 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
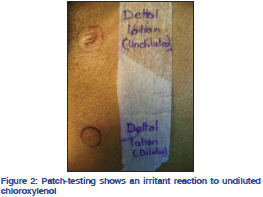
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 5, September-October, 2011, pp. 612-614 Letter to the Editor Contact depigmentation following irritant contact dermatitis to chloroxylenol (dettol) Ghanshyam K. Verma, Vikram K. Mahajan1, Vinay Shanker, Geeta Ram Tegta, Nidhi Jindal, Samridhi Minhas Department of Dermatology, Venereology and Leprosy, Indira Gandhi Medical College, Shimla 171 001, Himachal Pradesh, 1Department of Dermatology, Venereology and Leprosy, Dr. R.P. Govt. Medical College, Kangra (Tanda) 176 001, Himachal Pradesh, India Correspondence Address: Code Number: dv11180 DOI: 10.4103/0378-6323.84086 Contact de-pigmentation or chemical leukoderma can occur as sequelae of either irritant or allergic contact dermatitis (ACD) that may or may not be of occupational origin. The chemicals implicated invariably are monobenzyl ether of hydroquinone, hydroquinone, tertiary butyl catechol, p-tertiary butyl phenol (PTBP), p-cresol, phenol derivatives, mercaptoamines, physostigmine, and topical minoxidil.[1,2] The described case of contact depigmentation following irritant contact dermatitis (ICD) from chloroxylenol (dettol), a common household disinfectant, is first of its kind to the best of our knowledge. A 65-year-old male presented with mild erythema and scaling, hyperpigmented, and depigmented patches of variable size and shape over face, ears, “V” area of neck and dorsal of hands and feet [Figure 1]. He had applied undiluted chloroxylenol (dettol) over face, hands, and feet for itchy skin (photopruritus) and developed erythema, edema, oozing, crusting, and stinging and burning sensation that subsided over next 2 weeks with blotchy hyperpigmentation and depigmentation. He did not have history of prior topical/systemic medications or, personal or family history of vitiligo. Systemic examination and laboratory investigations were normal. A skin biopsy performed with the provisional diagnoses of contact depigmentation and disseminated discoid lupus erythematosus showed focal hyperkeratosis, epidermal atrophy, flattened reteridges, perivascular lymphocytic infiltrate in the upper dermis and lack of melanocytes in the basal layer. Patch testing showed no positive reaction with Indian Standard Series[3] or chloroxylenol (1% pet), but an irritant reaction to undiluted chloroxylenol occurred [Figure 2] and the test site developed depigmentation later. Topical mometasone furate 0.1% ointment was prescribed for twice daily application. Chemical leukoderma from occupational exposure to compounds containing PTBP, amylphenol, O-syl, vesprene in insecticides, paints, rubber, lubricating and motor oils, photographic chemicals, antimicrobials, disinfectants, soaps, detergents, deodorants, and inks has been reported often.[1] Nonoccupational chemical leukoderma reportedly occurs secondary to allergic contact dermatitis with para phenylene diamine (PPD) in hair colorants or temporary tattoos,[4,5] methacrylates,[6] perfumes, and alstroemeria[7] or following contact with common household products such as rubber or nylon articles, spectacles, plastic watch strap, adhesives, condoms, foot wears, etc.[1] Chloroxylenol (dettol) or p-chloro-m-xylenol (PCMX), a water and oil soluble halogenated aromatic compound, is used commonly as preservative and household disinfectant or as an active agent in antimicrobial soaps. It is also used in many over-the-counter products for cuts, wounds and infections, powders, cleansers, work creams, coolant oils, electrocardiogarphic pastes and cosmetics. People often use it diluted/undiluted to decontaminate themselves or their environment hoping to eradicate a genuine or imagined infection, add in bathing water, apply it in inflammatory conditions especially in perineal area, or for any other dermatoses such as urticaria, generalized pruritus, xerosis, or inflammatory conditions without medical advice. It is a potential contact sensitizer and can cause localized ICD, ACD or exacerbation of pre-existing dermatitis.[8] Generalized body involvement may occur from its use in bathing water or for washing particularly when used undiluted. However, chemical leukoderma due to chloroxylenol (dettol) is rare. Malakar and Panda[9] reported widespread hypopigmentation in a car mechanic who took dettol bath on two consecutive days to treat a pustular dermatosis and developed generalized depigmentation a week later. A positive patch test to chloroxylenol (1%) and depigmentation at the patch test site in their patient suggested contact allergic dermatitis to chloroxylenol as the underlying mechanism. Negative reaction with chloroxylenol (1% in petrolatum), irritant contact reaction to undiluted chloroxylenol (as used by the patient) on patch testing and subsequent depigmentation of test site, and histologic features were suggestive of chemical leukoderma as a result of ICD in our patient. As he did not follow-up further, his primary dermatosis (cause of photopruritus?) remained unidentified. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11180f2.jpg] [dv11180f1.jpg] |
| |||||||||

{kind=link}
{kind=link}