 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
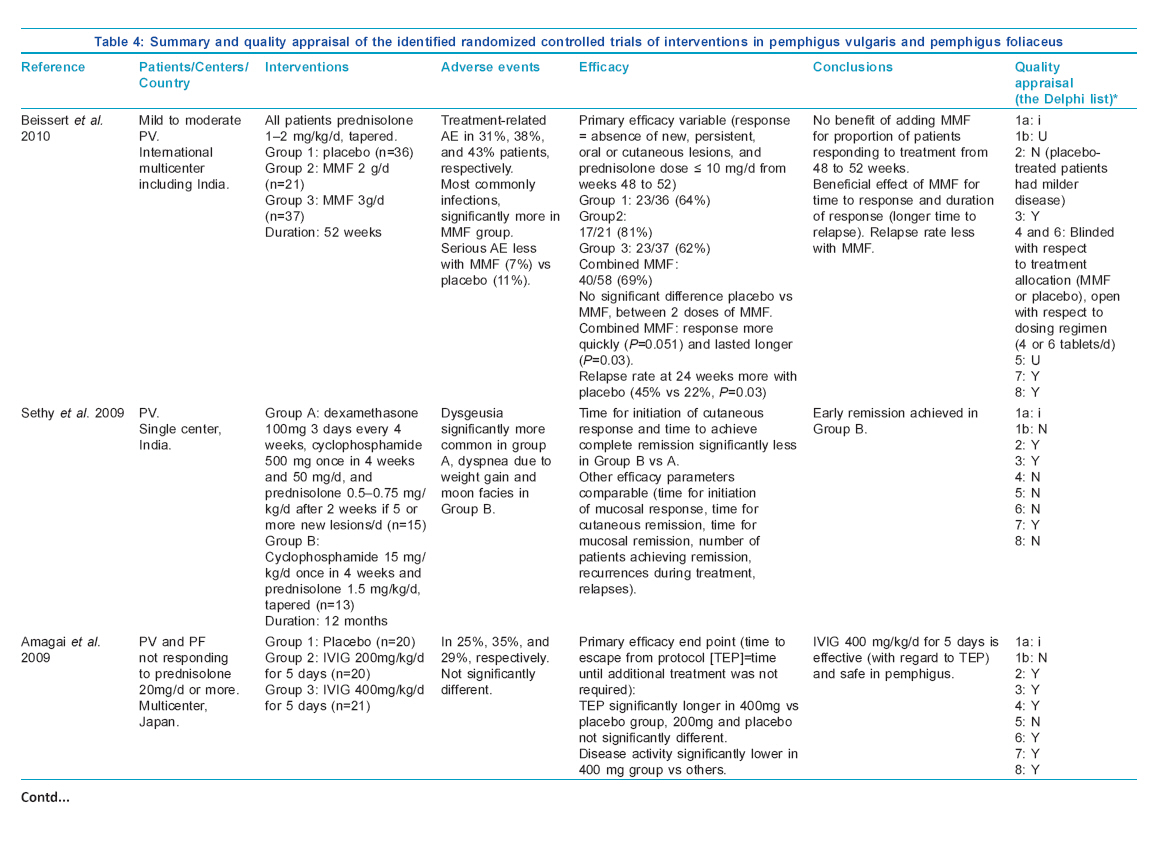
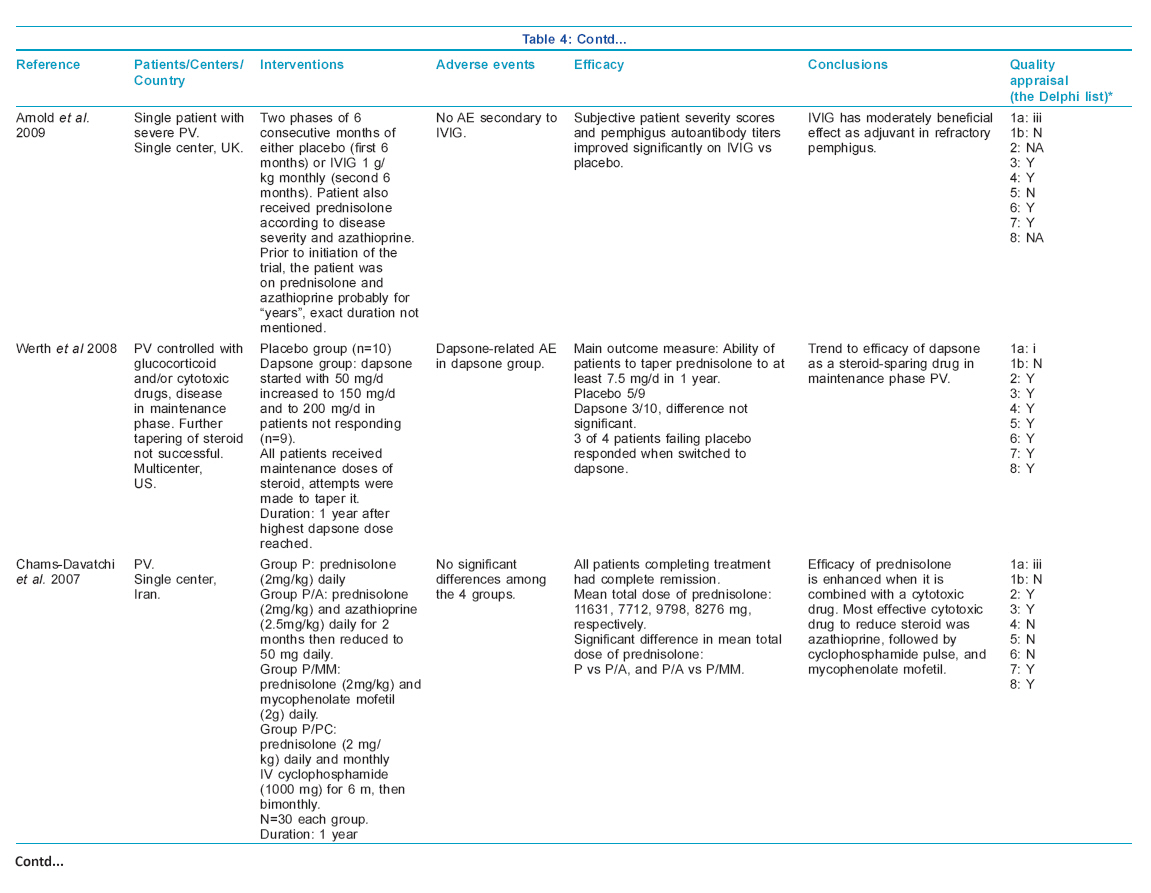
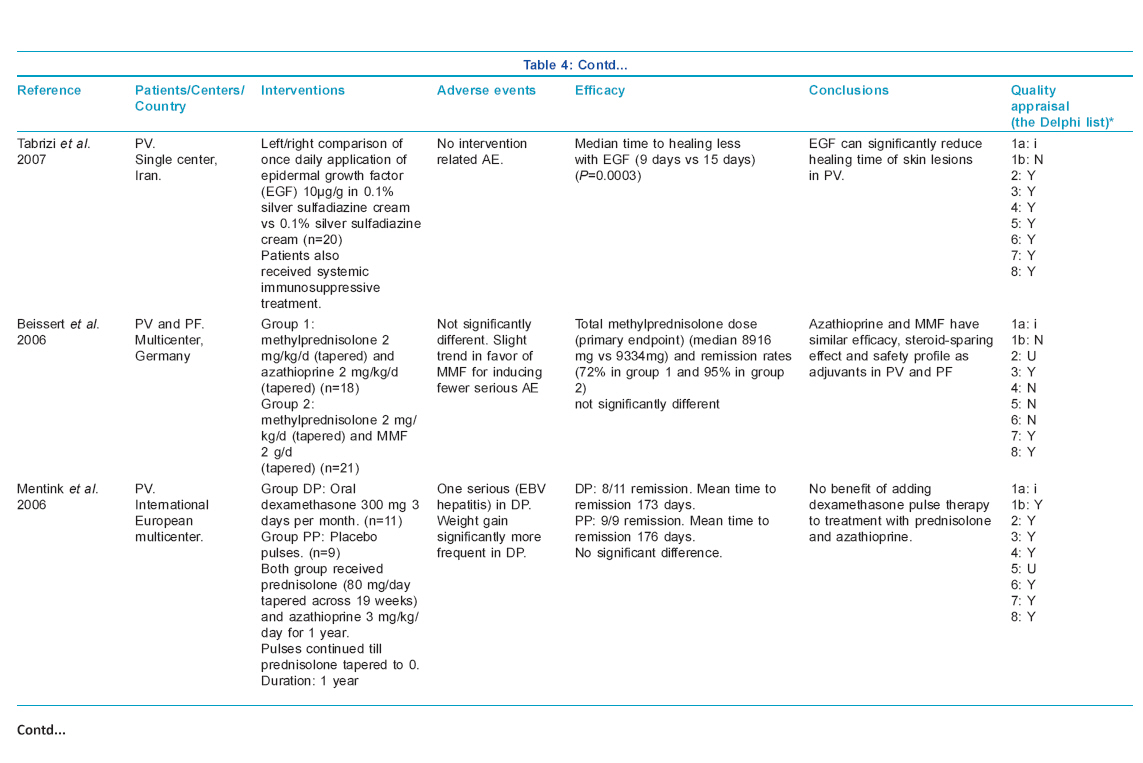
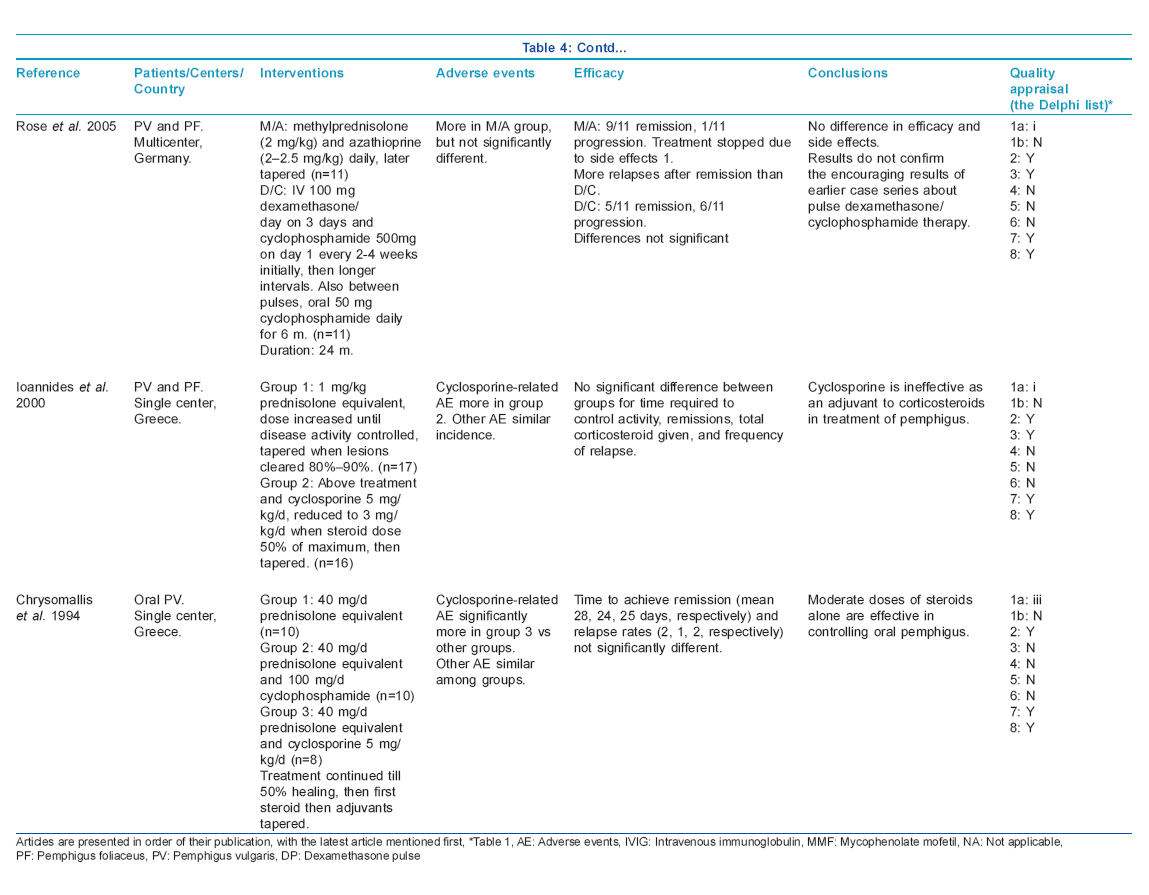
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 4, July-August, 2011, pp. 456-469 Original Article Evidence-based treatments for pemphigus vulgaris, pemphigus foliaceus, and bullous pemphigoid: A systematic review Sanjay Singh Department of Dermatology and Venereology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India Correspondence Address: Sanjay Singh C-23, Swastik Towers, Lanka, Varanasi, Uttar Pradesh India sanjaye2@gmail.com Code Number: dv11128 PMID: 21727693 DOI: 10.4103/0378-6323.82400 Abstract Background: Pemphigus, bullous pemphigoid, and epidermolysis bullosa acquisita are autoimmune diseases of skin associated with considerable morbidity and sometimes mortality. There is no cure for these diseases.Aims: To summarize evidence-based treatments for these diseases by performing a systematic review. Methods: The research protocol included the following steps: identification of databases to be searched, defining search strategy, searching the databases for references, first-stage screening of the abstracts, second-stage screening of full texts of articles identified after the first-stage screening, data extraction from the identified articles after second-stage screening, quality appraisal of the studies using the Delphi list, and summarizing the findings. Results: No randomized controlled trials of interventions in pemphigus vegetans, pemphigus erythematosus, and epidermolysis bullosa acquisita could be found. After the second-stage screening, 12 randomized controlled trials were analyzed, which included patients with pemphigus vulgaris or pemphigus vulgaris and pemphigus foliaceus, and 7 which included patients with bullous pemphigoid. Conclusions: Number of high-quality randomized controlled trials conducted on pemphigus and bullous pemphigoid is small. Oral corticosteroid along with a steroid-sparing agent appears to be the most effective treatment for pemphigus. Azathioprine may be most effective as a steroid-sparing agent. Topical corticosteroid therapy (as studied) is effective for bullous pemphigoid and appears to be superior to oral corticosteroid for extensive disease. Some suggestions about future research are made. Keywords: Bullous pemphigoid, evidence-based treatment, interventions, pemphigus, review, systematic review, treatment Introduction Pemphigus is a group of autoimmune diseases of skin and mucous membranes, which is characterized by autoantibodies directed against antigens desmogleins 1 and/or 3 in the epidermis. This results in acantholysis in epidermis and clinically in the formation of flaccid blisters. There are mainly two types of pemphigus, pemphigus vulgaris (and its variant pemphigus vegetans), and pemphigus foliaceus (and its variant pemphigus erythematosus). The diseases are associated with considerable morbidity and sometimes mortality. Use of systemic glucocorticoids and other immunosuppressive drugs has changed the outlook in a large proportion of patients, but presently there is no cure of pemphigus. Bullous pemphigoid is an autoimmune disease of skin usually occurring in the elderly. It is characterized by autoantibodies against the 180-kd (BP 180) and/or 230-kd (BP 230) molecules present in basal keratinocyte hemidesmosomes in the dermoepidermal junction. This results in split at the dermoepidermal junction and clinically in the formation of tense blisters. Pemphigoid is associated with considerable morbidity and sometimes mortality. Corticosteroids, topical or systemic, and sometimes other immunosuppressive agents help many patients, but presently there is no cure. Epidermolysis bullosa acquisita (EBA) is a rare autoimmune disease characterized by skin fragility and subepidermal blisters due to the formation of autoantibodies against type VII collagen within the anchoring fibrils at the dermoepidermal junctions. EBA is associated with considerable morbidity. In the present review, an attempt will be made to answer the question: what are the evidence-based (randomized controlled trials-based) treatments for pemphigus, bullous pemphigoid, and epidermolysis bullosa acquisita? Methods Pemphigus The research protocol included the following steps: identification of databases to be searched, defining search strategy, searching the databases for references, first-stage screening of the abstracts, second-stage screening of full texts of articles identified after the first-stage screening, data extraction from the identified articles after second-stage screening, quality appraisal of the studies, and summarizing the findings. Databases searched Following two databases were searched:
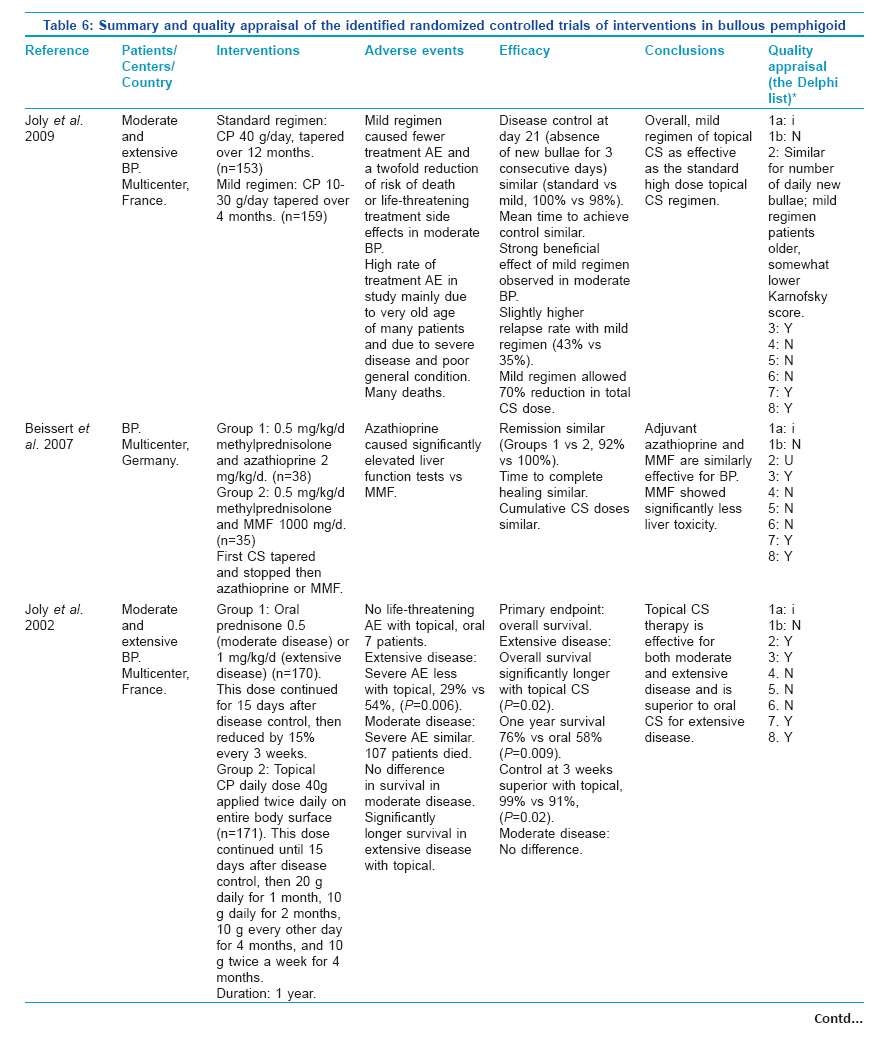
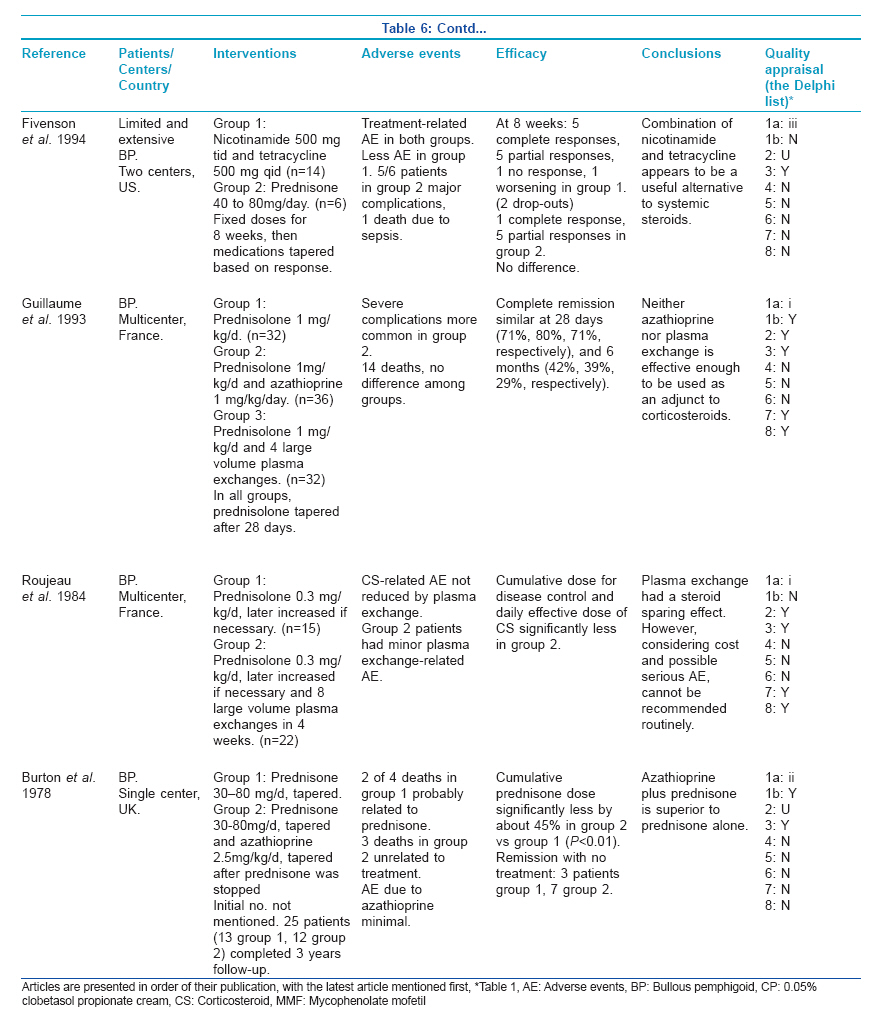
Search strategy 1. PubMed: This was searched for the phrases "pemphigus vulgaris," "pemphigus foliaceus," "pemphigus vegetans," and "pemphigus erythematosus" separately by activating the limit "Clinical Trial" and using the search field tag "Title/Abstract." 2. Cochrane Central Register of Controlled Trials: Search was performed for the above diseases separately in "Title, Abstract, or Keywords." The search was first performed on November 9, 2010 and was repeated on November 28, 2010; both searches resulted in identical references. All the articles thus identified went into first-stage screening. First-stage screening Abstracts of all the articles identified in the above-mentioned databases were read. Only those abstracts were selected for the second-stage screening, which met all of the following three inclusion criteria: (a) human trial, (b) prospective trial, and (c) controlled trial. Second-stage screening This was performed on the full-text articles. Full-texts of the articles which met the first-stage screening criteria were obtained. Only those articles were selected which met both of the following selection criteria: (a) mention of randomization in methods and (b) mention in methods that at least one of the following three tests were performed: (i) direct immunofluorescence test for detection of immunoglobulin G (IgG) on keratinocyte cell surface, (ii) test for detection of antibodies against desmoglein 1 and/or 3, or (iii) indirect immunofluorescence test for detecting IgG in patient′s serum, which binds the cell surface of normal keratinocytes. Articles that met the above-mentioned criteria were the randomized controlled trials (RCTs) of interventions in patients with pemphigus and these went into the data extraction stage. Data extraction Full-texts of the articles were read and the data regarding the following variables was noted separately for each article: name of disease(s) with which the patients were affected, number of centers where the trial was conducted and name of the country, interventions, adverse events, efficacy, and conclusions. Quality appraisal Quality appraisal of the RCTs was done by using the Delphi List, [1] which was expanded with respect to item number 1a as explained in the Discussion [Table - 1]. Summarizing the findings Summary of the RCTs was presented in tabular format. Bullous pemphigoid The same research protocol was followed as described above for pemphigus, with the following changes: Databases were searched for the word "pemphigoid." In the second-stage screening, only the articles that met both of the following selection criteria were selected: (a) mention of randomization in methods and (b) diagnosis of bullous pemphigoid by at least one of the following tests: (i) positive direct immunofluorescence test for C3 and/or IgG at the dermoepidermal junction, (ii) serum IgG labeling epidermal roof by indirect immunofluorescence, (iii) detection of antibodies against BP180 and/or BP230 antigens, or (iv) demonstration by immunoelectron microscopy of deposition of IgG associated with basal cell hemidesmosomes. Epidermolysis bullosa acquisita The same research protocol was followed as described above for pemphigus. Databases were searched for the phrase "epidermolysis bullosa acquisita." PubMed search resulted in three references which were excluded in first-stage screening. Search of Cochrane Central Register of Controlled Trials did not result in any reference. As no RCTs were available on epidermolysis bullosa acquisita, no RCT-based conclusions can be drawn about its treatment. Results Pemphigus Number of articles on pemphigus vulgaris selected at different stages of the review is shown in [Table - 2] and those related to other types of pemphigus in [Table - 3]. On reading the full-texts of articles, it became clear that no RCTs of interventions exclusively in pemphigus vegetans, pemphigus foliaceus, or pemphigus erythematosus were available. Of the 12 selected RCTs, 8 included patients with pemphigus vulgaris only and 4 included patients with both pemphigus vulgaris and pemphigus foliaceus. None of the available RCTs were found to include patients with pemphigus vegetans or pemphigus erythematosus. Summary of the selected articles [4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15] of interventions in pemphigus vulgaris and foliaceus is presented in [Table - 4a, b, c, d]. Bullous pemphigoid Number of articles on bullous pemphigoid selected at different stages of the systematic review is shown in [Table - 5]. Seven articles [19],[20],[21],[22],[23],[24],[25] met the selection criteria of second-stage screening and were selected for final analysis. Results are presented in [Table - 6a, b]. Discussion Pemphigus In the present review, an attempt was made to find out the evidence-based treatment for pemphigus. Good quality evidence consists of results of randomized controlled trials (RCTs). When an initial search was made on the two databases by using the phrase "randomized controlled trial" and name of a disease (eg, pemphigus vulgaris), it was found that very few articles were identified. The reason for this finding was that usually the articles that reported RCTs did not have this phrase in the titles or abstracts. Therefore, the search strategy was modified and it included a two-stage screening. It appears that this modified plan led to the identification of most, if not all, of the relevant articles. PubMed is a service of the United States National Library of Medicine and the National Institutes of Health and comprises more than 20 million citations for biomedical literature from MEDLINE, life science journals and online books. Approximately 5400 journals published in more than 80 countries are currently indexed in MEDLINE. The other database selected was the Cochrane Central Register of Controlled Trials. This database includes details of articles from MEDLINE and also from EMBASE and other published and unpublished sources. EMBASE currently has over 23 million indexed records from more than 7500 journals. For the second-stage screening, full-texts of 23 of 25 articles on pemphigus vulgaris and pemphigus foliaceus selected after the first-stage screening were obtained, from which 12 articles were finally selected [Table - 2] and [Table - 3]. These 12 studies used randomization for allocating treatments to different groups of patients. Most of the articles used at least one of the three immunological tests mentioned in methods of this article for diagnosing pemphigus. Two articles, [5],[15] which appeared to be relevant, mentioned that immunological tests (enzyme-linked immunosorbent assay [ELISA] for antidesmoglein 1 and 3 antibodies [5] and direct and indirect immunofluorescence assays [15] ) were performed, but it was unclear to this reviewer how the results of these tests were used in making the diagnosis. It may be very important to have clear-cut diagnostic criteria for pemphigus. This is relevant in individual patients as well as in a situation when a patient may be included in a clinical study. Using a uniform set of criteria will make it easier for results of different clinical studies to be compared. One of the articles selected in this review used a set of diagnostic criteria, which appear to be appealing. [6] These Japanese diagnostic criteria are as follows: pemphigus is diagnosed when at least one item from every three findings, or two items from clinical findings and one item from immunological findings are satisfied. The three groups of findings are:
In the immunologic findings, indirect immunofluorescence test for detecting IgG in patient′s serum which binds the cell surface of normal keratinocytes may also be added. Scientifically, one would require a set of diagnostic criteria for which sensitivity and specificity have been worked out. Assessment of the quality of the RCTs is a key step in a systematic review. Several quality scales have been developed for this purpose. In the present review, quality assessment was done using the Delphi list [Table - 1], which is a criteria list for quality assessment of RCTs specially for conducting systematic reviews. [1] This list consists of eight items and item one was further elaborated for quality assessment in this review. The first item of the original Delphi list is as follows: Treatment allocation (a) was a method of randomization performed? (b) was the treatment allocation concealed? Item 1a was expanded to give three possible responses: (i) Correct randomization method described, (ii) Inadequate randomization method described, and (iii) Randomization stated, but method not described. This expansion provided a clearer picture about the randomization procedure. Treatment allocation concealment, which is considered to be the most important indicator of quality of a trial, was understood to have taken place only when there was a clear statement about it or when there was a statement which meant that treatment to be allocated was not known before the patient was entered into the study. Quality appraisal of RCTs is sometimes done to produce a quality score and a threshold score may be used for inclusion of RCTs in a systematic review. However, as there may be differences of opinion among the reviewers with regard to the relative importance of different items of quality, in the present review detailed data about different quality items of all selected articles was presented [Table - 4a, b, c, d]. The Cochrane Collaboration publishes high-quality systematic reviews. Its review on interventions for pemphigus vulgaris and pemphigus foliaceus [26] describes 11 RCTs, using a different search strategy. Eight of these RCTs were identified in the present review also; four articles identified in the present review [4],[5],[6],[7] are not included in the Cochrane review. On the other hand, three articles [27],[28],[29] included in the Cochrane review were not identified in the database search for this review. These articles described the use of glucocorticoid alone versus glucocorticoid plus a traditional Chinese medicine, [27] low (0.5 mg/kg/day) versus high (1.0 mg/kg/day) initial doses of prednisolone, [28] and oral prednisolone versus oral prednisolone and plasma exchange. [29] All these studies had serious methodological problems and the effects of study interventions were considered inconclusive. [26] Following general conclusions may be drawn about the evidence-based treatment of pemphigus from the present review:
In view of the foregoing discussion, following suggestions may be made about future research on treatment of pemphigus:
Bullous pemphigoid In the second-stage screening, initially the first test in the second criteria was kept as follows: (i) positive direct immunofluorescence test for C3 and/or IgG on the epidermal roof of salt-split skin. This was done so that the patients with bullous pemphigoid are differentiated from those with EBA. But it was found that none of the articles in the second-stage screening met any of the criteria (ii), (iii), or (iv) and in only one article [20] the diagnosis was made by detection of autoantibody deposition at the blister roof on salt-split skin. Therefore, as a compromise, the wordings of the first test were changed to "positive direct immunofluorescence test for C3 and/or IgG at the dermoepidermal junction." It is to be clarified that in six [19],[21],[22],[23],[24],[25] of the seven RCTs, which were selected for final analysis based on this criteria, the possibility of inadvertent inclusion of some patients with EBA cannot be ruled out. This brings us to a situation similar to pemphigus. There are no uniform diagnostic criteria available for making diagnosis of bullous pemphigoid, which are used for individual patients and for their inclusion in clinical studies. It is important to have clear-cut diagnostic criteria for bullous pemphigoid, which include at least one positive immunological test from the following four tests: (i) positive direct immunofluorescence test for C3 and/or IgG on the epidermal roof of salt-split skin, (ii) serum IgG labeling epidermal roof by indirect immunofluorescence, (iii) detection of antibodies against BP180 and/or BP230 antigens, or (iv) demonstration by immunoelectron microscopy of deposition of IgG associated with basal cell hemidesmosomes. Cochrane systematic review on interventions for bullous pemphigoid describes 10 RCTs. [33] The three extra articles in the Cochrane review were identified in search of databases for the present review also. One article was in Chinese [16] and the other two in French [17],[18] and their full texts were unobtainable. These studies compared prednisolone alone versus prednisolone plus a Chinese medicine, [16] methylprednisolone versus prednisolone, [17] and higher versus lower doses of prednisolone. [18] All the three studies had important methodological problems and the results did not show statistically significant differences in any study. [33] Following general conclusions may be drawn about the evidence-based treatment of bullous pemphigoid from the present review:
In the light of the foregoing discussion, following suggestions may be made regarding future research on treatment of bullous pemphigoid:
At the final proof reading stage, repeat search on June 10, 2011 found 3 new articles on pemphigus vulgaris in PubMed and Cochrane Central Register of Controlled Trials each. Two articles were same in both databases. Only one article [34] passed through the second-stage screening [Table - 7]. One new article on bullous pemphigoid found in PubMed was excluded in first-stage screening. No new articles were found on other diseases. References
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11128t6b.jpg] [dv11128t4b.jpg] [dv11128t4a.jpg] [dv11128t2.jpg] [dv11128t4d.jpg] [dv11128t5.jpg] [dv11128t6a.jpg] [dv11128t7.jpg] [dv11128t3.jpg] [dv11128t1.jpg] [dv11128t4c.jpg] |
| |||||||||

![[Table - 1]](/showimage?dv/photo/dv11128t1.jpg){kind=link}
![[Table - 2]](/showimage?dv/photo/dv11128t2.jpg){kind=link}
![[Table - 3]](/showimage?dv/photo/dv11128t3.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[Table - 5]](/showimage?dv/photo/dv11128t5.jpg){kind=link}
{kind=link}
{kind=link}
![[Table - 7]](/showimage?dv/photo/dv11128t7.jpg){kind=link}