucity of data on this, positive photopatch test reactions to captan have been observed by Mark et al. [28] The North American Contact Dermatitis Group recommends inclusion of thiourea rubber accelerators in the standard photopatch test battery. [29] However, none of our patients showed any type of reactivity to thiourea. Anti-histaminic drugs like promethazine, diphenhydramine, chlorpromazine and fentichlor have been reported to be the common photo contact sensitizers, with 2-15.8% positivity. [6],[7],[11],[12] However, Sharma et al.[17] did not observe any positive reaction to these drugs. Some of the systemically administered non-steroidal anti-inflammatory drugs, especially ketoprofen, ibuprofen, diclofenac and piroxicam, were also the common photo contact sensitizers in a multicentric photopatch test study. [30] Similarly, hydrochlorthiazide, a diuretic and commonly used anti-hypertensive, is a well-known photosensitizer, especially in patients sensitive to sulphonamides. [31] Flouroquinolones too can cause phototoxic reactions. [32],[33] In the present study, none of the patients showed any contact or photo contact allergy to any of the systemic drugs patch tested, signifying a dissociation between photosensitivity following ingestion of drugs and contact photosensitivity. Polysensitivity was observed in 13 (43.33%) patients who showed sensitivity to ≥2 allergens; one patient had sensitivity to a maximum of five patch test allergens. Such multiple positive patch test reactions perhaps occur because of either cross-reactivity, simultaneous exposure to multiple antigens in predisposed individuals or non-specific hyperreactivity. However, none of these allergens showed any photoallergic reactions. Conclusions Interpretation and evaluation of relevance of a positive patch-/photopatch test reaction is difficult and intricate. This is evident as we could establish an overall relevance in only 66% of the cases, although relevance in photopatch test-positive patients was high (90%). We feel that insecticides/pesticides need to be studied more comprehensively for their sensitizing and photosensitizing potentials as their exposure, especially inadvertent, is quite frequent in our Indian population. We also feel that a photopatch test tray needs to integrate relevant photosensitizers of past and of today as well as those predicted to be relevant in the future, and need continuous updating. References
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 2, March-April, 2011, pp. 148-155 Original Article Evaluation of photopatch test allergens for Indian patients of photodermatitis: Preliminary results Nidhi Jindal1, Nand Lal Sharma2, Vikram Kumar Mahajan2, Vinay Shanker1, Gita Ram Tegta1, Ghanshyam Kumar Verma1 1 Department of Dermatology, Venereology and Leprosy, Indira Gandhi Medical College, Shimla, India Correspondence Address: Nand Lal Sharma, Department of Dermatology and Venereology, RPGMC, Kangra (Tanda), Himachal Pradesh, India, nandlals@hotmail.com Code Number: dv11043 PMID: 21393943 DOI: 10.4103/0378-6323.77453 Abstract Background: There is a strong need to develop a photopatch test tray suitable for Indian patients of photodermatitis as European/Scandinavian photopatch test trays may not be wholly relevant for them.Aim: We carried out this study using photoallergens relevant in the Indian context to determine their relevance in patients of photodermatitis. Methods: Thirty patients (M:F, 23:7) between 19 and 76 years of age of photodermatitis and 10 controls were patch- and photopatch tested with 20 common photoallergens. In addition, the patients were also (photo) patch tested with articles of daily use as and when these were suspected to be the cause. Results: Forty-three positive reactions to one or more antigens were seen in 22 (74%) patients. Fourteen positive photopatch tests to seven allergens were observed in 10 (33%) patients, and nine (30%) of them had a definite relevance. The most common contact allergen was fragrance mix (FM) (30%), followed by p-phenylenediamine (20%) and Parthenium hysterophorous (17%). The definite relevance of the patch- and photopatch tests could be correlated in 47% of these patients. Conclusions: FM is the most common contact and photocontact allergen among the various photopatch test antigens. Although differences in technique and evaluation make direct comparison between different centers difficult, still photopatch testing remains an integral part and gold standard for the work-up of the photosensitive patients. Keywords: Photo dermatitis, photopatch test, captan, fragrance mix Introduction Photosensitivity is a poorly understood cutaneous reaction to sunlight probably involving the immune system. Photoallergic dermatitis is caused by direct contact of skin with the causative agent and subsequent exposure to light of a certain wavelength. The common photosensitizing agents include chemicals used in sunscreens, antiseptic agents, fragrances and non-steroidal anti-inflammatory agents. A thorough history, especially of evolution of symptoms and of photoaggravation combined with photopatch testing, is an effective approach for the diagnosis of photodermatitis or unclear photoreactions that cannot be associated with genuine photodermatoses. Photopatch testing helps in determining the sensitizing potentials of commonly used agents. Recommendations differ widely across the various photodermatitis research groups, and include variations in test procedures and interpretation, the range of tests substances, the irradiation doses, the precise irradiating wavelengths, the timing of irradiation, the irradiance used and the delay before reading of results. [1],[2],[3] Despite these variations, approximately 4-20% of the patients who undergo photopatch testing have clinically relevant positive results, eventuating in the diagnosis of photoallergic contact dermatitis. [1],[4] There is no Indian standard photopatch test series available, and few studies carried out in India have used European/Scandinavian photo patch test trays, which may not be wholly relevant for Indian patients. Hence, there is a strong need to develop a photopatch test tray suitable for Indian patients of photodermatitis. In this study, we present the preliminary results of photopatch testing using allergens relevant in the Indian context and their relevance in the Indian patients of photodermatitis. Methods Thirty consecutive patients (excluding pregnant/lactating females and children aged <18 years) of clinically diagnosed photodermatitis attending the Outpatient Dermatology Department were patch tested between July 2008 and June 2009. Other exclusion criteria included any systemic or congenital disorder and idiopathic photodermatoses known for photosensitivity. Patients having acute dermatitis were enrolled after the acute episode subsided or when the dose of prednisolone was <20 mg/d. Clinical details regarding age, sex, occupation, duration and progress of dermatitis, aggravating factors for photoaggravation and treatment (topical or systemic, particularly photosensitizing drugs) taken were recorded and lesions were charted. Ten subjects were also selected as controls from patients having minor dermatoses other than dermatitis or photodermatitis. The patch test antigens comprising 20 common photoallergens [Table - 1] were photopatch tested by the Finn Chamber method after obtaining written consent. Para-phenylenediamine (PPD), balsam of Peru (BP), fragrance mix (FM), parthenium and paraben mix were taken from the Indian Standard Series [5] (Systopic India Ltd., New Delhi, India). Sulphacetamide (10% aqueous), chlorhexidine gluconate (0.2% aqueous) and tretinoin (0.025% cream) were tested as such from commercial preparations. The chemicals of other antigens were procured from Himedia Laboratories Pvt. Ltd. Mumbai India and oral drugs were taken from commercially available tablet forms. Antigens were then prepared in the departmental laboratory in standard concentrations with petrolatum as the vehicle. Paraben mix included in this series is used as a preservative in tretinoin cream. All the allergens were stored at 2-8ºC. In addition, the patients were also patch/photopatch tested with articles of daily use as and when these were suspected to have caused photodermatitis. The patch test units were applied as per the standard procedure in two sets and were kept covered with a radioopaque sheet. After 48 h, one set of patches was removed and exposed to 10 J/cm 2 of UVA (tubes from Philips Holland - TL/10R with dosimeter calibration). After irradiation, the other set of patches was also removed and both the sites were then covered again with the opaque sheet and the patient was asked to come after another 48 h for reading. Readings were taken at 48 and 96 h in all patients and, if needed, at 120 h for reading of the late reaction. Patch test results were graded according to the International Contact Dermatitis Research Group criteria. [5] Photopatch test results were interpreted according to the criteria shown in [Table - 2]. Photo-aggravated reactions are interpreted as contact allergy with photoaggravation while photo-augmented reactions signify both contact and photocontact allergy. The relevance of the patch and photopatch test results was defined as "definite" if the reaction is positive to the patch test allergen, object or product containing the suspected allergen; "probable" if the substance identified by the patch test could be verified as present in the known skin contactants; "possible" if the patient is exposed to circumstances in which skin contact with the material known to contain the putative allergen likely occurred; "past" if a positive patch test reaction could be explained by a previous and unrelated episode of contact dermatitis; and "unknown" if there is no evidence of relevance even after extensive investigations. Results These 30 patients (M:F, 23:7) were between 19 and 76 years of age, and the majority 16 (53%) were in the age group of 41-60 years [Table - 3]. All patients were engaged in various occupations that involved working outdoors some or the other time in the sun, and had a characteristic clinical picture of photodermatitis for the duration varying from 12 days to 30 years with remissions and relapses. Five (16.67%) patients showed generalized body involvement. Twenty-three (77%) patients presented within 5 years while seven (23%) patients had dermatitis for >5 years at the time of presentation. All patients except one had history of exacerbation of dermatitis few minutes to 4 h after sun exposure. The exacerbating factors were: summer season in 15 (50%) patients, insecticides spraying in three (10%) and exposure to parthenium plant in 10 (33.33%). History of drug intake prior to dermatitis was present in five (16.66%) patients (paracetamol, nimesulide, anti-tubercular drugs and tetracycline), although there was no definite history of aggravation of dermatitis with these drugs. Use of hair colorants and cement aggravated dermatitis in two (6.67%) and one (3.33%) patients, respectively. Forty-three positive test reactions were observed to 18 antigens in 22 (73.33%) subjects [Table - 4a & b]. FM was the most common contact allergen (nine patients). Of these nine patients, one showed photocontact allergy after 96 h while three showed photoaggravation. PPD was the next common allergen (six patients), with two patients showing photoaggravation and one exhibiting photoaugmentation. Parthenium hysterophorus showed positive patch test reactions in five (16.67%), with two and one patients exhibiting photo-aggravated and photo-augmented reactions, respectively. Among the pesticides/insecticides group, mancozeb, hexaconazole, captan and proparagite exhibited contact sensitivity in three, two, two and one patients, respectively. One patient exhibited a definite photoallergy to captan while one each showed photo-augmented reactions to hexaconazole and propargite. Positive photopatch tests were definitely relevant in nine (30%) patients and of probable relevance in one. Two controls, both females, were sensitive to tretinoin and FM, but exhibited no photosensitivity. Discussion The clinicodemographic profile of our patients of photodermatitis does not differ from what is already reported in the literature. [6],[7],[8],[9],[10],[11] Clinically relevant positive photopatch tests have been observed in 4-20% of the patients in previous studies [1],[4] as compared with 30% in our study. However, this being a small study, the overall prevalence of photoallergens in the population cannot be interpreted. Exposure to FM occurs commonly through cosmetics and toiletries, food items, other household products (room fresheners, waxes, polishes and insect repellents) and industrial products like metal working fluids. It was the most common contact allergen (30%) in our study, with one (3%) subject having definite photocontact allergy and three (10%) showing a photo-aggravated reaction. Various other studies have also documented positivity, varying from 2 to 21%. [3],[4],[6],[7],[11],[12] Establishing the relevance of FM sensitivity is a difficult task. Most of our patients were using a multitude of products like detergents, soaps and cosmetics, and had a fair chance of developing contact sensitivity to FM. BP is generally included in standard screening patch test series as an indicator of fragrance sensitivity, and shows positive reactions in about 50% of the cases of fragrance allergy when tested with both. [7],[13] Positive photopatch test (phototoxic and photoallergic) results due to BP were ranging from 1.2 to 10.2% in various studies [6],[7],[14] as compared with one (3.33%) patient in our study. However, none of our patients had a concurrent positive patch test to FM and BP. Six (20%) patients showed contact allergy to PPD, with one of them having photo augmentation and two (7%) having photo aggravation. PPD is a constituent of cosmetic hair colorants, pharmaceuticals and rubber and has been implicated for photocontact sensitivity or persistent light reactions in sensitive individuals. LeVine [15] demonstrated a positive photopatch test to caine mix and PPD and UVA photosensitivity in a 61-year-old man having a recurrent, summer-exacerbated chronic dermatitis. However, PPD is not included for photopatch testing in most standard series. Our patients perhaps developed contact dermatitis/photo contact dermatitis/photoaggravation to PPD from hair colorants. In India, Parthenium hysterophorus is perhaps the most common cause of contact dermatitis/airborne contact dermatitis, with an element of photosensitivity in some cases. Photo contact dermatitis secondary to P. hysterophorus too has been reported. [16] Understandably, sensitivity to Parthenium is expected to be high due to its profuse and widespread growth and its high sensitizing property. However, its photosensitizing potential remains debatable. While Sharma et al.[17] could correlate P. hysterophorus causing photo contact allergy in four and photoaggravation in six patients, Srinivas et al.[18] did not observe any photosensitivity. In the present study, P. hysterophorus showed a positive patch test reaction in five (16.67%) patients, with one patient having a photo-augmented reaction and two patients showing photo-aggravated reactions. This perhaps signifies that some of these patients of Parthenium sensitivity may show contact allergy with photoaggravation or both, i.e. contact allergy and photo contact allergy. The photo component of Parthenium sensitivity might possibly be due to some allergens of Parthenium hitherto unrecognized or to some other additional allergens unrelated to Parthenium. Two (6.67%) patients each showed a positive patch test reaction to tetrachlorosalicylanilide (TCSA) and chlorhexidine gluconate, respectively. Although during the 1960s various studies [19],[20] showed TCSA as an important photo contact sensitizer among soap dermatitis patients, Wilkinson [21] observed no reactions in normal persons. Withdrawal of TCSA from soaps subsequently resulted in a decline of the photosensitivity. Similarly, the incidence of contact sensitivity to chlorhexidine is quite low. [6],[7],[11] Contact sensitivity to octylmethoxy cinnamate, benzophenone-3, benzophenone-4, potassium dichromate, dicholorophene, triclosan, paraben mix and tretinoin was observed in one (3.33%) patient each. Among the various topical sunscreens, contact and photo contact allergy to para-aminobenzoic acid and its esters [2],[4],[22] has reduced considerably while benzophenone [9],[23],[24] is being observed as a frequent photoallergen. Only one patient each showed contact sensitivity to benzophenone-3, benzophenone-4 and octylmethoxy cinnamate without photoallergy or photoaggravation in the present study. Potassium dichromate is not a known photo contact sensitizer, [14],[25] although it is a common contact sensitizer. It gave a photo-augmented reaction in one of our patients, which needs to be emphasized. The incidence of photo contact allergy to dichlorophene, triclosan and parabens is infrequent, and so are our observations. Clinically, tretinoin often produces irritant reactions with photoaggravation, but is not a component of the standard photopatch test series. Not many studies on its photosensitizing potential are available. We had only one (3.33%) patient showing contact allergy to it without any photoaggravation. However, large studies are needed to determine its actual contact and photo contact sensitizing properties. [26],[27] Significant positive patch test reactions to the patient′s own articles/allergens were to mancozeb (three patients), hexaconazole and captan (two patients each) and proparagite (one patient). These were obtained in three farmers having a definite history of aggravation of their dermatitis after exposure to insecticides/pesticides. Photo contact allergy to captan in one patient and photo-augmented reaction to hexaconazole and proparagite in two other patients were significant observations in the present study. Although there is paucity of data on this, positive photopatch test reactions to captan have been observed by Mark et al. [28] The North American Contact Dermatitis Group recommends inclusion of thiourea rubber accelerators in the standard photopatch test battery. [29] However, none of our patients showed any type of reactivity to thiourea. Anti-histaminic drugs like promethazine, diphenhydramine, chlorpromazine and fentichlor have been reported to be the common photo contact sensitizers, with 2-15.8% positivity. [6],[7],[11],[12] However, Sharma et al.[17] did not observe any positive reaction to these drugs. Some of the systemically administered non-steroidal anti-inflammatory drugs, especially ketoprofen, ibuprofen, diclofenac and piroxicam, were also the common photo contact sensitizers in a multicentric photopatch test study. [30] Similarly, hydrochlorthiazide, a diuretic and commonly used anti-hypertensive, is a well-known photosensitizer, especially in patients sensitive to sulphonamides. [31] Flouroquinolones too can cause phototoxic reactions. [32],[33] In the present study, none of the patients showed any contact or photo contact allergy to any of the systemic drugs patch tested, signifying a dissociation between photosensitivity following ingestion of drugs and contact photosensitivity. Polysensitivity was observed in 13 (43.33%) patients who showed sensitivity to ≥2 allergens; one patient had sensitivity to a maximum of five patch test allergens. Such multiple positive patch test reactions perhaps occur because of either cross-reactivity, simultaneous exposure to multiple antigens in predisposed individuals or non-specific hyperreactivity. However, none of these allergens showed any photoallergic reactions. Conclusions Interpretation and evaluation of relevance of a positive patch-/photopatch test reaction is difficult and intricate. This is evident as we could establish an overall relevance in only 66% of the cases, although relevance in photopatch test-positive patients was high (90%). We feel that insecticides/pesticides need to be studied more comprehensively for their sensitizing and photosensitizing potentials as their exposure, especially inadvertent, is quite frequent in our Indian population. We also feel that a photopatch test tray needs to integrate relevant photosensitizers of past and of today as well as those predicted to be relevant in the future, and need continuous updating. References
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11043t1.jpg] [dv11043t3.jpg] [dv11043t2.jpg] [dv11043t4b.jpg] [dv11043t4a.jpg] |
| |||||||||


![[Table - 1]](../photo/dv11043t1.jpg){kind=link}
![[Table - 2]](../photo/dv11043t2.jpg){kind=link}
![[Table - 3]](../photo/dv11043t3.jpg){kind=link}
{kind=link}
{kind=link}
![[Table - 1]](/showimage?dv/photo/dv11043t1.jpg){kind=link}
![[Table - 2]](/showimage?dv/photo/dv11043t2.jpg){kind=link}
![[Table - 3]](/showimage?dv/photo/dv11043t3.jpg){kind=link}
{kind=link}
{kind=link}