 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
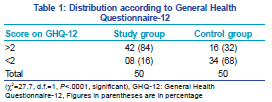
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 5, September-October, 2011, pp. 625 Net Letter Psychiatric morbidity in psoriasis patients: A pilot study Surender Kumar, Dilip Kachhawha1, Ghanshyam Das Koolwal, Sanjay Gehlot, Ankit Awasthi Departments of Psychiatry and 1Dermatology, Dr. S.N. Medical College, Jodhpur, Rajasthan, India Correspondence Address: Code Number: dv11188 DOI: 10.4103/0378-6323.84074 Sir, Psoriasis is a relatively common, chronic, inflammatory, and hyperproliferative skin disease that affects 1.4%–2.0% of the population. The skin and the central nervous system are embryologically related, and they share several hormones, neurotransmitters, and receptors. The skin plays a key role as a sensory organ in the socialization processes throughout the life cycle. Numerous skin changes are seen in response to emotional stimuli, and skin appearance greatly influences body image and self-esteem. It has been reported that psychological stress perturbs the epidermal permeability barrier homeostasis, thus acting as a precipitant for psoriasis. Psychiatric and psychosocial factors play an important role in several skin diseases and the prevalence of psychiatric morbidity in these patients is also very high. Most of the data available on psychosocial dysfunction and psychiatric morbidity in psoriasis is from the West. Only a few studies are available from India. Approval for this study was obtained from the Ethical Committee of Dr SN Medical College. The study was conducted over a period of 7 months, from June 2009 to December 2009 in the OPD of the Skin and STD Department, MDM Hospital, Jodhpur. We selected 50 psoriasis patients of both sexes between 12–65 years of age. In all patients the diagnosis had been confirmed by a dermatologist. These patients were compared with 50 matched controls. Patients having chronic debilitating disease and other concomitant skin diseases were excluded from the study. The tools use were Goldberg’s General Health Questionnaire-12 (GHQ-12), which is a self-administered 12-item questionnaire that was originally designed for use in the general practice setting as a screening tool. In the GHQ-12 the respondent was asked to compare his recent state of health with his usual state of health. Interpretation of the answer was based on a fourpoint response scale scored using a bimodal method. The maximum score was 12 and the cutoff score was ≥2. The Hamilton Rating Scale for Anxiety (HAM-A) consisted of 14 items and was heavily focused on somatic symptoms, with a great reliance on the patient’s subjective report. Each item was rated on a 0–4 scale. The Zung Self-Rating Depression Scale (ZSRDS) consisted of 20 items and was used for quantitative measurement of depression. Information gained after administration of these questionnaires was subjected to suitable statistical analysis (Chi-square test and Pearson coefficient of correlation). Psychiatric morbidity was studied by using the GHQ- 12 [Table 1]. It revealed that 84% of the psoriasis patients had psychiatric morbidity, while only 32% of the control subjects had psychiatric morbidity. The difference was found to be statistically significant (P<0.0001). Anxiety symptoms were assessed using the HAM-A. We found that 52% psoriasis patient had mild anxiety, 36% had mild to moderate anxiety, and 12% had moderate to severe anxiety. The corresponding figures among the controls were 84%, 14%, and 2%, respectively. The difference between the groups was statistically significant (P=0.0023). The ZSRDS was used to assess depression. It revealed that 68% of the psoriasis patient had mild depression, 18% had moderate depression, 4% had severe depression, and 10% had minimal or no depression, compared to 16%, 2%, 0%, and 82%, respectively, of the control group. The difference between the two groups was extremely significant (P<0.0005). Thus, depression and anxiety were the most common psychiatric morbidities evident in psoriasis patients. Earlier studies by Picardi et al.,[1] Mattoo et al.,[2] and Saleh et al.[3] reported psychiatric morbidity in 45%, 24.27%, and 38% of the subjects, respectively, which is quite low as compared to the results of our study. Previous studies by Saleh et al.[3] and Deshpande et al.[4] found low prevalence of anxiety also, with only 58% and 15%–50% of psoriasis patients, respectively, having features of anxiety. Our study found that 90% of psoriasis patients had depression of some grade, which is very high as compared to 51% reported by Devrimici-Ozguven et al.[5] and 30% reported by Saleh et al.[3] The study by Deshpande et al.[4] found that 50%–97% of psoriasis patient had depression, which is quite close to our own findings. The relatively higher percentage of psychiatric morbidity found in our study is probably partly due to increased awareness regarding psychiatric illness in the current decade, with people becoming more concerned about their behavior and attitude. Moreover, cosmetic awareness has also increased, and people today are more concerned about their looks and appearance. Competition and the stresses of day-to-day life make psoriasis patients feel inferior and less competent as compared to the normal population, which leads to anxiety and depression. The chronicity of the disease and the frequent relapses are also causes for the increased anxiety and depression in psoriasis patients. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11188t1.jpg] |
| |||||||||

{kind=link}