 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 17, No. 1, May 2002, pp. 103-124 Impact of HIV/AIDS on Fertility in Sub-Saharan Africa James P.M. NTOZI Department of Population Studies, Institute of Statistics and Applied Economics, Makerere University, Kampala, Uganda. Code Number: ep02006 Abstract One of the impacts of HIV/AIDS on individual women and populations in severely affected areas of Sub-Saharan Africa is change in fertility levels. HIV/AIDS has influenced fertility of individual women through proximate determinants of fertility, namely, marriage, contraception, pregnancy, abortion, breastfeeding, postpartum abstinence, pathological sterility and natural fecundity. Fertility may decline in the era of HIV/AIDS because of delayed onset of sexual relations and age at first union, reduced premarital sexual relations and remarriage and increased marital dissolution. Desired family size and condom use are also increased. HIV infected women experience reduced pregnancy rate and rising levels of induced and spontaneous abortion. HIV/AIDS induces sterility, increases foetal mortality and decreases frequency of sexual intercourse and production of spermatozoa. In contrast, the epidemic may increase fertility due to reduced extra marital relations, polygyny, breastfeeding, postpartum abstinence, STD prevalence and spousal separation, increased infant mortality and switching to condom use from more effective contraceptives. Examples of sites in Tanzania, Uganda and Zambia indicate that fertility has declined in populations hard hit by HIV/AIDS epidemic. However, it will take long durations of high HIV/AIDS prevalence to reduce fertility at a national scale. RésuméDans les zones de l'Afrique au Sud du Sahara à forte prévalence du VIH/SIDA, l'un des impacts sur les femmes tant au niveau individuel qu'à celui de la population de manière globale est sur le taux de fécondité. Le VIH/SIDA a affecté la fécondité des femmes au niveau individuel à travers les déterminants comme le mariage, la contraception, la grossesse, l'avortement, l'allaitement maternel, l'abstinence post-partum, la stérilité pathologique et la fécondité naturelle. A cause du démarrage tardif des relations sexuelles, de l'âge au premier mariage, de la diminution des rapports sexuels avant mariage et de l'augmentation des séparations, la fécondité peut baisser à l'ère du VIH/SIDA. En outre, plus de gens optent pour une famille réduite et une utilisation plus systématique du condom. Les femmes atteintes de Sida ont tendance à réduire le taux de grossesse et à augmenter les avortements spontanés provoqués. Le VIH/SIDA entraîne la stérilité, augmente la mortalité fœtale et diminue la fréquence des rapports sexuels et la production des spermatozoïdes. Par contre, l'épidémie peut engendrer une hausse de la fécondité à cause de la baisse des relations sexuelles hors mariage, la polyginie, l'allaitement maternel, l'abstinence post-partum, la prévalence des MST et les divorces, mais également la mortalité infantile et l'utilisation du condom en lieu et place de contraceptifs plus efficaces. Des exemples de sites tirés de la Tanzanie, de l'Ouganda et de la Zambie montrent que la fécondité des populations touchées par la pandémie du Sida baisse. Par contre, pour que le taux de fécondité au niveau national soit affecté par la prévalence du VIH/SIDA, il faut du temps. Introduction It is now two decades since the first case of HIV was diagnosed. Since the onset of HIV/AIDS all regions of the world have experienced the pandemic. According to UNAIDS/WHO (2000) by December 2000, a huge 36.1 million people including 16.4 women and 1.4 million children aged below 15 years had been living with the disease. Of these 21.8 million people, 9 million women and 4.3 children have died due to the epidemic. This means that HIV/AIDS has had a heavy toll of human lives and adversely affected many activities in the world. The impact of the epidemic has included: increased morbidity rates, higher infant, childhood and adult mortality, a large number of orphans and widows, deterioration of health sector, poorer households, reduced agricultural output, disrupted business activities, adverse effects on education and fertility change. Research on impact of the epidemic on fertility has recently received some attention. In their study of 412 HIV infected women in Paris and south east of France from 1988 to 1993, De Vincenzi et al (1997) found that the incidence of pregnancy decreased significantly from 20.4 per 100 person years before HIV diagnosis to less than half, 7.9 per 100 person years after HIV diagnosis. The study also showed that the proportion of pregnancies voluntarily interrupted more than doubled from 29 to 63% between before and after HIV diagnosis. The percentage of spontaneous abortions and ectopic pregnancies increased significantly from 8.3 to 25.4 of those conceived before and after HIV diagnosis, respectively. Also the proportion of women who were sexually not active rose four times from 5 per cent before diagnosis to 20% after diagnosis. Similar results were observed in Italy by D'Ubaldo et al (1998), who studied a cohort of 423 women from 12 cities. It was found that among the HIV-1 positive women a lower proportion of 62.3% compared to 67% of the HIV-1 negative women reported at least one delivery of a baby. Conversely, 19.4% of the HIV-1 positive women claimed to have experienced a miscarriage, higher than 15% of the HIV-1 negative women. A fitted logistic regression model indicated that HIV-1 infection was associated with miscarriage with odds ratio of 1.67. Also, 62.9% of the HIV-1 infected women had intentional abortion, compared to a lower proportion of 45.4% of the HIV-1 uninfected women. Three explanations in form of hypotheses were offered by D'Ubaldo et al (1998) for the relationship between HIV-1 infection and spontaneous abortion. First, the direct effect of HIV-1 on the placenta or on the development of embrio. Damage of the placenta interferes with the normal transfer of nutrients including oxygen from the maternal blood to the foetus, resulting in fetal death and expulsion. Also, abnormal development of embryo results into a non-viable fetus, which is subsequently expelled. The second hypothesis is that HIV-1 infection causes abnormalities or injury of the fetal thymus gland. This results into altered production of enzymes and leads to a hostile uterine environment that does not allow continuation of the pregnancy. The third explanation is that both HIV-1 infection and the pregnancy itself depress the mother's immunity. This encourages opportunistic bacteria and viruses to ascend from the lower genital tract (vagina and vulva) into the uterus causing infection of the placenta, which interferes with the transfer of nutrients/oxygen to the foetus leading to its death. More evidence on the relationship between HIV/AIDS and fertility was reported in four states of Australia among 294 women whose medical records in early 1990s were reviewed (Thackway et al 1997). It was found that of the women who had had at least one pregnancy, a much lower proportion (38%) became pregnant after HIV-1 diagnosis than 62% who were pregnant before knowing that they were HIV-1infected. Of the pregnancies recorded to have occurred after HIV-1 diagnosis, only 44% were continued to full term, while a high 47% were terminated and 9% ended as miscarriages. Out of three pregnancies confirmed after AIDS symptoms had appeared two were terminated. This pregnancy termination rate was much higher than 19% to 26% experienced in the Australian states of the study. It is possible to attribute the high termination rates to fears of mother-to-child transmission and faster progression of the disease in the body. Furthermore, the general fertility rate for the women in the study aged 15 - 44 years was only 29.6 per 1000, much lower by 53% than the rate (63 per 1000) for Australian women in the same age group and during the same period. Also the adjusted birth rate in the study population was under one-half (45%) that of the overall birth rate in Australian women. The reasons for lower birth rate in HIV-1 infected women were threefold (Thackway et al 1997). First, women were likely to have used condoms to reduce HIV risks and avoid more pregnancies. Second, these women were likely to have reduced sexual activity following their HIV-1 diagnosis. It should be noted that perhaps for these two reasons only three out of fifty eight women were pregnant after AIDS stage was diagnosed. Third, the huge number of pregnancy terminations had a depressing impact on the fertility rate, which is computed using the number of live births only. Given the above evidence in the developed world with advanced facilities of testing for HIV and counseling women about the implications of HIV infection on pregnancies, it is the intention of this paper to study the relationship of the epidemic and fertility in Sub-Saharan Africa. Before this relationship is investigated, the paper reviews the situations of HIV/AIDS and fertility in the region. HIV/AIDS in Sub-Saharan Africa Sub-Saharan Africa has been the most severely affected world region by the epidemic. With 25.3 million people ever infected by HIV, Africa is a home of 70% of adults and 80% of children living with HIV in the world, and has buried three-quarters of 21.8 million who died of AIDS by end of 2000 (UNAIDS/WHO 2000). The region has the highest adult prevalence rate of 8.8% in 2000 in the world, which is as high as 35.8% in Botswana. The epidemic has been in the region for about two decades and has affected every country. In the 1980s and early 1990s the epidemic was experienced mostly in Eastern and Central Africa, where the HIV prevalence of women attending antenatal clinics were as high as 30% in some sites in Uganda. Since the late 1990s the epidemic increased rapidly in the Southern African countries with high prevalence record of 35.6% in Botswana, 23.6% in Lesotho, 16% in Malawi, 13.2% in Mozambique, 19.5% in Namibia, 19.9% in South Africa, 25.3% in Swaziland, 20% in Zambia, and 25.1% in Zimbabwe. With the exception of Mozambique the prevalence in Southern Africa is at least 16%. In Eastern Africa, the prevalence is between 5% and 15%. The prevalence in Central Africa is also between 5% and 15%, except Angola and Gabon with lower rates. With the exception of Cote D'Ivoire, Nigeria, Burkina Faso and Togo, West Africa's prevalence is below 5%. The lowest prevalence at less than 1% in Africa is in North Africa. Because the main mode of transmission of HIV in Sub-Saharan Africa is heterosexual, most of the HIV infected adults are women, forming 55% of the total. This means that the impact of HIV/AIDS on fertility could be serious, since it is the women who are most concerned with bearing of children. Fertility in Sub-Saharan Africa For a long time now Sub-Saharan Africa has led other regions in levels of fertility. At an estimated average level of about 6 children per woman, the region has the highest levels in the world. However, recently some countries in the region have experienced major fertility declines to total fertility rates below 5.0. The countries include: Botswana from 7.1 in 1981 to 4.4 in 1995-2000, Ghana from 7.2 in 1960 to 4.5 in 1998, Kenya from 8.0 in 1975-77 to 4.6 in 1998, South Africa from 6.4 in 1960 to 3.1 in 1995-2000, Swaziland from 6.9 in 1966 to 4.8 in 1995-2000, and Zimbabwe from 8.3 in 1969 to 4.0 in 1996-99. Most other African countries are currently undergoing modest fertility declines. Nevertheless, there are as many as 16 countries in the region with either constant or increasing levels of fertility (UN 2000). Five of these have displayed fairly constant but high levels of fertility since 1950s, namely Burundi at total fertility rate of 6.8, Mali at 7.1, Somalia at 7.2, Togo at 6.6 and Uganda at 6.9. The remaining eleven countries have actually experienced a rise in total fertility rates between 1950s and 1990s, including Angola from 6.4 to 7.2, Chad from 5.8 to 6.6, Congo from 5.7 to 6.3, Democratic Republic of Congo from 6.0 to 6.7, Equatorial Guinea from 5.0 to 5.9, Gabon from 4.1 to 5.2, Guinea Bissau from 5.1 to 6.0, Liberia from 6.3 to 6.8, Malawi from 6.8 to 7.2, Mozambique from 6.2 to 6.5 and Sierra Leone from 6.1 to 6.5. Many factors have been responsible for influencing fertility changes in Sub-Saharan countries. These have included cultural, social, economic and health factors. With the severe HIV/AIDS epidemic for almost two decades and continuing, it is important to investigate its effect on fertility in the region, so that we know what changes might have taken place in the past and what to expect in future. Impact of HIV/AIDS on FertilityMany studies investigating the impact of HIV/AIDS in several Sub-Saharan African countries have been done. Perhaps, the best way to summarize the studies is to use the proximate determinants of fertility as a conceptual framework. Table 1 shows that depending on the mechanism specified, fertility can decline or even increase due to HIV/AIDS.
With marriage, which exposes women to sexual relations, individual women are likely to respond to HIV/AIDS epidemic by delaying their first sexual intercourse, and for those already sexually active reduce premarital sexual relations due to fear of infection. There is also a possibility of girls postponing their marriage or deciding not to marry at all. Those women married may decide to separate with unfaithful spouses to avoid infection. Due to increased death of partners, more women become widows, which reduces their reproductive lifetime. The widows and divorced women find it more difficult than before to remarry for lack of suitors who fear possible HIV infection. All these behavioural actions reduce the exposure of women to pregnancy and hence depress fertility. However, owing to educational campaigns, which discourage multiple partnerships, men may decide to stick to one wife and hence polygyny is reduced. Increased monogamy may mean higher fertility for individual women. The mechanism of contraception may mean HIV infected women having higher or lower fertility. HIV infected women may be concerned with the likelihood of transmitting infection to their babies and do not want to leave additional children as orphans and hence use contraceptives to stop a pregnancy happening, leading to lower fertility. Other women may want to protect themselves from further infection of HIV and STDs, which would increase progression of the disease. The HIV negative women are likely to increase uptake of condoms in order to protect themselves against HIV infection and STDs. This would depress fertility. On the other hand, in light of high HIV/AIDS related infant mortality both HIV infected and uninfected may desire more children in order to ensure that the preferred minimum number survive and to replace the dead children or even other loved dead relatives. Secondly, in order to increase protection against HIV/AIDS, women using efficient contraceptives such as the pill would switch to using condoms, which may be less efficient in preventing pregnancies, resulting in higher fertility. Demographic and Health Surveys in Sub-Saharan Africa have reported that some couples do not know how to use condoms correctly and others find condoms inconvenient to use. Through abortion, HIV/AIDS may lead to fertility reduction. As seen above in case of France and Italy, HIV infection has the biological effect of increasing spontaneous abortions. The infected woman may also voluntarily terminate a pregnancy for fear of disease progression and wanting to save the baby from vertical infection, as in the case of Australia. It is expected that the two proximate determinants, breastfeeding and postpartum abstinence can increase fertility. To avoid mother-to-child transmission of HIV, women may decide to reduce breastfeeding. In communities practicing long postpartum abstinence, women may reduce the duration to discourage regular partners from engaging in extra marital relationships that may result in infection of HIV of the family. With increased deaths of infants due to HIV/AIDS, women would automatically stop breastfeeding and postpartum practice, attracting early pregnancy and hence higher fertility. Pathological sterility would affect fertility positively or negatively. By causing sub-fecundity, HIV-1 induces sterility and hence depresses fertility. Conversely, through massive interventions of condom use and increased access to treatment, STDs have been greatly reduced. This means that more women are less pathologically infertile, leading to increased fertility. HIV/AIDS can work through natural fecundity mechanism to affect fertility. First, foetal deaths through spontaneous abortion and stillbirths due to HIV infection reduces the live births which are used in the calculation of fertility. Second, because of frequent sickness due to HIV/AIDS, women are less able to engage in sexual intercourse and hence less exposed to getting pregnant. Third, due to reduced nutrition and deteriorating health due to HIV/AIDS, men produce fewer spermatozoa and become less able to impregnate their partners. Fourth, efforts to stick to one partner encourages couples to avoid long spousal separation, which would promote frequent sexual intercourse and create more chances for pregnancies, leading to higher fertility. Evidence of Impact of HIV/AIDS on Fertility in Sub-Saharan Africa Over time data has been collected on HIV/AIDS and proximate determinants of fertility in various parts of Sub-Saharan Africa. This section will present this data and evaluate how it demonstrates the influence of the epidemic on fertility. Briefly, individual women's fertility is affected through biological and behavioural effects of HIV/AIDS on proximate determinants of fertility, including marriage, contraception, pregnancy, abortion, breastfeeding, postpartum abstinence, pathological sterility and natural fecundity. At the societal level the effects of HIV/AIDS on population are based on selected studies in the region. Marriage Following a long period of HIV/AIDS epidemic in Uganda, several studies show that sexual behaviour of several population groups is changing. Asiimwe-Okiror et al (1997) did a population-based knowledge, attitudes and behavioural (KAB) studies of 1500 - 1600 adult women and men aged 15 - 49 years old in 5 urban and rural districts of Uganda in 1989 and 1995. These studies found that during the 6-year inter-study period, the onset of sexual relations had significantly decreased. The proportions of male and female youth aged 15 - 19 years old, who had never had sexual intercourse had increased from 31% to 56% and 26% to 46% respectively with corresponding p < 0.005 and 0.001. The median age at first sex had also increased from below 15 years to 17.4 years for males and 16.6 years for females. Similarly, a delay of median age at first sex was noted for males aged 13 - 19 years old from 17.5 to 18.2 years (p = 0.002) between 1992/93 and 1996/97 in a longitudinal study of Masaka district, Uganda (Kamali et al. 2000). The same studies by Asiimwe-Okiror et. al. (1997) and Kamali et al. (2000) observed delayed marriage among the respondents. Kamali et. al. (2000) reported that women aged 13 - 19 years in Masaka district experienced a significant decrease of annual age specific prevalence of being married, especially at ages 16 - 19 years with p < 0.001. The median age at first marriage rose from 18.5 to 19.5 years between 1992/93 and 1996/97. In the study by Asiimwe-Okiror et al. (1997), huge proportions of 84% of males and 62% of females aged 15 - 19 years in 1995 had never married compared to 75% and 46% in 1989. In addition, findings of focus group discussions in 6 districts of Uganda by Mukiza-Gapere and Ntozi (1995) indicated that women were reluctant to enter into marital unions for fear of HIV infection. In Zimbabwe, Gregson et. al. (1998) found that among 1237 women of childbearing age in Mutasa and Chimanimani districts of Manicaland, personal risk perception was associated with non-marriage. Young women who felt at risk because many of their friends and relatives were dying of AIDS were less likely to enter long-term or cohabiting union. Psychological problems have been found to cause marital instability, separation or divorce due to women refusing sexual advances from spouses for fear of infection by men with several women partners (Dhoundiyal and Shah 1996). In a study in Nigeria, Orubuloye et al. (1992) found that Yoruba women were breaking off marriages, refusing their husband sex or having sex only by using a condom when the husband was HIV infected. In both Kenya and Uganda, it was found that the levels of AIDS widowhood are high. According to Ntozi (1997) the proportions of women who were widows in six districts of Uganda in 1992/93 were high among the prime reproductive age groups, namely 7.5% in 20-24 years, 10.6% in 25-29 years, 14.7% in 30-34 years, 17.7% in 35-39 years. Some of these proportions were as high as 27.7% for 35-39 year-olds in Kabale. Studies among the Luos of Western Kenya also indicated high levels of widowhood (Okeyo and Allen 1994). With HIV/AIDS epidemics, these widows cannot find new sexual partners, so that they can continue producing children. This is because the traditional practice of widow inheritance where a male relative of the late husband used to marry the widow has been discouraged for fear of spreading HIV infection. The widow remarriage rates have fallen. The six-district study in Uganda observed high proportions of widows not remarried in their prime reproductive ages, rising from 59% among the 20-24 year-olds to about 70% among the 25-29 and 30-34 year old (Ntozi 1997). Contraception There is evidence that HIV/AIDS has increased the use of contraception. Glynn et. al. (2000) found that HIV infected women who had given one birth were more likely to have used contraceptives than HIV negative women. The proportion of HIV positive women using modern contraceptives was 34.5% compared to 17.5% among HIV negative women in Yaounde, Cameroon and 20.3% compared to 14.8% respectively in Ndola, Zambia in 1998. Also Ryder et al. (1991) comparing 238 HIV positive and 315 sero negative women in Kinshasa, Democratic Republic of Congo found that 26.4% of the HIV infected were using modern contraceptives significantly higher than 16.3% of the uninfected (p < 0.05). The proportion using a modern method increased with the progression to AIDS stage (42%). This increased contraceptive use was for HIV infected women to meet their objective of reducing their family sizes. For instance in Zambia, two studies observed that respondents favoured reduced family sizes of couples living with HIV/AIDS. Results of 8 focus groups and 23 in-depth studies in Ndola indicated that both women and men were overwhelmingly opposed to continued childbearing by persons with symptoms of AIDS in order to prevent HIV transmission to spouses and children (Rutenberg et. al. 2000). These sentiments were found elsewhere in Zambia among the 65 respondents in in-depth interview in periurban and rural households by Baylies (2000). The threat of contracting HIV had led to some of these respondents decide to produce fewer children than hitherto desired, because of worries of leaving orphans behind for others to look after, the costs to be incurred in caring for them and the hope that fewer orphans would be better cared for. One of the family planning methods that have been resisted in Africa for cultural and other reasons is the condom. With HIV/AIDS epidemic, the resistance is slowly giving way. Recent Demographic and Health Surveys in various African countries have noted increases in condom use for protection against HIV and other STDs. In Manicaland study in Zimbabwe 21% of women reported ever use of condoms for HIV prevention (Gregson). In addition, Lutalo et al. (2000) observed that 26% of 5185 women in Rakai, Uganda in 1995 had ever used condoms, 86% of whom did it for HIV/STDs prevention. Between 1995 and 1998 the condom use in the area increased significantly. For both sexes condom use was greater among respondents who perceived themselves to be at risk of HIV than others. Current condom use was higher among women who had received their results and been counseled than others. HIV positive and counseled women used condoms (12%) more significantly than HIV negative and counseled (8%). Similar results were obtained in Kinshasa, where uptake of condoms was much higher among HIV infected (17%) than among HIV uninfected (3.2%) and the percentage increased to 33.6 for those with AIDS symptoms (Ryder et al. 1991). In West Africa, a study of 450 sexually active women aged 15 - 49 years and men aged 15 - 64 years in Nigeria found that the fear of being HIV infected was a factor that made individuals rely on condoms (Okeibunor 1999). However, some data has indicated that the popularity of condoms as HIV preventive measure has made some women switch from effective methods of family planning to condom use, which is less efficient. Gregson et. al. (1997) reported that 5% (38) of 752 women in the Manicaland study had changed from other contraceptives to using condoms since hearing of AIDS. The majority (63%) of these women had been using the pill, which is considered more efficient than the condom. This switch of methods may result in more pregnancies and hence increase fertility. Pregnancy Rate Other things remaining the same, the level of fertility is directly dependant on the pregnancy rate. Studies in Cote D'Ivoire and Uganda have indicated that HIV infected women have fewer pregnancies than HIV negative women. Table 2 shows results of a study of 4813 sexually active women in reproductive ages in Rakai district of Uganda by Gray et al. (1998). The table displays that in all age groups the pregnancy rate of HIV positive women was lower than of HIV uninfected women with overall rate of 13.4% and 21.4% respectively. A risk ratio of pregnancy between the HIV negative and HIV positive women ranges from as low as 0.48 in age group 20 - 24 years to 0.81 among the 25 - 29 year-olds with an average of 0.63. Regardless of other factors, such as demographic and social variables, pregnancy rate was consistently lower in HIV infected than in HIV uninfected women. Similarly, when the Cox model was fitted to data from the Abidjan study, the hazard ratio was 0.83 implying that being HIV infected decreased the risk of being pregnant by 17% (Desgrees du Lou et al. 1999).
Furthermore, Gray et al. (1998) found that the pregnancy rate was significantly higher among the symptom free seropositive women (14.3%) than among those with AIDS symptoms (7.5%) with p = 0.05. A logistic regression analysis estimated that the risk of pregnancy was greatly reduced in symptomatic HIV infected women (odds ratio = 0.23) compared to the symptom free HIV positive women (odds ratio = 0.49), which implies a 77% reduction in pregnancy risk compared to 51% respectively. This is because clinical manifestations of the disease are expected to increase the illness, reduce the frequency of sexual intercourse and result in disruption of menstrual period (anovulation) and amenorrhoea and probably cause abortion. Similar findings can be seen in Table 3 observed among 4396 women in Yopougon district of Abidjan in Cote D'Ivoire in 1995/96 by Desgrees du Lou et al (1998). The mean number of pregnancies reported by HIV positive women was significantly lower than by HIV negative women in the prime reproductive ages of 25 - 34 years (p < 0.05). Also in Masaka district, Uganda a smaller number of pregnancies (only 30%) were noted among HIV positive women than the uninfected women (52%) at the time of enrolment in a longitudinal study (Ross et. al. 1999).
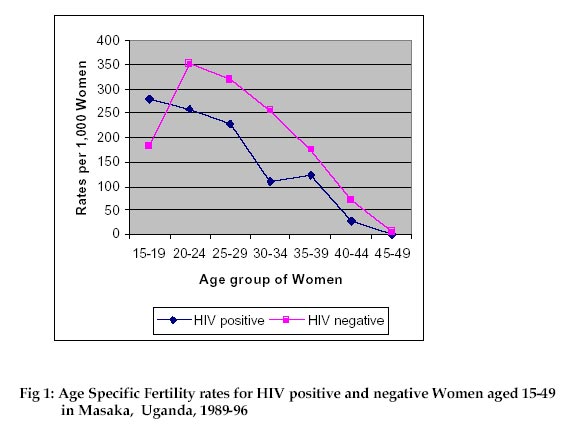
Abortion Abortion is a proximate determinant of fertility, since a pregnancy is not allowed to become a live birth. The Rakai, study in Uganda showed that 18.5% of 130 pregnancies in HIV infected women ended in abortion compared to a lower proportion of 12.2% of 861 pregnancies in HIV negative women. The age adjusted odds ratio of the pregnancy loss in HIV infected versus HIV uninfected women is 1.5, which is high and significant (p = 0.048). This result in East Africa is corroborated by data collected in Abidjan, Cote D'Ivoire in West Africa by Desgrees du Lou etal. (1998), where a multiple logistic regression analysis of risk of having at least one abortion among multiple birth HIV positive versus HIV negative women was 1.15. In a study comparing HIV positive and HIV negative women in Yaounde, Cameroon and Kisumu, Kenya, Glynn et al. (2000) divided abortion into induced or voluntary and spontaneous, which is not controlled by a woman. It was found that 24.1% and 6.2% of HIV infected women in Yaounde and Kisumu respectively attending antenatal clinics and with one live birth had experienced a previous induced abortion, which were higher rates than 16.4% and 4% of HIV uninfected respectively. This could have been done to avoid mother-to-child transmission, reduce the chances of leaving orphans or decrease the AIDS progression rate. Also in Yaounde, Cameroon and Ndola, Zambia, Glynn et al. (2000) observed higher previous spontaneous abortion among HIV infected than HIV uninfected women. The proportion of HIV positive women with one birth who experienced spontaneous abortion was 10.3% in Yaounde and 4.4% in Ndola higher than 7.0% and 1.7% respectively among HIV negative women. Similarly, 10.7% of multiple birth HIV positive women in Yaounde had spontaneous abortion since last pregnancy compared to 7.7% of the HIV negative women. Breast-feeding Breastfeeding is known to delay pregnancy by postponing the return of ovulation. Briefly, the process is that suckling stimulates receptors in the breast nipple resulting into the pituitary gland increasing the production of hormone prolactin. Prolactin inhibits ovulation by reducing hormones needed for ovulation or affecting ovaries. In Sub-Saharan Africa, most women breastfeed intensively and frequently for a long time (at least 12 months) and have been encouraged by government and non-government organizations to continue doing so. Hence, breastfeeding has been used consciously or subconsciously to space children and reduce fertility. It is now established that babies can be infected by their HIV positive mothers through breast milk. Gregson et.al. (1997) found that in Manicaland, Zimbabwe a high two-thirds (67%) of the women in the study knew breastfeeding as a mode of HIV infection. He also observed that women who were aware of the mother-to-child transmission of HIV as a problem associated with breastfeeding were more likely not to have breastfed recent infants. This action may shorten the duration of infecundability amenorrhea leading to a pregnancy sooner and then higher fertility. Postpartum Abstinence In many parts of Sub-Saharan Africa breastfeeding means sexual abstinence of women. This action ensures that the woman is not pregnant until after the breastfeeding duration, which can be as long as over two years in some West African countries. In a study in Southern Benin in 1989, Donadje and Tabutin (1994) reported that over half (53%) of men interviewed favoured extra-marital relations during postpartum abstinence period of wives. Cleland et al. (1999) investigated the relationship between duration of postpartum abstinence and extra-marital sex among a sample of 5941 women and 1533 men in Benin in 1996. A logistic regression fitted to the data showed that sex abstinence of women for 1 - 5 and at least 6 months attracted 1.6 and 1.63 times extra-marital sex compared to no abstinence at all. During focus group discussions in Zimbabwe men cited postpartum abstinence by their wives as a reason for extra-marital relationships (Gregson et. al. 1997). In the era of HIV/AIDS epidemic, this is dangerous to both women and men as it can attract HIV infection to the family. It is possible that women have started to reduce the duration of this abstinence, so as to decrease the risks of HIV infection from other women. This women's action has been facilitated by higher infant mortality due to HIV/AIDS, abruptly stopping breastfeeding and postpartum abstinence and resuming sex with a spouse. Such mechanism would increase fertility in many African societies where low modern contraception is being practiced. However, a three-African-city study of Yaounde, Kisumu and Ndola indicated that higher proportions of HIV positive than negative women practiced postpartum abstinence. Glynn et al. (2000) reported that the percentages of women who had abstained from sex for over 12 months after child birth among HIV infected and uninfected were 41.2% versus 21.5% in Yaounde, 8.6% versus 6.8% in Kisumu and 6.3% versus 3.8% in Ndola. Correspondingly, higher proportions of HIV positive than negative women with several births reported at birth intervals of at least 48 months in Yaounde (48.1% versus 34.6%), Kisumu (35.6% versus 27.4%) and Ndola (32.4% versus 20.6%). This implies that lower proportions of HIV infected than HIV uninfected women were exposed to pregnancy and hence with higher probability of lower fertility. Pathological Sterility The association between sexually transmitted diseases especially gonorrhea and chlamydia and primary and secondary sterility caused by pelvic inflammatory disease leading to subfecundity in several countries in Central and East Africa has been documented elsewhere (Larsen 1989 and Arya et al. 1973). STDs, such as gonorrhea, have been found associated with genital ulceration and to be cofactors in sexual transmission of HIV (Latif et al. 1989). Since HIV is also an STD, it could lead to sub-fecundity directly or indirectly. In an investigation of 1233 pregnant women attending antenatal clinic of Central Hospital of Kigali (CHK), Rwanda in 1992/93, Leroy et al. (1998) observed that HIV positive women had significantly more STDs than HIV negative women. When compared with HIV non-infected women, the infected women were more likely to have history of subfertility in Rakai, although no interaction on pregnancy was observed between HIV infection and the presence of other STDs (Gray et al. 1998). Also menstrual disorders, common in HIV infected women may reduce fecundity, as reported by a study of sentinel sites in Uganda where 26% of HIV positive female patients had amenorrhea compared with only 2% in HIV negative female patients (Widy-Wirski et al. 1988). Because of STDs being cofactors of HIV infection, massive interventions to eliminate STDs have been implemented in areas severely affected by the epidemic, such as Rakai, Uganda. These interventions have the happy result of reducing infertility in women and hence increase their pregnancy risks and fertility, in absence of modern contraception. Natural Fecundity HIV/AIDS in Africa has increased foetal and adult mortality, reduced frequency of intercourse and decreased production of spermatozoa in men. Slightly higher proportion of HIV infected (2.7%) than uninfected women (2.2%) was noted to have had stillbirths in a study in Kigali, Rwanda (Leroy et al. 1998). Glynn et al. (2000) also observed a significantly higher percentage of HIV positive (13.3%) than HIV negative women (7.9%) having a history of stillbirths in Abidjan. Findings from Kagera region, Tanzania claimed that deaths of female household members and close relatives were associated with lower fertility in the households. It was estimated that an increase in adult mortality rate of 5 per 1,000 would reduce the percentage of women giving birth from 10.4% to 6.2% (Ainsworth et al. 1996). Sexual activity of women is affected by HIV/AIDS sickness for an extended period. This reduces the frequency of intercourse, an important proximate determinant of fertility. A study in Rakai by Gray et al (1998) found lower coital frequencies amongst HIV positive women. Also Krieger et al. (1991) and Martin et al. (1991) claimed that HIV infection in men reduces production of spermatozoa, which would affect sexual activity outcome. Macro-Level Effects of HIV/AIDS on Fertility The above presentation was about the biological and behavioural effects of HIV/AIDS on proximate determinants of fertility of individual women. In order to clearly appreciate the impact of HIV/AIDS, it is important to look at macro-level fertility levels and trends. Unfortunately, there are few studies in Sub-Saharan Africa that have data linking the epidemic and fertility of populations at macro-level. Perhaps, the best study published on this relationship on Africa is by Carpenter et al. (1997) on Masaka district, Uganda with HIV prevalence of 11.8%. This is a longitudinal study, which started in 1989 and followed a cohort of over 3500 women aged 15-49 years examined in relation to HIV infection and asked questions on births annually for 6 years. Table 4 and Figure 1 show the age specific fertility rates of HIV positive and negative women and the ratios between the two sets of rates. It can be seen from the table and graph that fertility rates in all age groups except 15-19 years declined with HIV positive status. The reduction in fertility due to HIV/AIDS is high: 26% in 20-24 year age group, 28% in ages 25-29, 57% in ages 30-34, 31% in ages 35-39, 63% in ages 40-44 and 100% in ages 45-49. It is not surprising that with exception of ages 35-39, the level of decline increases with age of women since the HIV effects are combined with other fertility inhibition problems, such as natural infecundity that afflict older women.
It is interesting to note that the resultant general fertility rates of HIV positive women was 194.8 per 1,000 woman-years much lower than 212.3 per 1,000 woman-years for HIV negative women. The ratio between the two rates is 0.74, which is highly significant at p<0.001. The annual ratios of the general fertility of the two groups of women are all below 1.0, namely 0.72 in 1989/90, 0.81 in 1990/91, 0.60 in 1991/92, 0.93 in 1992/93, 0.74 in 1993/94, 0.69 in 1994/95 and 0.69 in 1995/96. This implies that fertility of HIV positive women was consistently lower (by between 7% and 40%) than that of HIV negative women every year for 6 years. The overall ratio (0.74) did not change much when adjusted for marital status (0.75). It is also remarkable to note that total fertility rate in the study population (both HIV infected and uninfected) declined sharply in the six year period from 7.0 in 1989/90 to 6.1 in 1995/96, but most sharply in years of highest prevalence - to 5.3 in 1991/92 and 5.5 in 1992/93 before recovering to 6.2 in 1993/94 when the prevalence started to decline. Carpenter et al. (1997) further presented results of a logistic regression analysis of the relationship between HIV prevalence and giving births shown in Table 5. The table shows that for all reproductive age groups, the proportions of women infected with HIV were much lower for those who gave birth than those who did not give births. The odds ratios ranged from 0.30 to 0.54 and are significant for ages 20-34. The exception was the age group 13-19 years where the odds ratio was 1.43. This is the age group when women are first HIV infected and the disease has perhaps not progressed enough to lower fertility. The overall prevalence for those who gave birth was 9.5% significantly lower than 12.3% for those who did not give birth (odds ratio = 0.56 and p < 0.001).
Another study showing levels and trends of fertility in the population was based on cross-sectional data in 9 districts of Uganda (Ntozi and Ahimbisibwe 2001). Six of the districts outside northern Uganda were surveyed in 1992 and 1995 and the other three all in northern Uganda were studied in 1997. Similar questionnaires were used in the three surveys to collect fertility information from women of reproductive age groups, using a verbal autopsy method to probe for persons living with HIV/AIDS or died of the disease in 1797 households in 1992, 2352 in 1995 and 1206 in 1997. Table 6 displaying results of the study compares fertility rates of households affected by HIV/AIDS (where a member died or was sick of HIV/AIDS) and households not affected by HIV/AIDS (no member of the household had been infected by HIV). The table shows that between 1992 and 1995 fertility declined in the six study districts. The total fertility rate in AIDS affected households dropped from a high 6.8 in 1992 to 5.3 in 1995. Similar decline was experienced in the non-AIDS households from 8.0 in 1992 to 6.3 in 1995. A comparison of the two types of households shows that AIDS affected households had lower fertility rates than the non-AIDS households in both surveys (6.8 compared to 8.0 in 1992 and 5.3 compared to 6.3 in 1995). This pattern is also true of the three northern Ugandan districts, which reported a total fertility of 5.6 in AIDS affected households versus 7.2 in non-AIDS households in 1997. These results imply that women in households traumatized by HIV/AIDS sickness and deaths experience fertility decline, perhaps due to behavioural and biological reasons explained above. It should however be pointed out that these findings should be interpreted cautiously since they do not necessarily refer to the same women in the two surveys.
Across Sub-Saharan Africa, 6 studies in Tanzania, Uganda and Zambia support the claim that fertility has been decreased by HIV/AIDS epidemic. Table 7 shows that without exception HIV infected women experienced major decline of fertility in all 6 studies. The last 2 columns of the table show a tendency of sharper fertility decline with higher HIV prevalence, except the case of Lusaka.
Implications of HIV/AIDS for Fertility Transition in Sub-Saharan Africa As indicated above some countries in the region have started experiencing fertility decline for reasons other than HIV/AIDS. The contribution of HIV/AIDS to the fertility transition is not currently evident for four reasons. First, isolating the factor of HIV/AIDS from other factors of fertility is a complex process because it is not a proximate variable, but one of the contributors to several proximate determinants of fertility. For instance, it is difficult to attribute fertility decline in Botswana, Kenya, South Africa, Swaziland and Zimbabwe to HIV/AIDS, when the fertility transition in these countries started before the effects of the epidemic were felt. Efforts at developing methods to measure the impact of HIV/AIDS on fertility have started (for example see Zaba and Gregson 1998). When refined the methods will be useful to tease out HIV/AIDS contribution to fertility change. Secondly, for the impact of the epidemic to be felt, the prevalence has to be high in the region of 20% and above and be sustained for a long time, about a decade or longer. So far, a few countries have experienced over 20% and none for a decade or so. So the impact can be felt in local areas but not by countries as a whole. An example is Uganda whose prevalence in some areas was as high as 30% in early 1990s, but not sustained for a long time. The country as a whole has not showed a fertility decline between 1991 (TFR = 7.1), 1995 (TFR=6.9) and 2000/01 (TFR = 6.9), but women and households and perhaps districts directly affected by the epidemic have experienced fertility reduction. Thirdly, behaviour factors may reduce fertility of women with symptoms of AIDS, but not those asymptomatic. This is because most African countries severely affected by HIV/AIDS do not have enough HIV testing equipment in place to test and advise most women of their sero status. Even those places with HIV testing equipment, the population is not willing to take the test until their conditions have advanced to AIDS stage. Fourthly, as infant mortality increases, the need to replace dead children and produce more to ensure survival of some will challenge implementation of family planning programmes in Sub-Saharan Africa and perhaps increase fertility. Also, increasing HIV prevalence in the region will mean that HIV/AIDS programmes will compete for resources with family planning programmes, which would weaken the latter. However, the rapid spread of HIV/AIDS and high prevalence in Southern African countries would most likely affect fertility if the current levels persist for at least a decade. Sexual behavioural changes brought about by the epidemic will be critical in postponing the mean ages at first sex and first marriage, reduction in remarriage rates of widows and divorcees and increase of current use of condoms. This could result in fertility decline on national scale. Regardless of the epidemic, demographic transition is already underway in many African countries as mortality and fertility rates started falling in 1980s and 1990s respectively. It is interesting to note that HIV/AIDS has recently resulted into a demographic transition where mortality is increasing as fertility is declining in the African countries severely affected by the HIV/AIDS epidemic. This transition will mean declining population growth rates, which is not in the interests of the population. This is because rising death rates as a means of bringing down population growth rates are not welcome by neither policy makers nor planners. Conclusions The impact of HIV/AIDS on fertility is through biological and behavioural proximate determinants of fertility. To understand the relationship between HIV/AIDS and biological factors of fertility requires expensive medical studies, some of which have fortunately been conducted and pointed to fertility reduction in HIV infected women. Also the link between the epidemic and behavioural factors of fertility indicate fertility decline. What is lacking in understanding the impact of the epidemic on fertility is data on macro-level to decipher the relationship on macro level. The scarce data on macro-level used in this paper was from studies not originally intended to investigate this subject, but was analyzed as a proxy to the required data. It is therefore recommended that focused studies on the impact of HIV/AIDS on fertility be conducted in countries severely affected by the epidemic. A population based sero survey where women in selected households would give blood for testing HIV and questions on pregnancy and birth histories are asked will collect the required data. In spite of the expected decreasing population growth rates due to HIV/AIDS epidemic, policies to reduce the prevalence should be vigorously implemented to eventually eliminate the epidemic. Then the conventional measures of reducing fertility, notably family planning programmes can be adopted. References
Copyright 2002 - Union for African Population Studies | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

{kind=link}