 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
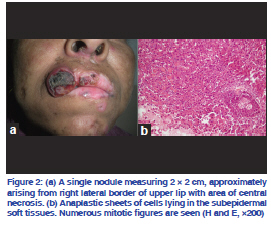
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 5, September-October, 2011, pp. 626 Net Letter Metastasizing squamous cell carcinoma arising from chronic discoid lupus erythematosus plaque of recent onset Mandeep Dhingra, Mala Bhalla, Gurvinder Pal Thami, Preeti Mittal Departments of Dermatology and Pathology, Government Medical College and Hospital, Sector 32, Chandigarh, IndiaCorrespondence Address: Code Number: dv11191 DOI: 10.4103/0378-6323.84078 Sir, Squamous cell carcinoma (SCC) is a well-recognized, long-term complication of chronic discoid lupus erythematosus (CDLE). Hypertrophic lupus erythematosus (HLE) is a distinct variant of CDLE characterized by its chronic course, sometimes destructive scarring, and poor response to treatment. In the present communication, we describe a case of rapid malignant transformation in a CDLE plaque of recent onset over the upper lip, which was initially diagnosed as HLE.A 36-year-old housewife from North India, a known case of CDLE for last 2 years, presented with a single asymptomatic, slowly progressive, warty lesion over the upper lip since 1 year. There was no history of fever, photosensitivity, joint pain or Raynaud’s phenomenon. Cutaneous examination revealed a large, verrucous, non-adherent plaque, 3 × 6 cm, involving right side of the upper lip and extending across the midline and into the oral mucosa [Figure 1a], along with multiple, discrete, scaly, erythematous plaques with central atrophy over the face, V area of neck, upper back and arms. Histopathologic examination of the lip lesion did not reveal any signs of malignancy [Figure 1b] and was provisionally diagnosed as HLE. Haemogram showed anemia. Chest X-ray, electrocardiogram and urine examination were within normal limits. Antinuclear antibody (ANA) and anti-dsDNA tests were negative. Therapy with hydroxychloroquine and topical steroids along with intralesional steroids over the verrucous lesion was initiated. As the lip lesion reduced in size over the next 11 months, surgical debulking was done for cosmetic reasons. Other lesions responded favorably to therapy. Within a month of excision, the patient developed a distinct growth over the debulked lesion, starting as a small nodule, which rapidly progressed to a large mass with central ulceration [Figure 2a]. The nodule was tender, adherent to the underlying muscle and bled on touch. Right submandibular lymph nodes were enlarged, firm, mobile and non-tender. Histopathologic examination confirmed the diagnosis of poorly differentiated SCC [Figure 2b]. Fine needle aspiration cytology from the lymph nodes showed malignant cells along with tissue necrosis. Surgical debulking was done and chemotherapy in the form of cisplatin and 5-flurouracil was started. CDLE lesions may develop malignant transformation; an incidence of 3.3% was reported by Millard and Barker, with a delay of 26–41 years (mean 30.8 years) between initiation of the CDLE and the appearance of SCC.[1] In another review of 10 African-American patients by Sherman et al.,[2] it was observed that SCC in depigmented CDLE lesions occurred only in sunexposed areas with a male predisposition and a history of CDLE for an average of approximately 18 years (range 7–30 years). Although the above-mentioned studies[1,2] indicate a long latent period, Parikh et al.[3] have reported a case of SCC in a CDLE plaque over sunprotected area of only 1 year duration. In the present case, the SCC occurred after an interval of 3 years on photoexposed upper lip CDLE plaque with chronic scarring. Hence, a high index of suspicion is warranted in cases of CDLE even if the plaque is of recent onset, especially with risk factors like photoexposed area and chronic scarring. Early SCC may be difficult to differentiate from HLE, posing a significant clinical as well as histopathologic dilemma. Eruption of nodules within heavily scarred areas of the scalp, lips and nose in association with bleeding and ulceration favor the development of SCC within the lesions of CDLE.[4] Histologically, pseudo-epitheliomatous hyperplasia may be a feature of HLE, and the distinction between this and SCC is important. The presence of predominantly lichenoid interface dermatitis, thickened basement membrane, and perivascular and periappendageal mononuclear infiltrate associated with epidermal hyperplasia may help in differentiating SCC from HLE.[4,5] Presence of epidermal hyperplasia with atypical keratinocytes and breach of the basement membrane are characteristic of neoplasia. Immunoflourescence may also be helpful to differentiate between SCC and HLE.[4] In the present case, it is very likely that the initial lesion diagnosed as HLE might have been early invasive SCC at the first instance which may not have been picked on histopathologic examination. Also, the presence of single lesion of HLE in a patient with so many classic CDLE lesions is unlikely. The rapid recurrence of lesions within 1 month after surgery again suggests that it may have been an early invasive SCC from the very onset. In retrospect, biopsies from multiple quadrants and histopathologic examination of the excised lesion might have helped. This case has been presented to highlight that malignant transformation may occur even in a recent plaque of CDLE and also the diagnostic dilemma that verrucous lesions may pose in CDLE patients. REFERENCES
The following images related to this document are available:Photo images[dv11191f2.jpg] [dv11191f1.jpg] |
| |||||||||

{kind=link}
{kind=link}