 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 77, No.6, November-December 2011, pp.745-746 Net Letter Giant warts in a Chinese with epidermodysplasia verruciformis Jose Aneiros-Fernandez, Jose M. Jimenez-Rodriguez1, Aurelio Martin, Salvador Arias-Santiago2, Angel Concha Departments of Pathology and 1Plastic Surgery, Virgen de las Nieves
Hospital, Granada, 2Department of Dermatology, University San
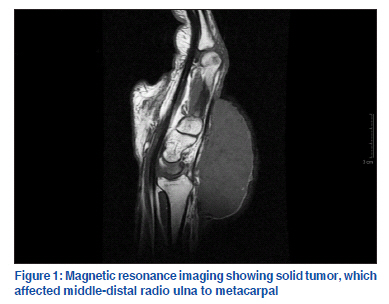
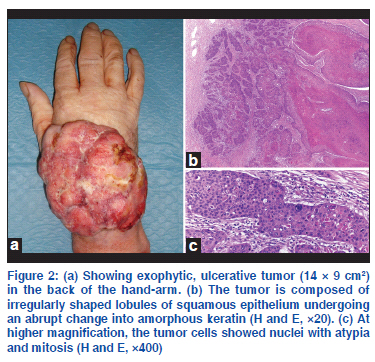
Cecilio Hospital, Granada, Spain Code Number: dv11227 Sir, Proliferating trichilemmal cyst is a benign tumor that originates in the outer root sheath of hair follicle. Usually, it is located on the scalp in older women, but also have been reported in other sites such as back, chest, axilla, groin, gluteal region, thigh, vulva, and face.[1] Malignant transformation of proliferating trichilemmal cyst is confirmed only on histological findings. This tumor has a variable biologic behavior with local recurrence and lymph node metastasis.[2] We have recently observed a case of giant malignant proliferating trichilemmal tumor in a 63-year old man affecting the arm, wrist, and back of hand. Magnetic resonance imaging showed it to be a solid tumor affecting middle-distal radio ulna to metacarpal [Figure 1]; however, tendinous structures were preserved. Clinical examination revealed a focally ulcerated, exophytic tumor, limiting the mobility of the fingers, measuring 14 × 9 cm2 with 3 years of evolution [Figure 2a]. He noticed a rapid increase in size 3 months ago. He had no prior trauma to this area, and had no prior dermatologic problem. There was no papable lymphadenopathy. Histopathology of the lesion showed typical cystic areas with trichilemmal keratinization [Figure 2b], showing irregular nests with deep desmoplastic stroma [Figure 2c]. The tumor cells showed marked nuclear atypia and abundant mitotic activity. Immunohistochemistry was focally positive for CK7, CK8, and CK18, and negative for AML, CD34. Surgical excision was performed with wide margins and axillary dissection without evidence of metastasis. At 3 months, there was no tumor recurrence. There are less than 30 published cases of malignant proliferating trichilemmal tumor, showing 12 cases of metastatic disease, with an average of 30%. Metastases may be noticed at the time of diagnosis or until 30 years later.[3] Ye et al.[4] proposed three groupings of proliferating pilar tumors (PPTs) within a series of 76 cases with regard to histologic criteria and correlated these criteria with malignant potential. Group 1 PPTs, benign lesions that had no recurrence, displayed well circumscribed margins, modest nuclear atypia, and no pathologic mitoses, necrosis, or vascular or neural invasion. Group 2 PPTs, low-grade malignant lesions that may recur, exhibit in addition irregular and locally invasive margins and involvement of deep dermis and subcutis. Group 3 PPTs, high-grade malignant tumors with a tendency toward recurrence and lymph node metastasis, manifest invasive patterns of growth with prominent nuclear pleomorphism, atypical mitoses, necrosis, and possible vascular or neural invasion. Group 1 may be regarded as benign, group 2 as having the potential for locally aggressive growth, and group 3 as also having metastatic potential. The latter two categories might be equated with low and high grades of malignancy among PPTs of the skin.[4] Malignant proliferating trichilemmal tumor with human papillomavirus type 21 in a patient with epidermodysplasia verruciformis had been reported. There is no specific immunohistochemical marker of malignant trichilemmal differentiation (absence of CD34, AML, etc.) and although they are positive for cytokeratin 8, cytokeratin 18 and 5/6 does not allow differentiation from squamous cell carcinoma.[5] The only information that allows us to establish the diagnosis and differentiate it from squamous cell carcinoma is the presence of solid and cystic areas showing a sharp keratinization with extensive amorphous eosinophilic keratin, and an invasive component with marked nuclear atypia, necrosis, and mitosis. The treatment of these lesions is local excision with a margin of 1 cm, sometimes may require radiation therapy to prevent recurrence and chemotherapy for metastatic disease.[5] This neoplasm is most commonly found on the scalp and on back of the neck. We report this case of malignant proliferating trichilemmal tumor giant infrequent location on the hand. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11227f2.jpg] [dv11227f1.jpg] |
| |||||||||

{kind=link}
{kind=link}