 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
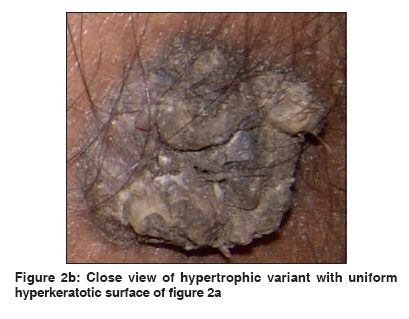
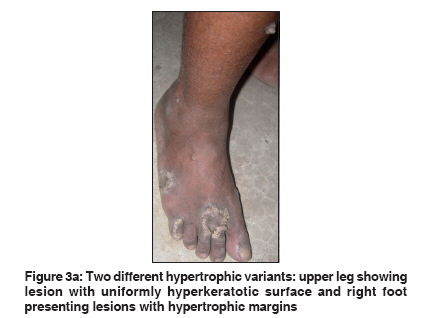
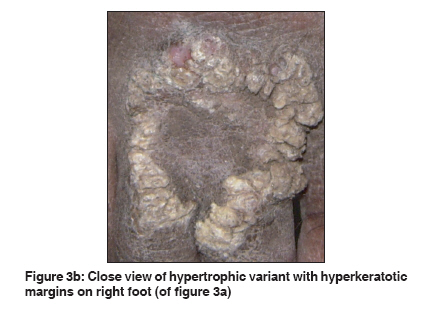
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 2, March-April, 2011, pp. 199-202 Letter to the Editor Different morphological variants of hypertrophic porokeratosis and disseminated lesions of porokeratosis of Mibelli: A rare co-existence Sankha Koley1, Jyotirindranath Sarkar1, Sanjiv Choudhary2, Suparna Dhara1, Manoj Choudhury3, Swagata Bhattacharya3 1 Department of Dermatology, Bankura Sammilani Medical College, West Bengal, India Correspondence Address: Sankha Koley, Subhankar Sarani, Bankura - 722 101, West Bengal, India, skoley@gmail.com Code Number: dv11057 PMID: 21393956 DOI: 10.4103/0378-6323.77467 Sir, Porokeratosis (PK) is a rare genodermatosis of abnormal epidermal keratinization. The etiology is unknown with varying presentation and an unpredictable outcome. Coexistence of the different variants of PK is seldom noted. Disseminated lesions of PK of Mibelli are considered to be very rare. [1] Hypertrophic verrucous type of PK may present in two ways: the whole surface may be hyperkeratotic or the hypertrophy may be localized only to periphery. We report two different presentations of hypertrophic verrucous PK in association with disseminated chronic plaque type in the same patient. A 46-years-old male patient presented with multiple asymptomatic lesions on the body since last 20 years. The lesions were gradually progressive in size and number. Initially all the lesions were small with smooth surfaces. With years, some of them on legs had become large with rough, verrucous surfaces. Close examination revealed well-defined, annular, oval or irregular shaped lesions with raised margin and central atrophy on bilateral hands and trunk [Figure - 1]. Each lesion was 1 to 4 cm in diameter and along the margin, there was a prominent deep furrow. The lesions were distributed on the exposed as well as covered areas. There was a hyperpigmented plaque (2 to 3 cm in diameter) with uniform verrucous surface on the medial side of either leg [Figure - 2a and b]. On the dorsum of the right foot, there were three plaques (4 to 6 cm in diameter) with gross hypertrophic verrucous surface confined to the periphery [Figure - 3a and b]. The central part of the lesions showed clinically normal skin in most lesions. Considering the clinical presentation, we diagnosed these lesions as disseminated lesions of porokeratosis of Mibelli and different morphological presentations of hypertrophic verrucous type of PK. Biopsy was done from all these three types of lesions; one from margin of annular plaque of right arm, [Figure - 4] one from periphery of uniformly verrucous surfaced plaque of right leg and one from the well-defined verrucous margin of a lesion on dorsum of right foot. Histology of all the lesions was characterized by epidermal invagination with cornoid lamella; consistent with the findings of PK. Granular layer was absent below the invagination and upper dermis showed lichenoid infiltrate [Figure - 4]. The verrucous lesions over the leg and foot revealed columns of severe hyperkeratosis. Since the first description of ′porokeratosis′ by Vittorio Mibelli in 1893, many variants of PK have been reported. The different types of PK are differentiated purely on clinical criteria. Classically, five clinical variants are recognized: classic porokeratosis of Mibelli, disseminated superficial (actinic and non actinic type) PK, porokeratosis palmaris et plantaris disseminata, linear PK and punctate PK. Apart from these five variants, a number of morphological forms, like facial PK, giant PK, hypertrophic verrucous porokeratosis, reticulate PK have been reported in the literature. [2] With the exception of the punctate type, it is characterized by a keratotic ridge that corresponds histologically by the presence of cornoid lamella. [1] Mibelli originally described the plaque type variety in large lesions which were limited in number, with prominent raised walls and distinct furrows. [3] In contrast, in the disseminated superficial form, the lesions are smaller, more in number, and have only minimally raised, less hyperkeratotic border. Among the atypical presentations, few cases of hypertrophic, verrucous, or nodular porokeratosis have been reported. [4] In most of them, the whole lesions are keratotic and nodular. Although they may be found in all parts of body, most of them are localized to the buttocks and mimics psoriasis. [5] In the other rarer variant, hypertrophy may be confined to the margins. Interestingly, the first Indian case report describing this variant was made from our institution. [6] Recently Sarma et al, [7] reported development of multiple horns in the marginal areas due to extreme hypertrophy. Mukhopadhyay [8] reported simultaneous occurrence of disseminated superficial, linear and hypertrophic verrucous perianal forms of PK in a child.Simultaneous presentation of different types of PK in the same patient and their similar histology imply that variation in clinical presentations may be due to the different phenotypic expressions of a common genetic abnormality or may be the consequence of abnormalities in closely linked genetic loci or genes. The pathogenesis of PK is unknown. An autosomal mode of inheritance with variable penetrance has been described. But sporadic cases, as in the present patient, may also occur. The different trigger factors are ultraviolet radiation, electron beam therapy, radiation therapy and immunosuppression. Malignancy, although rare, has been reported in almost all forms of PK. Larger lesion, especially of the giant variety of PK, is most frequently reported to produce malignancy like squamous cell carcinoma, Bowen′s disease, basal cell carcinoma, diffuse large B-cell lymphoma, etc. The clinical features of hyperkeratotic lesions on the legs and the right foot resembled psoriasis and lupus vulgaris. But presence of classical lesions of PK on bilateral hands and trunk helped us to clinch the diagnosis. As far as we know, simultaneous presentation of two different types of hypertrophic verrucous type of porokeratosis in the same patient has never been reported before. Interestingly, disseminated lesions of the porokeratosis of Mibelli were also noted in the same patient. References
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 2, March-April, 2011, pp. 199-202 Letter to the Editor Different morphological variants of hypertrophic porokeratosis and disseminated lesions of porokeratosis of Mibelli: A rare co-existence Sankha Koley1, Jyotirindranath Sarkar1, Sanjiv Choudhary2, Suparna Dhara1, Manoj Choudhury3, Swagata Bhattacharya3 1 Department of Dermatology, Bankura Sammilani Medical College, West Bengal, India Correspondence Address: Sankha Koley, Subhankar Sarani, Bankura - 722 101, West Bengal, India, skoley@gmail.com Code Number: dv11057 PMID: 21393956 DOI: 10.4103/0378-6323.77467 Sir, Porokeratosis (PK) is a rare genodermatosis of abnormal epidermal keratinization. The etiology is unknown with varying presentation and an unpredictable outcome. Coexistence of the different variants of PK is seldom noted. Disseminated lesions of PK of Mibelli are considered to be very rare. [1] Hypertrophic verrucous type of PK may present in two ways: the whole surface may be hyperkeratotic or the hypertrophy may be localized only to periphery. We report two different presentations of hypertrophic verrucous PK in association with disseminated chronic plaque type in the same patient. A 46-years-old male patient presented with multiple asymptomatic lesions on the body since last 20 years. The lesions were gradually progressive in size and number. Initially all the lesions were small with smooth surfaces. With years, some of them on legs had become large with rough, verrucous surfaces. Close examination revealed well-defined, annular, oval or irregular shaped lesions with raised margin and central atrophy on bilateral hands and trunk [Figure - 1]. Each lesion was 1 to 4 cm in diameter and along the margin, there was a prominent deep furrow. The lesions were distributed on the exposed as well as covered areas. There was a hyperpigmented plaque (2 to 3 cm in diameter) with uniform verrucous surface on the medial side of either leg [Figure - 2a and b]. On the dorsum of the right foot, there were three plaques (4 to 6 cm in diameter) with gross hypertrophic verrucous surface confined to the periphery [Figure - 3a and b]. The central part of the lesions showed clinically normal skin in most lesions. Considering the clinical presentation, we diagnosed these lesions as disseminated lesions of porokeratosis of Mibelli and different morphological presentations of hypertrophic verrucous type of PK. Biopsy was done from all these three types of lesions; one from margin of annular plaque of right arm, [Figure - 4] one from periphery of uniformly verrucous surfaced plaque of right leg and one from the well-defined verrucous margin of a lesion on dorsum of right foot. Histology of all the lesions was characterized by epidermal invagination with cornoid lamella; consistent with the findings of PK. Granular layer was absent below the invagination and upper dermis showed lichenoid infiltrate [Figure - 4]. The verrucous lesions over the leg and foot revealed columns of severe hyperkeratosis. Since the first description of ′porokeratosis′ by Vittorio Mibelli in 1893, many variants of PK have been reported. The different types of PK are differentiated purely on clinical criteria. Classically, five clinical variants are recognized: classic porokeratosis of Mibelli, disseminated superficial (actinic and non actinic type) PK, porokeratosis palmaris et plantaris disseminata, linear PK and punctate PK. Apart from these five variants, a number of morphological forms, like facial PK, giant PK, hypertrophic verrucous porokeratosis, reticulate PK have been reported in the literature. [2] With the exception of the punctate type, it is characterized by a keratotic ridge that corresponds histologically by the presence of cornoid lamella. [1] Mibelli originally described the plaque type variety in large lesions which were limited in number, with prominent raised walls and distinct furrows. [3] In contrast, in the disseminated superficial form, the lesions are smaller, more in number, and have only minimally raised, less hyperkeratotic border. Among the atypical presentations, few cases of hypertrophic, verrucous, or nodular porokeratosis have been reported. [4] In most of them, the whole lesions are keratotic and nodular. Although they may be found in all parts of body, most of them are localized to the buttocks and mimics psoriasis. [5] In the other rarer variant, hypertrophy may be confined to the margins. Interestingly, the first Indian case report describing this variant was made from our institution. [6] Recently Sarma et al, [7] reported development of multiple horns in the marginal areas due to extreme hypertrophy. Mukhopadhyay [8] reported simultaneous occurrence of disseminated superficial, linear and hypertrophic verrucous perianal forms of PK in a child.Simultaneous presentation of different types of PK in the same patient and their similar histology imply that variation in clinical presentations may be due to the different phenotypic expressions of a common genetic abnormality or may be the consequence of abnormalities in closely linked genetic loci or genes. The pathogenesis of PK is unknown. An autosomal mode of inheritance with variable penetrance has been described. But sporadic cases, as in the present patient, may also occur. The different trigger factors are ultraviolet radiation, electron beam therapy, radiation therapy and immunosuppression. Malignancy, although rare, has been reported in almost all forms of PK. Larger lesion, especially of the giant variety of PK, is most frequently reported to produce malignancy like squamous cell carcinoma, Bowen′s disease, basal cell carcinoma, diffuse large B-cell lymphoma, etc. The clinical features of hyperkeratotic lesions on the legs and the right foot resembled psoriasis and lupus vulgaris. But presence of classical lesions of PK on bilateral hands and trunk helped us to clinch the diagnosis. As far as we know, simultaneous presentation of two different types of hypertrophic verrucous type of porokeratosis in the same patient has never been reported before. Interestingly, disseminated lesions of the porokeratosis of Mibelli were also noted in the same patient. References
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11057f2a.jpg] [dv11057f1.jpg] [dv11057f2b.jpg] [dv11057f3a.jpg] [dv11057f4.jpg] [dv11057f3b.jpg] |
| |||||||||

![[Figure - 1]](../photo/dv11057f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[Figure - 4]](../photo/dv11057f4.jpg){kind=link}
![[Figure - 1]](/showimage?dv/photo/dv11057f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[Figure - 4]](/showimage?dv/photo/dv11057f4.jpg){kind=link}