 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 17, No. 1, May 2002, pp. 47-67 Ghana's Reproductive Revolution: Analysis of the Determinants of Fertility Transition CHUKS J., Ph.D. Regional Institute for Population Studies, Legon, GHANA. Code Number: ep02003 Abstract: The present article examines trends in the proximate determinants of fertility in Ghana over a decade (from 1988 to 1998) with a view to finding out their contributions to reproductive change and whether the reported fertility decline was a product of short-term fluctuations in fertility or reporting errors or the commencement of a sustained decline in completed family size. Using the Ghana Demographic and Health Surveys data sets of 1988, 1993, and 1998, the findings show that postpartum infecundability has a far more dominant inhibiting effect on fertility than the other proximate fertility determinants. Specifically, the fertility suppressing effects of postpartum infecundability are more important than the effects of contraception, and marriage patterns in explaining fertility levels and trends in Ghana. The findings of the study further show that both age at first marriage and age at first birth have increased in Ghana during 1988-1998 period, thus confirming the reproductive revolution currently underway in Ghana. However, the greatest change has been noticed among the youngest age group, as well as among women with higher education, and who live in urban areas, and Greater Accra, Ashanti, and Eastern regions. Résumé: Dans cet article, l'auteur examine les tendances sur une période de 10 ans (1988-1998) de la fécondité au Ghana pour déterminer leurs contributions à l'évolution de la reproduction et voir si la baisse de la fécondité dont on parle résulte de fluctuations à court terme, d'erreurs dans l'analyse ou est le démarrage d'une diminution durable de la taille de la famille. En partant des données des Enquêtes de Démographie et de Santé (EDS) du Ghana des années 1988, 1993 et 1998, les résultats ont montré que l'infécondité post-partum a un effet beaucoup plus marqué sur la fécondité que les autres déterminants immédiats de la fécondité. En particulier, les effets de suppression de la fécondité de l'infécondité post-partum sont plus importants que ceux de la contraception et des types de mariage dans l'explication des taux et des tendances de la fécondité au Ghana. En outre, les résultats ont également montré qu'au Ghana, l'âge au premier mariage ainsi que l'âge à la première naissance ont tous deux augmenté pendant la période considérée, ce qui confirme la révolution actuelle en matière de reproduction dans ce pays. Cependant l'évolution la plus importante s'est faite chez les groupes les moins âgés ainsi que chez les femmes qui sont parvenues à l'enseignement secondaire et qui habitent dans les zones urbaines comme le Grand Accra et les régions Ashanti et orientales. Introduction High fertility and escalating growth rates in the face of steadily declining mortality characterized Ghana's population trends since the 1950s. This led to the promulgation of the 1969 Population Policy, which was revised in 1994 (Republic of Ghana, 1964; 1994). Ghana's population policy aims to achieve a systematic, sustained and orderly, national development which could ensure a constantly increasing quality of life for all Ghanaians. In fact, a crucial policy choice that stimulated the revision of the population policy document was to decelerate fertility and control the rate of population growth so as to keep pace with the actual capacity for resource generation for development. It is important to observe that the country has today made significant progress, most notably in reducing fertility. The results of the most recent survey, the 1998 Ghana Demographic and Health Survey (GDHS), indicate that there is a dramatic decline in fertility to the tune of about 2 births in a decade. The findings show that the total fertility rate (TFR) slumped from 6.4 births per woman in 1988 (to 5.5 in 1993, and then) to 4.6 births per woman in 1998 (Ghana Statistical Service and Macro International Inc., 1999). Given the prevailing favourable political commitment to population programmes, and the noticeable increase in the participation of grassroots organizations and non-governmental organizations in population management, some demographers are confident that the unfolding demographic transition in Ghana will be greatly accelerated in the next couple of years. However, little is known about the factors responsible for this phenomenal shift in reproductive behaviour. Ghana's demographic transition experience is unique because there is no empirical evidence to suggest any substantial uptake in contraceptive use, though knowledge of contraceptive technologies is virtually universal in the country. It has been suggested that if one desires to find out the commencement of a sustained decline in completed family size, separate from mere short-term fluctuations in fertility or reporting errors emanating from the data being used, one should investigate a number of indicators for evidence (Van de Walle and Foster, 1990; Mauldin and Berelson, 1978). Paramount among these indicators is a conclusive decline in fertility level using comparable data sets. This article therefore seeks to examine the factors that might have accounted for these outstanding rapid changes in reproductive behaviour using the three nationally-representative sample surveys - 1988 GDHS, 1993 GDHS, and 1998 GDHS. As societies transform from a condition of natural fertility (that is a situation whereby couples do not practice intentional fertility control) to that of deliberately controlled fertility, noticeable changes occur in their overall levels of total natural marital fertility, total marital fertility, and total fertility rate. These changes can be attributable to a number of socioeconomic, cultural, and environmental variables mediated through biological and behavioural factors. The biological and behavioural factors are otherwise called intermediate fertility variables or proximate determinants of fertility, and have the defining characteristic of influencing fertility directly. These proximate determinants include: (1) contraceptive use, (2) marriage patterns, (3) lactation, and (4) induced abortion. It has been conclusively empirically shown that changes in these proximate determinants of fertility account for much of the variations in fertility among populations (Bongaarts, 1978; Gaisie, 1984; Akinkumi, 1989; Chimere-Dan, 1990; Nasozi, 1990; Onuoha, 1992). Consequently, this article attempts to examine the relative changes associated with the first three of these proximate determinants of fertility over time using the three rounds of DHS surveys conducted in Ghana. Induced abortion, as a proximate determinant of fertility, is not examined here because no information on it was collected in the DHS programmes, and whatever information one gets on it presently is both fragmentary and unreliable (Cleland and Hobcraft, 1985; Mauldin and Ross, 1994). Data and Methods of Analysis The study utilizes the 1998, 1993, and 1988 Ghana Demographic and Health Surveys (GDHS) raw data files to analyze the course of the fertility transition in Ghana. The GDHS data (particularly the 1998 set) are the most current, nationally representative, stratified, probability sample surveys carried out in Ghana. Although the country has conducted another census in 2000, coming after 16 years subsequent to the 1984 one, the details of the latest headcount, are yet to be made public. In particular, the recent census asked questions on a number of demographic characteristics of the population, and therefore would have been more suitable for this analysis. As a result of its unavailability, the 1988-1998 GDHS data are preferred for this study because they are relatively more recent and therefore more relevant for programme-planning and decision-making. The 1988-1998 GDHS were conducted by the Ghana Statistical Service as part of the world-wide Demographic and Health survey (DHS) programme of the Institute for Resource development/Macro Systems. Households were identified using a two-stage stratified sampling procedure based on the 1984 census enumeration areas. A total of 6,375 households were selected for the 1998 GDHS sample. Out of these, 6,055 households were occupied. Overall, interviews were completed for 6,003 households, which represent 99% of the occupied households. Ninety-seven percent of all eligible women (aged 15-49 years) were successfully interviewed, resulting in a final sample of 4,843 women. Similarly, over 95% of all eligible women were successfully interviewed in the 1993 and 1988 surveys. It should be noted that a detailed description of the sample design and implementation of the three surveys is presented elsewhere (Ghana Statistical Service and Macro International Inc., 1999; Ghana Statistical Service and Macro International Inc., 1994; Ghana Statistical Service and Institute for Resource Development/Macro Systems, Inc., 1989). Fertility will be measured by indices such as Age-Specific Fertility Rate (ASFR), and Total Fertility Rate (TFR). ASFR will be used to examine the age pattern of fertility while TFR will be estimated to identify the level of fertility. To ascertain the authenticity of the reported substantial decline in fertility, analysis of trends in fertility and its correlates will be undertaken. In particular, ASFRs for 0-4, 5-9, and 10-14 years prior to the survey will be analyzed; key features of Ghana's fertility by age (mean age at first marriage, current contraceptive use, mean duration of postpartum infecundability, among others) will be analyzed using the principal data sets. The basic analytical technique used is the Bongaarts model (Bongaarts, 1978, Bongaarts and Potter, 1983). The Bongaarts model summarizes the effect of each of the fertility determinants in an index, which generally ranges between 0-1, with 0 having the greatest inhibiting effect on fertility and 1 having the least inhibiting effect (in other words, the lower the index, the more it reduces fertility and vice versa). In specific terms, the index measuring the effect of marriage patterns on fertility is denoted by Cm. This index takes the value of 1 when all women of reproductive age are in union and 0 when none are union. The index of contraception is depicted as Cc and equals 1 if no contraception is used and 0 if all fecund women use modern methods that are 100% effective. The effect of postpartum amenorrhoea and abstinence on fertility is measured by Ci, the index of postpartum infecundability in such a way that when there is no lactation or postpartum abstinence, Ci equals 1 and when infecundability is permanent, Ci equals 0. The index of abortion is denoted by Ca and equals 1 in the absence of induced abortion and 0 if all pregnancies are aborted. The index of pathological or primary sterility is represented as Cp and assumes the value of 1 in the absence of primary sterility and 0 if all women are sterile. Thus, the Bongaarts model, which estimates TFR as a residual value deriving from the multiplicative effect of these indexes is given as: TFR = TF x Cm x Ci x Cc x Cp x Ca where TF is the level of fertility expected in the absence of any of the eight proximate determinants (proportion married, contraception, induced abortion, lactational infecundability, frequency of intercourse, sterility, spontaneous abortion,and duration of the fertile period)or an assumed biological maximum fertility that is approximately constant across populations. The second part highlights the computational procedures used in estimating the indices of the proximate determinants. Indices of the Proximate Determinants of Fertility 1. Index of Marriage (Cm) where TFR = the average total number of births a woman would have in her lifetime at current age-specific fertility rates, and TMFR = the average total number of births a woman in union from age 15 to 49 would have at current age-specific marital fertility rates. Or simply dividing TFR by the proportion married. Both rates are estimated for the five years prior to the survey in order to provide most current information and vitiate under-reporting of births. It should be noted that the model assumes that all births occur within the
context of marriage. In Ghana, as in many other parts of Africa, a substantial
amount of childbearing occurs outside socially - sanctioned unions. Because
of this, Cm is likely to be greater than 1. Hence, if births outside
marital union are excluded from the analysis, the TFR will be underestimated
while TMFR will be accurately estimated. On the other hand, if births to unmarried
women are included, the TFR will be correctly estimated while the TMFR will
be inflated, thereby giving the erroneous impression that marriage patterns
reduce fertility by a greater proportion than they actually do. To circumvent
this problem and maintain a consistent definition for the other variables in
the Bongaarts framework, Jolly and Gribble (1993) have suggested the addition
of another variable, Mo to the model. The variable Mo
captures the effect on total fertility of births outside union. Mo
links total fertility computed by using all births to total fertility computed
by using births only to women in marriage. Also, a modified version of Cm,
C1m, measures the effect on total fertility of the specific
observed union pattern under the assumption that there are no non-marital births.
The product of Mo and C1m is
Cm, which is the Bongaarts' definition of the effects of marriage
patterns on fertility. The index of marriage Cm is computed as follows: Measured births outside marriage are computed as
Where TUFR (total union fertility rate) is the sum of the age-specific union fertility rates (ASUFR) of women. ASUFR is estimated like the ASFR but here the numerator refers to marital births while the denominator refers to women currently in union. It should be noted that the estimation of TUFR is predicated on the assumption that there is no disruption in marriage from the date of first union if the woman remains married at the time of the survey. This assumption is plausible because in Ghana and other parts of Africa, marital disruptions are quickly followed by remarriage. 2. Index of
Contraception (Cc) The average
use-effectiveness of a method is calculated as the weighted average of the
method-specific use-effectiveness levels, with weights equal to the proportion
of women using a given method. In this article, the following standard
use-effectiveness levels have been employed: Pill = 0.90; IUD = 0.95; Female
Sterilization = 1.00; Other methods =
0.70. where
i = mean number of months of postpartum infecundability (estimated as the mean
number of months of postpartum amenorrhoea or abstinence, which ever is longer)
for women in marriage. The i is estimated via the prevalence/incidence
procedure. where Cppam = index of lactational
amenorrhoea and 4. Index of Primary
Sterility (Cp) where s = proportion of married women between ages 40 and 49 who have never had a child on the assumption that all women must have had their first birth by 40 years of age in Ghana. The ten-year age group of 40-49 is preferred so as to increase the number of women in each subgroup and reduce the standard error in estimating s. 5. Total Natural Fecundity Rate
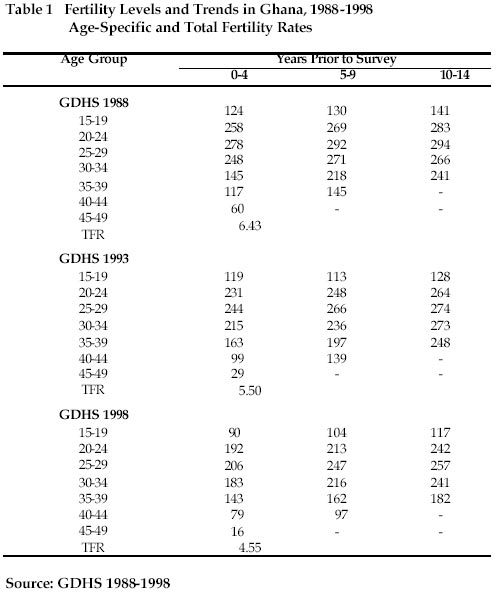
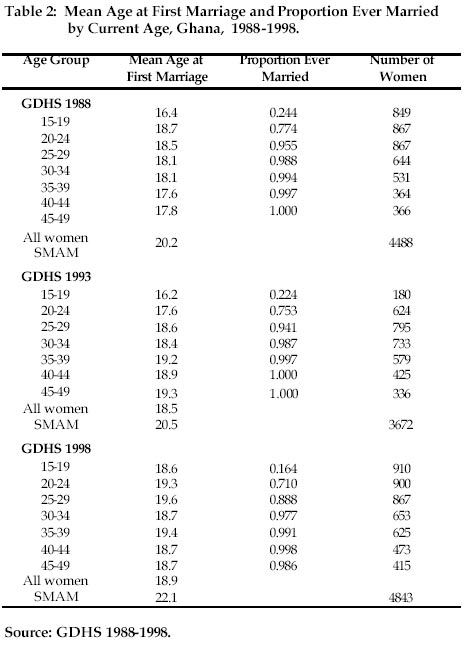
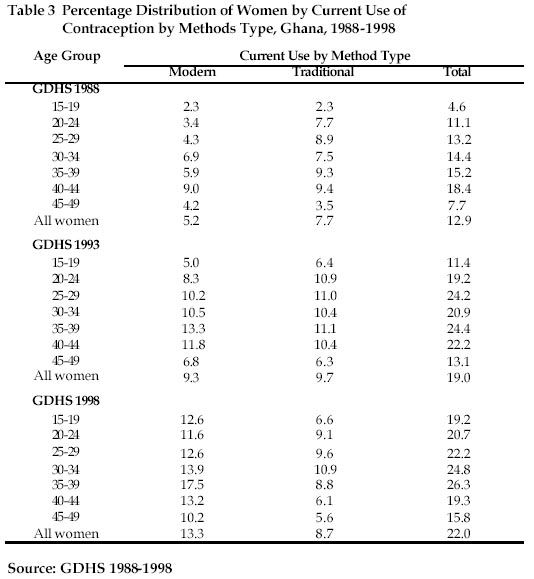
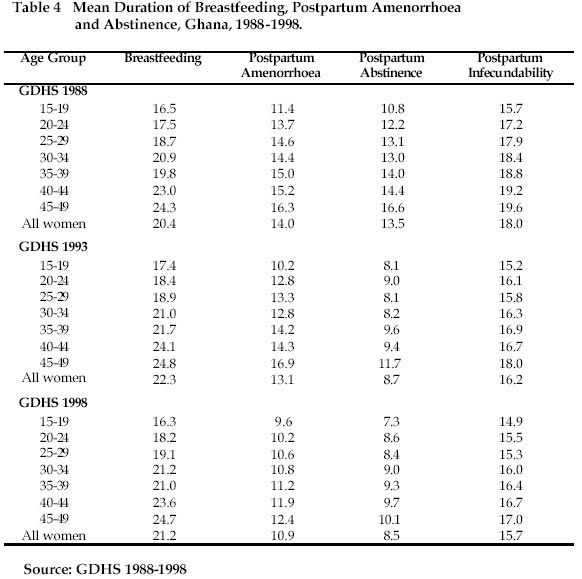
(TF) Lastly, in order to identify categorically which segment of the female population is undergoing most fertility change, the study will investigate differentials in levels of contraceptive use, marriage, and first births over time by selected background characteristics (age, place of residence, education, and region of residence). Results of the Analysis Fertility Levels and Trends An examination of trends in current fertility (age-specific fertility rates) and cumulative fertility (total fertility rates) brings to the fore the demographic transition unfolding in Ghana[1]. Table 1 shows that fertility has fallen in all age groups, especially among women within the age bracket of 15-34 over the decade. The result is that TFR fell from 6.4 in 1988 to 5.5 in 1993 and then to 4.6 in 1998, representing a decline of 28% or about 2 births per woman. The ASFRs for the five-year period before the survey further substantiate the fact of reproductive revolution in Ghana. The evidence suggests that there has been a significant reduction in ASFRs from 10-14 years preceding the 1998 survey (which more or less is coincidental with the 1983-1988 period), to 0-4 years preceding the survey (which coincides with 1993-1998 period). Consequently, it can be contended that the wind of change in favour of small family size is blowing across Ghana. But it is not clear what factors that have accounted for this dramatic fertility decline in Ghana. There is, therefore, need to investigate the role of the proximate determinants of fertility in an attempt to explain the phenomenal change in Ghana's fertility. Age at First Marriage and Proportion Married Age at first marriage identifies the onset of exposure to continuous and socially sanctioned childbearing. Implicitly therefore, the earlier a woman marries, the longer her reproductive life span, ceteris paribus. Here, age at first marriage refers to the ages reported by the respondents as those at which they began their first marital relationships. Table 2 indicates the mean age at first marriage and proportion of women who are currently or previously married (ever married) for the period under review. The mean age at first marriage varies from about 16 years for women aged 15-19 to about 19 years for women aged 45-49 years between 1988 and 1993. This might be due to the few number of women who were married at the younger ages and recall lapse of age at marriage for the older women. A notable exception, however, is with the 1998 data set. The results show that the mean age at first marriage is about 19 years across all age groups. The findings point to the fact that mean age at first marriage is likely to be increasing in Ghana. This increase is confirmed by a rise in the singulate mean age at marriage (SMAM) from about 20 years in 1988 to 22 years in 1998. The SMAM is the mean age at first marriage among those who ever marry (United Nations, 1983). The evidence from the 3 data sets, however, reveals that by age 40, almost all the women have married, implying universality of marriage in Ghana. Contraception Contraception has a direct negative impact on fertility. The use of contraceptive methods has not significantly risen in Ghana over the ten-year period. Table 3 indicates that contraceptive prevalence rate rose from 13% in 1988 to 19% in 1993 and then to 22% in 1998, representing an increase of only 69%. In particular, use of modern contraceptive methods stood at only 13% by 1998. It appears that the family planning programme efforts at both governmental and nongovernmental levels have not paid off, especially when one notes that the Planned Parenthood Association of Ghana (PPAG) was formed in 1967, and in May, 1970, the Government established the Ghana National Family Planning Programme (GNFPP). It should be noted, however, that rate is more concentrated at older ages, suggesting that the younger women are more interested in procreation than using contraception either for spacing or stopping of births. An important development concerning contraception in Ghana is that whereas traditional methods were more prevalent in the late 1980s, the modern methods have become more popular since the late 1990s. Breastfeeding, Postpartum Amenorrhoea, Abstinence, and Infecundability Lactation (breastfeeding) and postpartum practices (amenorrhoea and abstinence) are associated with fertility. Postpartum amenorrhoea refers to the temporary disappearance of menstruation after childbirth at which period a woman becomes non-susceptible to conception. Various studies have established a direct relationship between the length and intensity of breastfeeding and the duration of postpartum amenorrhoea (Bongaarts and Potter, 1983; Gutmann and Fliess, 1993; Mbamaonyeukwu, 2000). Postpartum abstinence refers to the period of voluntary sexual inactivity following childbirth. Thus, women are considered infecundable if they are not exposed to the risk of conception either because they are amenorrhoeic or are abstaining from sexual intercourse after childbirth. Stemming from its defining characteristic, postpartum infecundability is one of the four proximate factors through which economic, social and other factors operate to influence fertility. Table 4 shows the mean duration (in months) of breastfeeding, postpartum amenorrhoea, abstinence and infecundability by age between 1988 and 1998. The table reveals that Ghanaian women breastfeed their infants for about two years. This is quite encouraging, especially when viewed against the background of the nutritional benefits of breast milk. The table shows that this scenario has not changed much over the years. The results indicate that the older women consistently breastfeed for longer periods than the younger ones. The finding seems to suggest a sharp fertility decline in Ghana without significant changes in breastfeeding behaviour. This finding supports the argument of Casterline (1994) that fertility deceleration may not be correlated with remarkable changes in breastfeeding behaviour. Table 4 further shows that Ghanaian women were slightly more postpartum amenorrhoeic in 1988 than in 1993 and 1998. A similar picture emerges when postpartum abstinence and postpartum infecundability (PPI) are considered. In fact, while PPI was 18 months in 1988, it declined to about 16 months in 1993 and 1998. Impact of the Proximate Factors
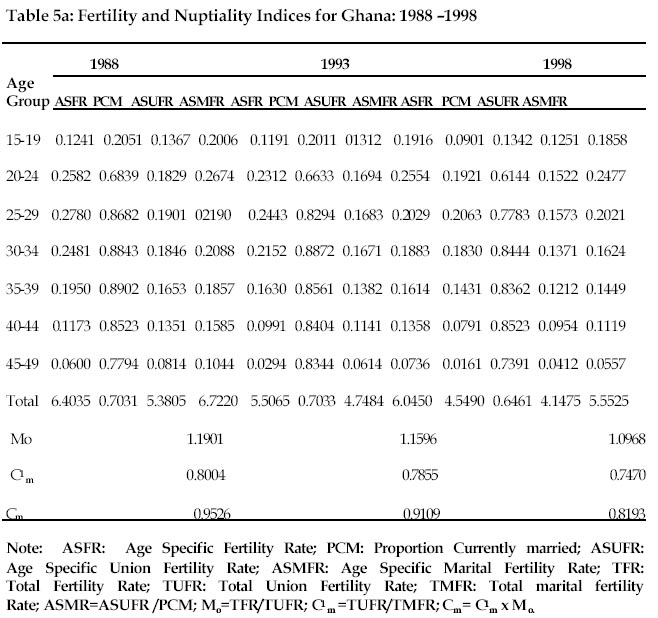
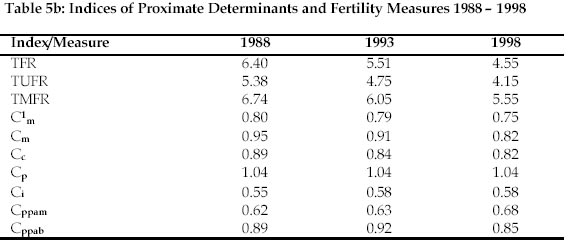
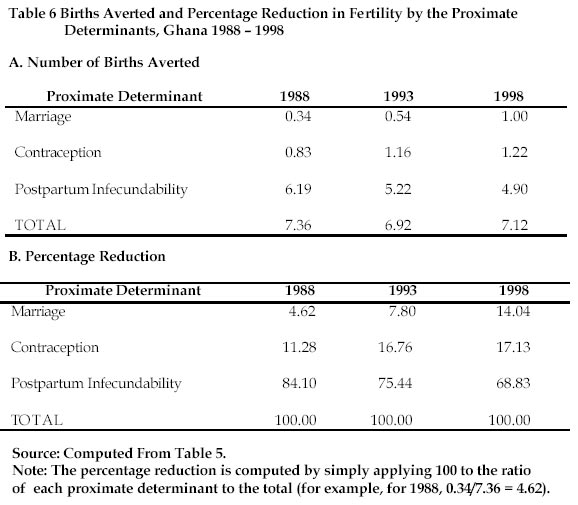
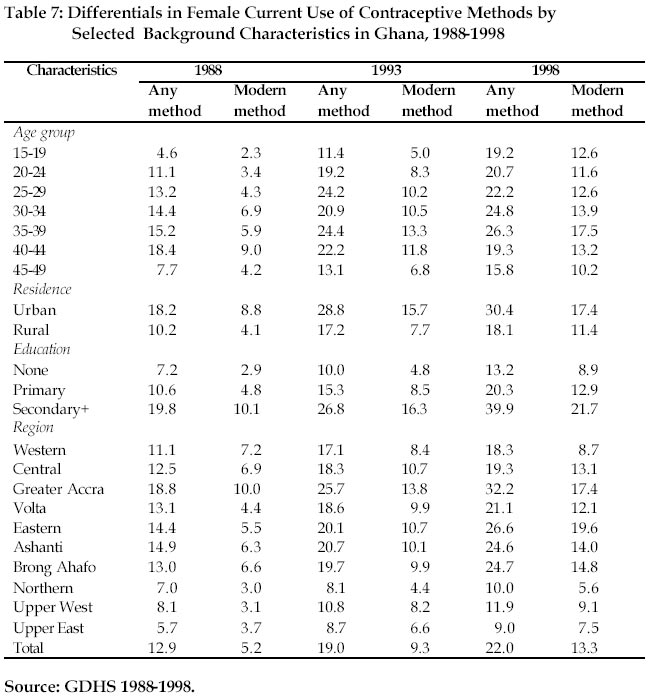
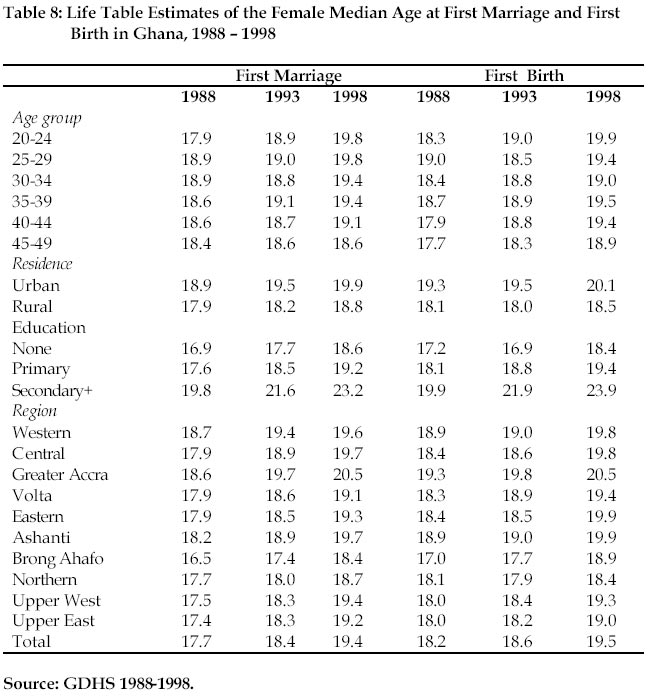
The findings depicted in Tables 5a and 5b illustrate the relative contribution of each of the proximate determinants to the observed differences in fertility levels in Ghana over the study period. It should be remembered that the lower the index, the greater the inhibiting effect it has on fertility, the reducing effect being the complement of the index value. The results reveal that Cm dropped from 0.95 in 1988 to 0.91 in 1993 and then to 0.82 in 1998. C1m also fell from 0.80 in 1988 to 0.79 in 1993 and then to 0.75 in 1998. In other words, marriage patterns reduced fertility by only 5% in 1988, 9% in 1993, and then by 18% by 1998. This means that if marriage were universal for all women of reproductive age, the observed TFR would increase, ceteris paribus, by 5%, 9% and 18% in 1988, 1993 and 1998 respectively. On the other hand, when premarital births are excluded, and all women marry and remain in marriage within the reproductive age bracket, then the TFR would have increased by 20% in 1988, 21% in 1993 and 25% in 1998 in Ghana. A closer look at the effects of marriage patterns by age (Table 2) reveals that the greatest fertility reducing effect of marital patterns is found at the age group 15-19, followed by 20 - 24 age group. An interesting trend emerges when the effect of births outside marriage is considered. The results indicate that the effect of Mo in 1988 was 1.19. This implies that the TFR was 19% higher than it would have been if all childbearing was confined to the marriage institution. By 1993 the effect of Mo was 1.16 while in 1998, it was 1.10, implying that the TFR had decreased by 16% and 10% in 1993 and 1998, respectively. These findings seem to suggest that there is a reduction of premarital births in the Ghanaian society. This is a welcome development because childbearing is generally sanctioned through marriage in many parts of Africa. The findings show that Cm has declined from 0.95 in 1988 to 0.91 in 1993 to 0.82 in 1998. A plausible explanation for this decline is the increase in both age at first marriage and never married women (Rutenberg and Diamond, 1993). Lastly, the Cm values have been consistently higher than the C1m values (0.95 versus 0.80 in 1988, 0.91 versus 0.79 in 1993, and 0.82 versus 0.75 in 1998). This finding suggests that marriage patterns have a fairly large effect in reducing fertility. Furthermore, in estimating the fertility-inhibiting effect of marriage patterns using births in union only, the probability of underestimating the overall effect of Cm on total fertility, though declining, is high. The empirical evidence presented in Table 5b clearly shows that contraception has the lowest fertility inhibitive effect in Ghana than the other proximate factors. Between 1988 and 1998, the index values of contraception (Cc) only dropped mildly from 0.89 to 0.82. However, it is important to observe that the inhibitive effect of contraception has been steadily gaining strength in Ghana. It should be noted that because of the few number of contraceptors across various age groups within the reproductive age category, it is not appropriate at this time, to quantify the index values of contraception by age group with a view to finding out where the fertility - inhibiting effects of contraception are strongest. But suffice it to say that a rise in the prevalence of conceptive use has resulted in the strengthening of the inhibitive effects of contraception on fertility over the decade in Ghana. A further examination of Table 5b reveals that postpartum infecundability (PPI) plays a pivotal role in explaining recent reproductive change in Ghana. The findings indicate that the index of PPI, Ci, had the smallest values (0.55 in 1988, 0.58 in 1993, and 0.58 in 1998), and therefore had the largest fertility-inhibiting effect of all the proximate factors. Consequently, the relative importance of PPI in explaining fertility change is substantially larger than that of any other proximate determinant in Ghana. This finding is consistent with results from other parts of Africa (Mbamaonyeukwu, 2000; Robinson, 1992). It should, however, be remarked that the fertility transition that is underway in Ghana has been accompanied by a mild weakening of the fertility-inhibiting impact of PPI (from 0.55 in 1988 to 0.58 in 1998). This pattern is consistent with that suggested by Bongaarts and Potter (1983) who argue that a typical movement from natural to controlled fertility is usually accompanied by a shortening of PPI (Table 4). It is important to note that this shortening of PPI is occurring at a time when both contraceptive use and mean age at first marriage are on the increase. The GDHS results show that in 1988, 4% of women aged 40-49 were childless while in both 1993 and 1998, 3% of these women were childless, a figure that is similar to the standard rate of childlessness in developing countries (Bongaarts et al. 1984; Frank 1983; Bulatao, 1984). Applying these values to the formula used in estimating the index of sterility yields approximately 1.04 over the decade which is greater than 1. It is difficult to interpret such a result within the context of the analysis of proximate determinants of fertility. Nevertheless, the results as depicted in Table 5b are suggestive of the fact that childlessness or pathological sterility did not play any significant role in the reproductive revolution Ghana is currently experiencing since the index value does not inhibit fertility below its theoretical maximum of unity. Relative Contribution of the Proximate Factors Having established the fertility-inhibiting effects of the proximate determinants, in what follows an attempt is made to quantify the effects of these proximate factors in terms of births averted and percentage reduction in fertility. Employing the formulae proposed in the Bongaarts model, the following steps are taken to capture births averted due to the effects of the proximate determinants: the effect of marriage is measured using TMFR - TFR, where TMFR = TFR/Cm; the effect of contraception is measured by TNMF-TMFR, where TNMF = TFR/(Cm x Cc); and the effect of PPI is measured by TF - TNMF, where TF=TFR/(Cm x Cc x Ci). The results of this exercise are presented in the first and second panels of Table 6. The findings indicate that marriage patterns reduced fertility in Ghana by about 0.3 births in 1988, 0.5 births in 1993 and 1.0 births by 1998. Thus, marriage patterns led to a larger decline in fertility in 1998 (representing 14%) than in 1993 and 1988. Contraceptive use reduced fertility by about 0.8 births in 1988 but the modest increase in contraceptive use in the country led to a reduction in fertility to the tune of about 1.2 births in 1993 and 1998, showing an increase from 5% to 17% over the period. The results shown in the table further reveal that observed fertility would have increased by about 7.4 births in 1988, 6.9 births in 1993 and 7.1 births in 1998, in the absence of postpartum infecundability. In other words, postpartum infecundability reduced fertility by about 84% in 1988, 75% in 1993, and 69% in 1998. The findings clearly show that the greatest reduction in Ghana's potential fertility is due to the impact of postpartum infecundability, although this is weakening with the passage of time. Extent of Reproductive Revolution In order to clearly show the pattern of fertility decline and underscore where the transition is most pronounced, two further levels of analysis are conducted. The first is an investigation of differentials in female contraceptive use by selected background characteristics, while the second is the life table estimation (Namboodiri and Suchindran, 1987) of the female median age at first marriage and first birth in Ghana for the period under review. The results of the former are presented in Table 7, while the results of the latter are shown in Table 8. The findings indicated in Table 7 reveal that the contraceptive revolution occurring in Ghana is generally a universal phenomenon, affecting all age groups, and persons of all residential, educational, and regional affiliation. However, the transition is more pronounced between 1988 and 1993 (47.3% increase for all methods) than between 1993 and 1998 (15.8% increase for all methods). Also, as expected, the women residing in urban areas and those of them with higher education have experienced consistent contraceptive uptake more than others. The reasons for this are obvious. People who live in urban areas and who have higher education are always the first recipients of the benefits of technological advancement and the spread of the western and modern values. As a result, those regions of Ghana that are more developed have the highest use of contraception - Greater Accra (where the nation's capital is situated), Ashanti (a very important commercial centre), Eastern, Brong Ahafo, and Volta. Table 8 shows the life table estimates of the median age at first marriage and first birth during 1988-1998. Age at first marriage has been recognized as a crucial determinant of fertility because it marks the beginning of exposure to the risk of childbearing in most societies. In fact, empirical studies suggest that women who marry early have larger completed families (Trussell et al., 1985; Hoem and Smelser, 1984; Trussell and Menken, 1978; Caldwell et al., 1992; Cheng and Rajulton, 1992; Goldscheider, 1992). Consequently, an increase in the age at first marriage is expected to lead to a visible fertility decline, ceteris paribus. The table reveals a consistent trend toward later marriage, and this trend has been accompanied by a corresponding pattern of later motherhood. The median age at first marriage increased from 17.7 years in1988 to 18.4 years in 1993, and then to 19.4 years in 1998. Similarly, the age at first birth increased from 18.2 years in 1988 to 18.6 years in 1993, and then to 19.5 years in 1998. The similarity between the evolution of marital and childbearing behaviour is particularly striking among the youngest women (20-24). This is because while their age at first marriage increased by 23 months during the study period, their age at first birth increased by 18 months. However, the median age at first birth is lower than the median age at first marriage in 1988 (for 25-29, and 40-49 age groups), in 1993 (for 25-29, 35-39, and 45-49 age groups), and in 1998 (for 25-34 age group). The lack of correspondence between the evolution of age at first marriage and age at first birth at these ages is suggesting a considerable increase in premarital childbearing. The high level of premarital childbearing is probably related to the fact that there is little pressure on the women to enter marriage because of pregnancy. Another contributing factor is Ghana's (and indeed Africa's) distinct cultural definition of marriage. Marriage, unlike what obtains in much of the developed world, can be regarded as a relatively long and fluid process rather than a single well-defined event. Since the date of marriage can be arbitrarily placed at any point during that process, women may tend to date marriage after the birth of their first child. Table 8 further indicates that the extent of the dissociation between marriage and childbearing varies by the selected background characteristics. The median age at first marriage is lower than the median age at first birth for women living in rural areas, those without any education, and among those living in Northern, Upper West, and Upper East regions in 1993 and 1998. This may imply the prevalence of premarital conception and childbearing in these areas. These population subgroups are the least developed, have a strong adherence to traditional concepts of marriage and family. They, generally, enter marriage earlier and may be more likely than others to be partners in polygynous relationships. Discussion and Policy Issues The present article has attempted to assess the role and relative importance over time of three proximate determinants of fertility with respect to the reproductive revolution currently underway in Ghana using the three DHS surveys conducted in the country. The findings show that the fertility-inhibiting effect of postpartum infecundability is more significant than the effects of marriage patterns and contraception. The effect of contraceptive use is next in importance in inhibiting fertility. However, the results reveal that there is the erosion of postpartum practices over time. The percentage reduction attributable to PPI declined from 84% in 1988 to 69% in 1998. On the other hand, the inhibiting effects of contraception and marriage increased remarkably over the decade. The results further show that there is a reduction in non-marital fertility since Mo decreased over time. Another important finding of this analysis is that there is an appreciable drop in total fertility rate in Ghana as evidenced from the trend analysis presented in Table 1. This has occurred at a time when there is noticeable uptake in contraceptive use and a rise in age at first marriage and first birth. It should be noted, however, that although the findings have shown that both age at first marriage and age at first birth have increased in Ghana during 1988-1998 period, the greatest change has been noticed among the youngest age group, as well as among women with higher education, and who live in urban areas, and Greater Accra, Ashanti, and Eastern regions. Nevertheless, it can be contended that the current reproductive revolution underway in Ghana may not be the product of short-term fluctuations in fertility or data errors. The current data do not permit investigating the role of informal networks in the diffusion of innovations and the evaluation of new behaviour in Ghana. However, it can be contended that conversations with other people might have spread information that might, on the one hand reinforced prevailing social norms, and on the other hand, provided a venue for the consideration of behavioural change. Granted that it is difficult to observe the process of diffusion directly, yet it is likely that diffusion of ideas could have occurred through networks of personal communication in Ghana. Through informal conversations, the women might have learnt about new ideas and techniques. Consequently, they might have learnt what their relatives and friends thought about the benefits of prolonged breastfeeding and child spacing, as well as the pros and cons of using contraceptive methods to limit family size, in addition to the adverse implications of early marriage. If this argument is true, then social interactions might have served not only to spread information, but also to alter more general conceptions of the family. Another closely related factor that might have precipitated fertility decline in Ghana is the imitation of behaviour inspired by the modern media and the exchange with non-Ghanaian (and for that matter, non-African) societies. This imitation essentially begins with the Western-educated elite. These individuals, in the first instance, tend to keep traditional values upon return from abroad, as a way to secure their reintegration into the community life. But in the process of time, they become vectors of change, especially women, who bear the heaviest burden of childbearing and childrearing. The results of this analysis have important implications for policy development and programme planning in Ghana. If the observed trend intensifies, contraceptive use is likely to replace PPI as the dominant fertility-inhibiting effect as more and more women will be utilizing contraception for purposes of either spacing or stopping births. Therefore, the current family planning programme efforts at both governmental and nongovernmental levels should be vigorously pursued so as to raise contraceptive prevalence rate and hence further reduce fertility. Rising levels of mean age at first marriage for women is clearly an evidence of rising levels of educational opportunities. The current emphasis on the education of the girl child should be intensified so as to further reduce marriage at an early age. Moreover, sufficient female education acts as a catalyst in changing pronatalist tendencies, empowers the woman, and prepares her for gainful employment outside the home, all of which have a negative influence on fertility. Overall, the findings of this study show that the fertility-inhibiting effects of postpartum infecundability are more important than the effects of contraception and marriage patterns. Consequently, the promotion of prolonged breast-feeding durations should continue to receive the attention of the government and other stake holders because long durations of lactation inhibit fertility. Moreover, the nutritional benefits of breast milk to children are well documented. References
[1] Because the thrust of the present paper is not on levels and trends of fertility per se, time and space constraints preclude investigating the 'true' levels of fertility during this period by the application of indirect techniques. Copyright 2002 - Union for African Population Studies |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}