 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
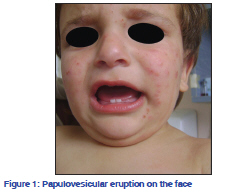
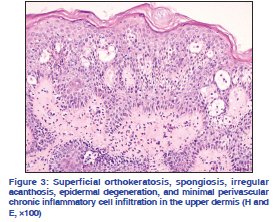
Indian Journal of Dermatology, Venereology, and Leprology, Vol. 77, No. 5, September-October, 2011, pp. 627-628 Net Quiz Papulovesicular eruption located on the face and extremities in a childMutlu Çoban, Engin Kocabaş, Peyker Temiz1, Pelin Ertan2, Aylin Türel Ermertcan Celal Bayar University, Faculty of Medicine, Departments of Dermatology, 1Pathology and 2Pediatrics, Manisa, Turkey Correspondence Address: Code Number: dv11197 DOI: 10.4103/0378-6323.84088 A 14-month-old male child presented to our outpatient clinic with pruritic vesicles that had started a month ago, first on the face and then on the hands and feet. With detailed history obtained from his mother we learned that he had had similar complaints in the newborn period, during the last summer, and again during the spring of the present year. She said that his lesions had healed on each occasion, leaving white spots. The family history was negative for photosensitivity. Dermatological examination revealed a papulovesicular eruption on the face and extremities and hypopigmented scars on the dorsal aspect of his hands [Figures 1 and 2]. The skin type of the patient was type II. The complete blood cell count and the liver and renal function tests were found to be in the normal ranges. The direct microscopic examination for Sarcoptes scabiei was negative. Histopathological examination of skin biopsy showed superficial orthokeratosis, spongiosis, irregular acanthosis, epidermal degeneration, and minimal perivascular chronic inflammatory cell infiltration in the upper dermis [Figure 3]. The diagnosis is hydroa vacciniforme Hydroa vacciniforme (HV) is a rare, acquired photodermatosis of unknown etiology, which predominantly affects children. It is characterized by the occurrence of vesicles on light-exposed areas, especially the malar areas, bridge of the nose, lips, ears, and the dorsa of the hands and forearms, a few hours after sun exposure. The vesicles crust and heal over a period of 1–6 weeks, leaving varioliform scars.[1] In our patient, with the detailed history obtained from his mother, we learned that he had had similar complaints last summer and, again, this spring. On dermatological examination, his lesions were localized on light-exposed areas and there were hypopigmented scars. The diagnosis of hydroa vacciniforme can be made on the basis of these clinical and histopathological findings. HV was first described by Bazin in 1862.[2] The condition is seen equally in both sexes. Presentation is usually during the first decade, but there is a lateonset variety.[3] There are no diagnostic laboratory tests for the disease, and the diagnosis is made principally on clinical grounds, supported by the very characteristic histology and the frequently abnormal monochromatic irradiation tests, which demonstrate photosensitivity.[4] The early lesion is an epidermal multilocular vesicle with reticular degeneration. A dense, perivascular, lymphohistiocytic infiltrate with vessel hemorrhage and thrombosis may occur in the dermis. Late lesions show epidermal and dermal necrosis with a surrounding, chronic, inflammatory infiltrate. Direct immunofluorescence study results are usually normal, except for rare reports (two patients) of C3 deposits at the dermoepidermal junction and in the small dermal vessels.[5] Complications of HV are rare. Eye involvement manifests as conjunctivitis, sometimes associated with severe chemosis. Corneal ulcerations have been described in a few cases and occur on the exposed areas of the cornea, with the upper photoprotected surface spared.[1] Some reports have recently demonstrated that HV is associated with Epstein-Barr virus (EBV) infection and lymphoma, but some of these cases showed atypical features, and these cases may not represent the usual form of HV.[6] History, examination, and laboratory investigations are usually sufficient to differentiate these conditions and accurately diagnose HV.[1] The differential diagnosis of HV includes several blistering disorders that are light induced, for example, erythropoietic protoporphyria (EPP), vesicular polymorphous light eruption (PMLE), bullous lupus erythematosus (BLE), solar urticaria, Hartnup disease, actinic prurigo, hydroa aestivale, porphyria cutanea tarda (PCT), and some forms of xeroderma pigmentosum (XP).[2,6] The eruptions in EPP are typically an intensely edematous, urticarial reaction, and only its more severe purpuric and vesicular forms cause scarring.[6] Negative porphyrins in the patients exclude EPP and other porphyrias that can mimic HV, such as congenital erythropoietic porphyria and childhood PCT. Actinic prurigo shows scarring and severe cases may show involvement of non-sunexposed sites such as the buttocks.[2] Hydroa aestivale is considered by some investigators to be a childhood type of PMLE, while other researchers have postulated that it is a nonscarring form of HV. Unlike HV, PMLE is usually nonscarring and has a later age of onset than HV.[5] Hartnup disease may clinically mimic HV but is excluded by the absence of aminoaciduria. Bullous LE is unlikely with a normal autoantibody profile. Milder forms of XP such as complementation group F (XPf) are characterized by repeated episodes of erythema with scaling, freckling, mild xerosis, and seborrheic keratosis-like lesions. Blistering is an uncommon feature and scarring does not seem to occur.[2] In most patients the condition disappears by the time they reach adolescence, although the scars are permanent. Photoprotection with appropriate clothing and a broad-spectrum sunscreen form the standard approach. If there is no response to photoprotection, spring-time prophylactic therapy using broad-band UVB, narrow-band UVB, or PUVA can be beneficial. Although some anecdotal evidence exists to support the use of beta-carotene/canthaxanthin, azathioprine, and antimalarial therapy, their real value is uncertain. Prophylactic fish oil may also be of help, although poor tolerance limits its use.[3] We prescribed a broad-spectrum sunscreen and a topical corticosteroid cream and adviced appropriate clothing for our patient. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11197f1.jpg] [dv11197f3.jpg] [dv11197f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}