 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
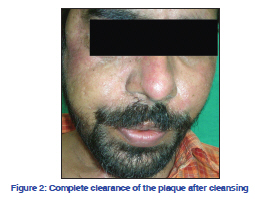
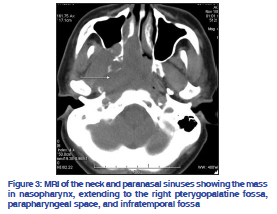
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 5, September-October, 2011, pp. 627 Net Letter Dermatosis neglecta unmasking recurrence of carcinoma nasopharynxThirthar Palanivelu Vetrichevvel, Venkatswami Sandhya, Subramanyam Shobana, Sankarasubramanian Anandan Department of Dermatology and Venereology, Sri Ramachandra University, Chennai, India Correspondence Address: Code Number: dv11196 DOI: 10.4103/0378-6323.84087 Sir, A 29-year-old man presented with complaints of progressively enlarging, hyperpigmented lesion over the face of 7 months duration. The lesion had started on the right infraorbital region and progressed to involve the left side of the face. He had been operated on the right side of his face, 1 year ago, for complaints of nasal stuffiness with bleeding, and was not on regular follow-up. He had mild pain on the right side of the face but maintained that he continued his regular cleansing habits. Local examination revealed a well-defined hyperpigmented verrucous plaque of size 15.2 × 5.1 cm extending from the right preauricular region to the nasolabial fold, and onto the left cheek [Figure 1]. Suture scars were noticed in the right infraorbital and paranasal regions, and in the neck. Tenderness was noted over the right cheek but there was no regional lymphadenopathy. Presence of a scar and the tenderness prompted a diagnosis of dermatosis neglecta. After counseling, the lesion was wiped firmly with a cleansing lotion containing cetyl alcohol and the plaque could be completely removed [Figure 2]. The patient was advised otorhinolaryngology reference, regular cleansing of the region with soap and water, and follow-up with previous case records. He presented to us again after one month with a recurrence of the skin lesions, associated with an increase in pain on the right hemi-face and persistent headache. The original case records revealed that the excised tumor was carcinoma of the nasopharynx (adenoid cystic carcinoma) [Figure 3] and an immediate otorhinolaryngology reference revealed the recurrence of the tumor. The skin lesions were re-cleansed and he was advised regarding the prevention of its re-accumulation. He is currently on treatment and follow-up with otorhinolaryngology and oncology departments. Dermatosis neglecta arises from inadequate cleansing of the skin leading to a build up of corneocytes, sebum, and sweat resulting in a hyperpigmented patch or plaque with variable degree of scaling and verrucosity, and is easily removable by cleansing with soap and water.[1] Our patient presented with a verrucous plaque, which is to be differentiated from verrucous epidermal nevi, terra firma forme dermatosis, confluent and reticulated papillomatosis, and acanthosis nigricans. While verrucous epidermal nevi are present since birth and amenable only to excision, confluent and reticulated papillomatosis of Gougerot and Carteaud, usually presents on the trunk as grayish brown papules, that coalesce to form confluent plaques centrally with a reticular pattern peripherally. Pityrosporum orbiculare is implicated in its causation and responds to oral Minocycline, oral and topical retinoids.[1,2] Terra firma forme dermatosis is a form of cutaneous discoloration resembling dirt, variably presenting from brownish/blackish hyperpimentation to papulamatosis plaques. It is postulated that it is initiated by inadequate cleansing, resulting in altered keratinocyte maturation and melanin retention, and is not removable with water or soap but by firm cleansing with isopropyl alcohol.[1] Acanthosis nigricans, commonly occurring secondary to obesity, insulin resistance and malignancy usually presents as symmetric, brown to gray-black, velvety, papillomatous cutaneous thickening in the flexures and responds to topical retinoids along with treatment of the primary disease. Similar hyperpigmented plaques can be seen over sites of previous inflammation, over elbows and knees in frictional dermatosis, and in the anterior neck in atopics, but can be differentiated by clinical history, examination, and alcohol cleansing test.[3] The inadequate cleansing in patients with dermatosis neglecta is usually attributable to a disability, pain/ hyperesthesia in that region or immobility occurring secondary to trauma, surgery, or nerve palsies.[4,5] Our patient had presented with recurrent dermatosis neglecta probably due to the increasing pain caused by the recurrence of the malignancy that prevented him from adequately cleaning the region. Although the lesions are innocuous and are easily amenable to treatment,[3] an attempt must always be made to ascertain the underlying cause in relevant clinical settings. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11196f3.jpg] [dv11196f2.jpg] [dv11196f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}