 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
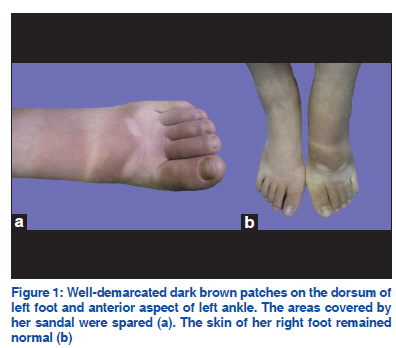
Indian Journal of Dermatology, Venereology and Leprology, Vol. 77, No.6, November-December 2011, pp.753-754 Net Letter Phytophotodermatitis due to wild carrot decoction Ru-zhi Zhang, Wen-yuan Zhu Department of Dermatology, The First Affiliated Hospital of Bengbu
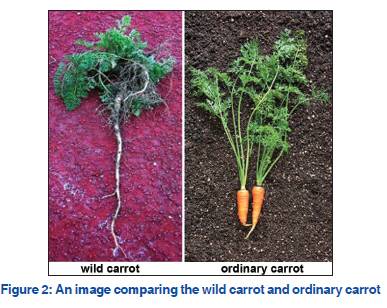
Medical College, Bengbu, Republic of China Code Number: dv11231 Sir, Phytophotodermatitis is the eruption that occurs after contact with photosensitizing compounds (furocoumarins) in plants and exposure to sunlight. Furocoumarins are a group of antifungal dyestuffs produced by certain plants and consist of psoralens, 5-methoxypsoralens, 8-methoxypsoralens, etc. Principal plant families provoking phototoxic reactions are Umbelliferae, Rutaceae, Moraceae, and Leguminoseae.[1] Wild carrot, which belongs to the Umbelliferae family, is credited with many medicinal properties. However, we describe here an unusual case of phytophototoxicity induced by wild carrot decoction. A 24-year-old female presented with a 4-day history of hyperpigmented macules on the dorsum of the left foot. Seven days prior, the patient applied wild carrot decoction for treating the unknown swelling of her left foot. The decoction was obtained from a handful of freshly whole wild carrots boiled in water. Wet compressing with the decoction over her left foot was performed three times a day, consecutively 3 days. During those days, she was dressed in short skirt, sandals, and walked about in the sunny days in July. On the third day, a burning sensation and erythema occurred on her left foot. Without any treatment but removing the wet compress, the erythema dissolved gradually and left behind disfiguring brown patches. During the whole period, the lesions were not particularly itchy and she was otherwise well. Dermatological examination revealed welldemarcated dark brown patches on her dorsum of left foot and anterior aspect of left ankle. There was complete sparing of the areas covered by her sandal, which blocked sun exposure. Meanwhile, the skin of her right foot remained normal [Figure 1a and b]. The patient’s clinical findings and history suggested the diagnosis of phytophotodermatitis. She was instructed to avoid exposure to sunlight. Four weeks after the initial clinical presentation, only a very slight hyperpigmentation over the affected areas remained. A year later, the patient told me by telephone that the hyperpigmentation on her foot took 3 months to fade. Subsequently, she attempted to use the same decoction over her right foot and kept away from sunlight, but no lesions or discoloration appeared. Both photoirritant contact dermatitis (PICD) and photoallergic contact dermatitis (PACD) are seen by most dermatologists in general practice. The reaction to furocoumarins in plants, termed as phytophotodermatitis, which belong to PICD, is a nonimmunologic, phototoxic reaction. Lesions may simply become erythematous, vesicles or bullae or appear as hyperpigmented patches without a preceding erythematous phase, and the hyperpigmentation may persist up to 6 months after exposure.[2] Phytophotodermatitis is a clinical diagnosis.[3] Photopatch testing in such patients is contraindicated, because a positive response might be severe, it would be expected to occur in the general population, and as such would not be discriminating in making the diagnosis. The differential diagnosis of this case includes irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), and suntan. Unlike phytophotodermatitis, the eruption of ICD does not require UVA light exposure. The patient used the same decoction over her right foot and kept away from sunlight, but no lesions or discoloration appeared. Moreover, there was complete sparing of the areas covered by her sandal. So the diagnosis of ICD and ICD could be excluded. The hyperpigmentation alone may resemble a suntan. However, a suntan has an immediate pigment darkening effect which peaks at about 72 hours, and usually darkens all exposed skin diffusely. By contrast, phytophotodermatis pigmentation may appear between 24 and 48 hours, but persists as long as 6 months; it produces well-circumscribed lesions, often with bizarre shapes. Based on the appropriate history and characteristic clinical manifestation, our patient was diagnosed with phytophotodermatitis. Our case is of great interest for the reason: the causative factor was wild carrot decoction. Comparing with cultivated form [Figure 2], wild carrot’s root is small and spindle shaped, whitish, slender and hard, with a strong aromatic smell, and an acrid, disagreeable taste. The leaves contain furocoumarins that may cause allergic contact dermatitis from the leaves, especially when wet.[4] Here rises a question: when the plant is boiled, does the containing photosensitizer plant still remain active? Although not further inquiring into the activity of phototoxic agents when the plant is boiled, we believe the phototoxic agents remain active. Recently, there are case reports of phytophotodermatitis caused by the fig leaf decoction.[5] Moloney and his colleagues[6] described a 56-year-old farmer who developed an extensive photo-induced dermatitis after ingesting a herbal decoction prescribed for his chronic hand dermatitis. Home-made decoctions are sometimes employed following recipes reported by friends and/or magazines, but it should be noticed that they may be dangerous for health, causing phytophotodermatitis. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11231f1.jpg] [dv11231f2.jpg] |
| |||||||||

{kind=link}
{kind=link}