 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
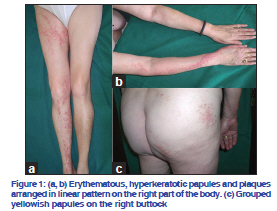
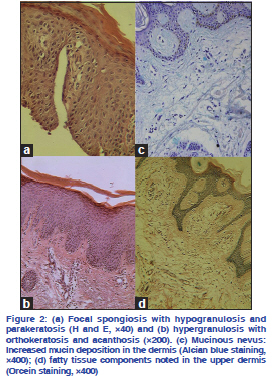
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 5, September-October, 2011, pp. 607-608 Letter to the Editor Extensive, adulthood inflammatory linear verrucous epidermal nevus associated with mucinous nevus Jelica S. Vukicevic, Danica J. Milobratovic1, Mirjana V. Milinkovic, Zoran Bogdanovic2 Clinic of Dermatovenereology, Faculty of Medicine, Clinical Centre of Serbia, Belgrade, 1Department of Dermatovenereology, Military Medical Centre, Belgrade, 2Outpatient Clinic Histolab, Belgrade, Serbia Correspondence Address: Code Number: dv11177 DOI: 10.4103/0378-6323.84079 Sir, Inflammatory linear verrucous epidermal nevus (ILVEN) is a benign cutaneous hamartoma first described in the literature in 1971.[1] Atypical presentations of ILVEN have been rarely reported and include onset in adulthood and involvement of wide areas of the body.[2] Mucinous nevus (MN) is a very rare entity whose name was proposed because of its nevoid character and distinctive histological pattern with mucin deposition in the papillary dermis.[3] We present a rare case of extensive, adulthood ILVEN associated with MN. A 68-year-old woman presented with linear, psoriasiform, pruritic papules, and plaques on the right side of the body. Lesions appeared 20 years ago in the right lower leg and were diagnosed as psoriasis with no response to treatment. On examination, skin of the right side of the face and neck, and right side of the trunk were covered with erythematous, scaly, verrucous papules and plaques disposed in a band-like fashion. Linear, hyperkeratotic, erythematous plaques were seen on right leg and arm and dorsa of the right hand and foot [Figure 1a, b]. The nail plates of the hands and feet were yellowish, discolored, and hyperkeratotic. On the right buttock, an oval, yellowish-colored, papular eruption with a linear distribution was also noted [Figure 1c]. The clinical diagnosis of ILVEN was confirmed by histology showing hyperkeratosis, focal parakeratosis, acanthosis with focal exocytosis and spongiosis in the epidermis. Agranulosis and parakeratosis alternating with hypergranulosis and orthokeratosis also were seen. Lymphocytic infiltrate around the blood vessels was found in the dermis [Figure 2a, b]. Skin biopsy from yellowish papules on the right buttock revealed invaginating hyperkeratosis, papillomatosis, acanthosis, and loosely separated collagen fibers in papillary dermis (either mucinosis or edema). The whole papillary dermis stained positive with Alcian blue at pH 2.5 [Figure 2c] suggesting mucinosis. Some fatty tissue components were also present in the upper dermis [Figure 2d]. After application of keratolytics, corticosteroid ointments and retinoids, scaling became less obvious and pruritus slightly regressed. ILVEN is a unilateral, pruriginous dermatosis manifested as erythematous, inflammatory, linear papules and plaques. Although the cause and pathogenesis are not known exactly, it is thought to be associated with upregulation of interleukin 1, interleukin 6, tumor necrosis factor α, and intercellular adhesion molecule 1.[4] It is most common in children, more often in girls, frequently occurs before the age of 2 years. Lesions are usually solitary, most often on the lower half of the body. Clinically, ILVEN should be distinguished from other epidermal nevi, nevoid psoriasis, and lichen striatus. Contrary to the linear epidermal nevus, ILVEN lesions are erythematous and pruriginous. The absence of pruritus and spontaneous regression are pathognomonic of lichen striatus. ILVEN is often difficult to differentiate from psoriasis. Psoriasis can occur in a nevoid form following Blaschko’s lines or Koebnerize and become superimposed on an epidermal nevus. The former is usually asymptomatic and typically responds to antipsoriatic treatment. Associated abnormalities are rarely reported in cases of ILVEN and it is likely that many are coincidental.[2] MN can be classified as either cutaneous mucinosis or a connective tissue nevus (CTN).[3] Some authors have suggested that MN without epidermal nevuslike changes should be included under CTN of the proteoglycan type and MN with epidermal changes included in the combined epidermal-CTN of proteoglycan type.[5] In half of the reported cases, MN was not present at birth and developed in childhood, adolescence, or early adulthood.[5] Clinically, MN appears as yellowish or brownish papules or plaques with unilateral and linear distribution. It affects more often the lower part of the trunk.[5] Diffuse mucin deposition in the superficial dermis, usually in a band-like distribution, is the primary histopathologic feature of MN.[5] Disruption of collagen and elastic fiber network in the mucinous area is often observed as well. Due to nevoid aspect, MN can be clinically confounded with the epidermal nevus, other CTN, nevus lipomatosus superficialis, surface hamartomas, and other types of cutaneous mucinosis.[3] CTN such as collagenoma may be associated with other congenital anomalies, for example, osteopoikilosis (in Buschke-Ollendorf syndrome) and tuberous sclerosis.[5] Typically, ILVEN is resistant to treatment. Therapeutic options include topical and intralesional glucocorticoids, dithranol, calcipotriol, excision, cryotherapy, and laser therapy.[2,4] MN may be treated with surgical excision and carbon dioxide laser.[5] In conclusion, we herein added an unusual presentation of ILVEN associated with hereditary MN. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11177f1.jpg] [dv11177f2.jpg] |
| |||||||||

{kind=link}
{kind=link}