 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies, Vol. 17, No. 2, 2002, pp. 37-60 The Influence of the Service Availability Environment on Contraception during the Course of Fertility Transition William MUHWAVA* Code Number: ep02009 AbstractThe research examines the relationship between the availability of contraceptives and their uptake during the different phases of the fertility transition. The central focus of the paper is to test the hypothesis that “supply creates its own demand”, which is the basis of many family planning programmes. The theory being tested contends that service availability contributes to the fertility transition through five stages of -awareness, information, evaluation, adoption and efficiency. We test this theory using Zimbabwe which has a history of a strong family planning programme and where there is evidence that fertility has been declining. Data from the 1988 and 1994 Zimbabwe Demographic and Health Survey (ZDHS) are used. The individual women records are merged with the service availability data to obtain both women variables and contextual (service environment) variables. Service availability factors considered are: availability of community-based distributor, distance/transport to nearest stationary facility, private doctor offering family planning and availability of pharmacy with family planning supplies. Multilevel modelling is used to measure the influence of service availability factors on contraceptive knowledge and use. This method is considered appropriate as we are dealing with clustered data that require the separation of individual and group effects. RésuméDans ce travail, l’auteur examine les rapports entre la disponibilité des contraceptifs et leur prise au cours des différentes étapes de la transition de la fertilité. L’objet fondamental de cet article est de tester l’hypothèse qui veut que « c’est l’offre qui crée la demande » qui constitue le principe de base de nombre de programmes de planification familiale. La théorie que nous cherchons à tester soutient que la disponibilité de service en planification familiale contribue à la transition de la fécondité par cinq étapes qui sont la sensibilisation, l’information, l’évaluation, l’adoption et l’efficacité. Pour tester cette théorie, nous utilisons le cas du Zimbabwe qui est connue pour ses programmes de planification familiale solides et où la preuve est établie que la fécondité baisse. Pour cela, nous utilisons les données de l’EDS de 1988 et 1994. Les données concernant les femmes prises individuellement sont fusionnées avec celles de la disponibilité du service pour avoir des données à la fois pour les variables femmes et celles pour l’environnement. Les facteurs de disponibilité de service pris en compte sont : la disponibilité d’un distributeur communautaire, l’existence de facilité de transport au point le plus proche, la présence de médecins privés faisant des consultations en planification familiale et l’existence d’une pharmacie disposant de médicaments en planification familiale. Le modèle à multi-niveau a été utilisé pour mesurer l’impact des facteurs de disponibilité du service sur la connaissance et l’utilisation des contraceptifs. Cette méthode est celle qui est la plus appropriée puisque nous traitons des données agrégées qui nécessitent que l’on sépare les effets individuels des effets de groupe. IntroductionThe family planning programme in Zimbabwe has been seen as an example of a successful story, which has raised the contraceptive prevalence rate to about 49 % as of 1994. This rate is the second highest recorded in Sub-Saharan Africa after South Africa. Some factors have been hypothesized to influence the high rate of contraceptive uptake in Zimbabwe and these include: high levels of education, relatively low levels of infant and child mortality, and a well-designed and well-managed family planning programme (Guilkey and Jayne, 1997). The family planning programme in Zimbabwe has focused on developing both outreach and stationary facilities, so it can be hypothesized that the widespread availability of services to both urban and rural communities has been an important determinant of increased contraceptive use. The theoretical view that the availability of family planning influences fertility decline has been presented by Cleland and Wilson (1987) in their "iconoclastic view". Their theory attempts to integrate the three conditions for fertility decline identified by Coale (1973) which are: i. Fertility reduction must be within the calculus of conscious choice. ii. Effective techniques of fertility reduction must be known and available iii. Reduced fertility must be perceived to be advantageous. The concept of service availability has been identified as consisting of four aspects: geographical, cognitive, economic and administrative access (Foreit, et al. 1978). Geographical access refers to how the services are distributed within space and this is usually measured in terms of distance or time to facility. Cognitive access refers to the psychological or woman's perception about the availability of services. Economic costs refer to the financial costs of contraceptives and how affordable these services are to the women. Administrative aspects refer to the organizational structure of the family planning programme and the efficiency with which it distributes supplies. The link between service availability and contraceptive use is that availability provides the supportive environment, which helps the women who wish to use contraception realize their goals. In this respect, service availability translates preferences into real action. Studies that have been carried out to ascertain the relationship between service availability and contraceptive use have produced mixed results. Many of these variations can be traced to the different interpretation of the term "availability". Some researchers use "perceived availability" which is measured from the awareness of the existence of outlets providing contraception and perceptions about the accessibility of these services. Some use "actual availability" which is measured by the physical proximity of services, as well as community factors that might influence the use of these services. While these two concepts can be treated as mutually exclusive, Tsui (1982) has demonstrated that perceived and actual availability interact in a positive way to increase contraceptive prevalence in a population. According to Tsui (1982):.
Studies based on the World Fertility Surveys (WFS) have found positive relationships between contraceptive use and perceived availability (Rodriguez 1979; Pebley and Brackett 1992; Tsui et al. 1981, Tsui 1982). However, a study by Jones (1984) using individual woman data from the WFS has found little relationship between perceived travel time to sources and contraceptive use. These findings are also confirmed by a study by Tsui (1985) using community level data from the WFS which concludes that there is a weak relationship between availability and current use of contraception. Also, data from the first round of the DHS show that there are few countries in the developing world which show a strong relationship between service availability and contraceptive use (Wilkinson et al. 1993). However, in the same report, Wilkinson et al. (1993) indicate Zimbabwe as one of the few countries in Sub-Saharan Africa with a favorable service availability environment, and this accounts for the high contraceptive prevalence, which is the second highest in Sub-Saharan Africa. Data SourcesThe data provided in the paper uses the 1988 and 1994 Individual Woman Recode Files and the Service Availability Modules from the two surveys. The data are merged at cluster level, so that women living in one cluster will have the service availability measures. Objectives 1. To show the effect of service availability on different stages of the fertility/contraceptive transition. 2. To establish the relationship between service availability and contraceptive knowledge/uptake. Analytic Framework of Service Availability and Fertility Transition The framework to be used in this analysis is based on the model developed by Tsui (1985) for the WFS. The model proposes that availability of family planning services generate demand for contraception by introducing ideas about methods of fertility regulation, which would otherwise be unknown to couples. The link between availability of family planning services and contraceptive use is twofold. First, the availability of services provide the technology, information and education, which have a role to play in the diffusion of contraceptive innovation to women/couples who seek to regulate their fertility and promote ideational change about reproductive preferences and norms. Second, the availability of services has to address latent demand by lowering the social, psychological and health costs of contraception. Based on these hypothesized relationships, there are three issues to be addressed here. First, an assessment will be made whether the availability of family planning services has initiated or accelerated fertility decline. Second, an analysis will be done on the effect of family planning availability on changes in reproductive behavior and motives. Third, an evaluation will be made on the effectiveness in contraceptive use of the varying distribution schemes or providers available in Zimbabwe. The framework for testing the effect of service availability in influencing the onset or pace of fertility decline is adapted from Tsui (1985). The framework is based on the notion that diffusion process of any innovation passes through five stages: awareness, knowledge, evaluation, trial and adoption. The stages and measurement are presented in Table 8.1. In this analysis, the stages which have been proposed by Tsui (1985) have been modified to reflect a transition from acquiring knowledge to efficient use. Also, the changes to the original model, which are proposed here will significantly improve the explanatory aspects of the framework. Framework for Analyzing the Relationship between Service Availability and Contraceptive Use
The framework by Tsui (1985) is formulated on the basis of the WFS which interviewed ever-married women in most countries, so the sample here has been changed to include all women in the childbearing ages as per the sample design of the 1988 and 1994 ZDHS. Although the framework suggests a unidirectional flow and ignores counterflows at each stage, it is adequate as a framework for analysing the stages in the rising prevalence of modern contraception in a population. Based on the Tsui's (1985) stages on contraception diffusion, Hammerslough (1992) has formulated some hypotheses related to each stage which aim to separate the effects of service availability on initiation and acceleration of a fertility transition. The initial phases of a fertility transition are characterized by the spread of information about the means of fertility regulation and this moves women with latent demand through Stages A and B. The original hypotheses proposed by Hammerslough (1992) have been revised here to reflect changes which have been made to the original stages proposed by Tsui (1985). They hypothesize that the availability of services in the initial phases is associated with increased knowledge and approval of contraceptive methods. The hypotheses which are linked to Stages A and B is:
An important inclusion in the hypotheisis is to test whether exposure to outreach family planning services leads to changes in contraceptive behavior. The main method of outreach programmes in Zimbabwe is the use of community-based distributors (CBDs). The main aim of using these cadres is to increase contraceptive use in areas which are deprived of services and where there is a large amount of unmet need of contraception. There is an implicit assumption in family planning development that the use of CBDs is an innovation that sidesteps the barriers to the women's adoption of contraception, which exist in stationery facility-oriented programmes. The long-term demographic significance of using CBDs has been questioned by Phillips et al. (1995) who note that:
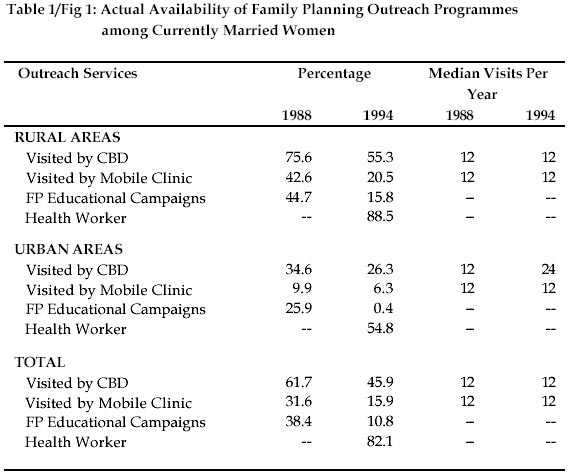
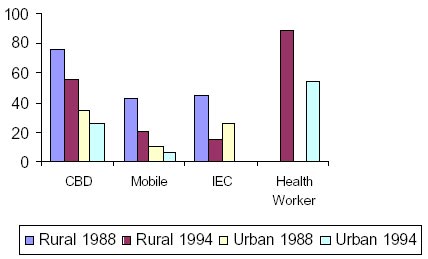
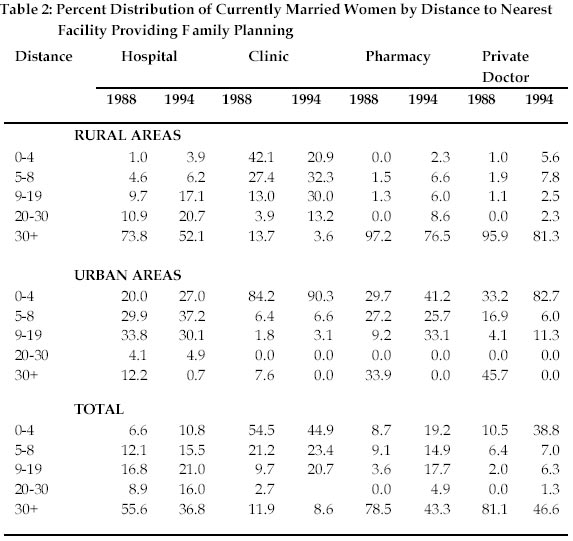
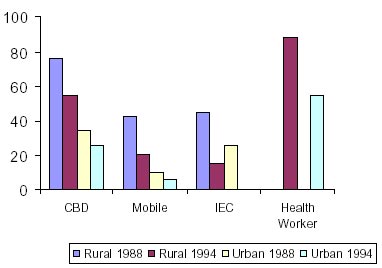
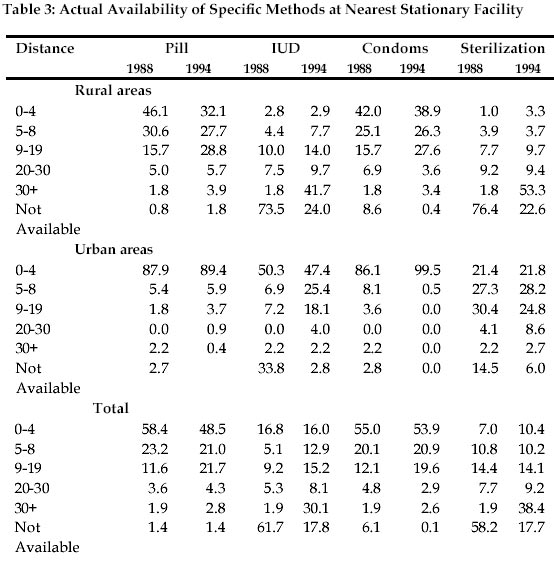
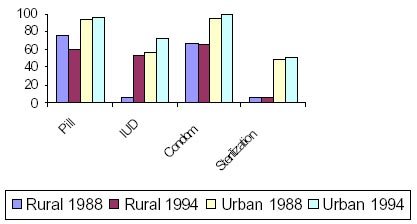
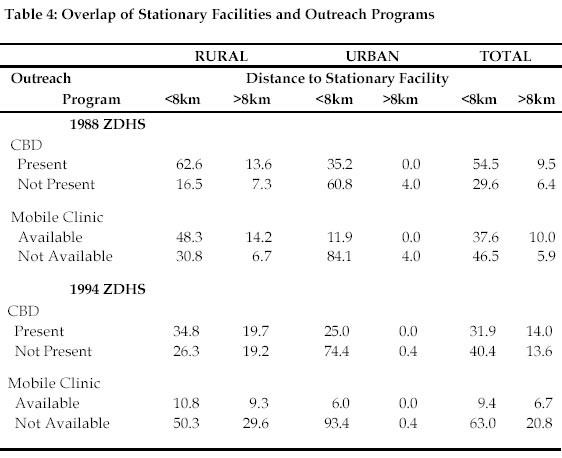
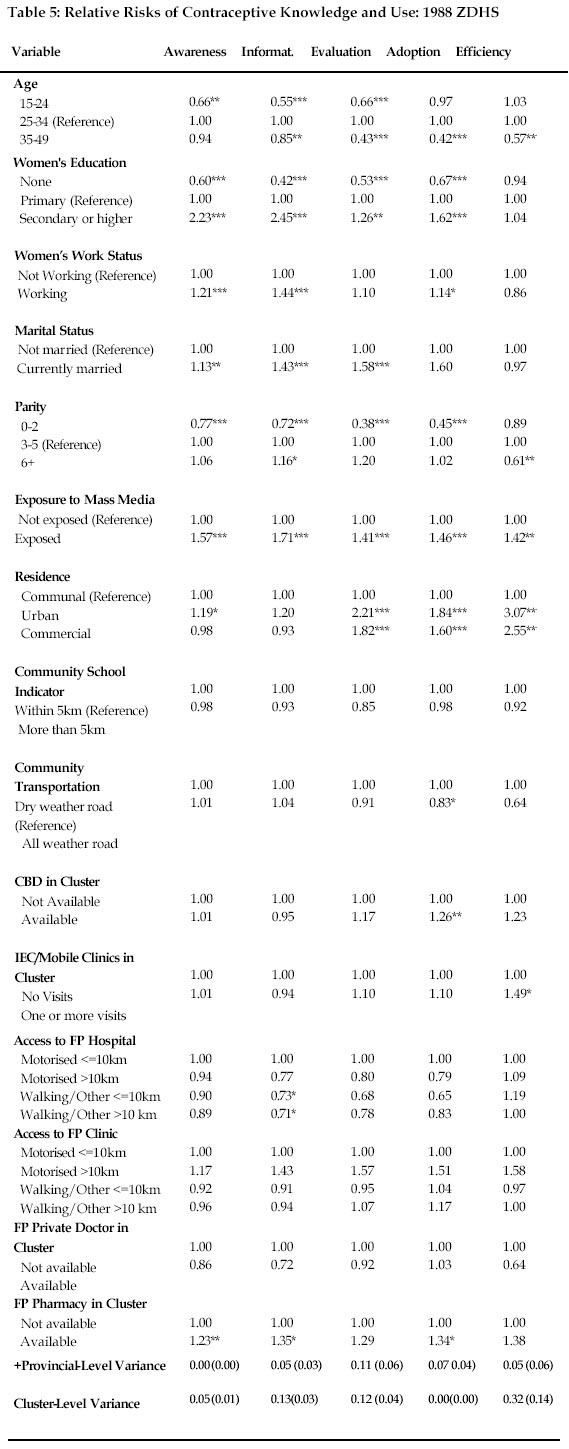
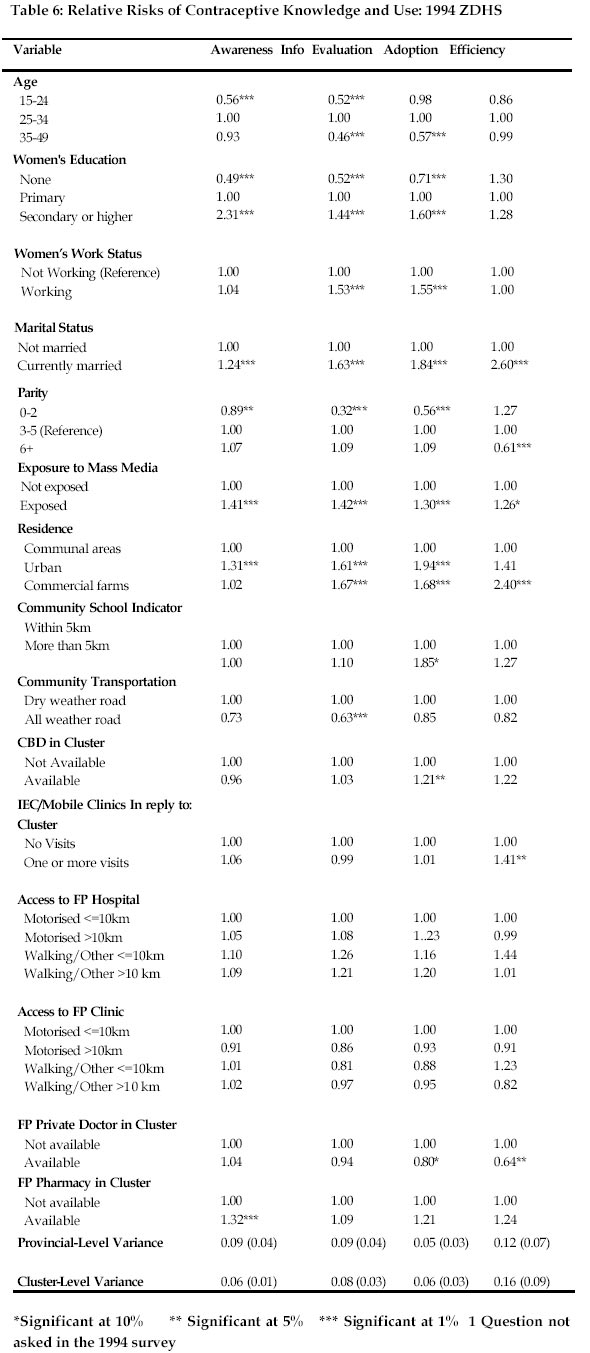
Notwithstanding the above criticism, it has been shown that in Zimbabwe the community-based distribution system has contributed significantly in dispensing supplies and in IEC (Information, Education and Communication) campaigns (Zinanga, 1992; Phiri, 1990; World Bank, 1989). The purpose of the outreach programmes is twofold. In the initial stages of a programme, the use of CBDs is to impact upon reproductive behavior by changing reproductive preferences resulting from ideational changes. Also, CBDs are used in realizing latent demand of contraception by reducing the costs of obtaining contraceptives. In this analysis, it is envisaged that these relationships will be tested. Findings Descriptive Analysis of Actual Service Availability Indicators important for assessing the impact of availability of family planning services include time and distance to facilities, convenience of access, methods available and cost, quality of staff and services, logistical support and follow-up care. Two types of service delivery are examined and these include: (1) outreach programmes which dispense services to the community; and (2) stationary facilities which require clients to come to the facilities. Availability of Outreach ProgrammesThe main task of the outreach programme is to provide a network of services, which distribute family planning services in rural areas where the stationary facilities are limited. The coverage of outreach programmes is provided in Table 1 and Fig 1. The main outreach programme includes the use of Community-Based Distributors (CBD) and Community Health Workers (CWS). The change in coverage by CBDs between the two surveys has resulted from extending the functions of community health workers to carry out development activities including family planning. Around 90 % of rural women are covered by the new cadres and slightly over 50 % in urban areas. Coverage by community workers in urban areas is shrinking since the ZNFPC has decided not to replace those who retire or die, as urban are as are well served by other facilities. Visits by CBDs in rural areas are around once per month although in urban areas visits occur about twice per month. However, it should be noted that these are community visits that do not necessarily reflect number of visits per women. Mobile clinics are the second outreach programme. This is more concentrated in rural areas which are least served by other facilities. Mobile clinics visit the communities a median of once a month. It should also be noted that these mobile clinics are mostly concentrated in three provinces, Midlands, Matebeleland North and South, which have the least facilities. Family planning education campaigns are carried out by the Information, Education and Communication Unit of the ZNFPC. The data show that the educational campaigns were not widely used in 1994 as they were in 1988. However, they still form a substantial part of the outreach programme. Actual Accessibility of Stationary FacilitiesThe main types of stationary facilities providing contraceptives in Zimbabwe include hospitals, clinics, pharmacies and private doctors. The distribution of women by distance to specific family planning stationary facilities is provided in Table 2. The data show there has been an improvement in the accessibility of hospitals, private doctors and pharmacies that offer family planning services between the two survey dates. Provision of family planning services in both urban and rural areas is more limited to clinics. Hospitals that provide family planning still remain inaccessible to women in both urban and rural areas and this has important implications for provision of methods that require specialized equipment and personnel like doctors. Facilities like pharmacies and private doctors are either very far or inaccessible to rural women, and yet these are more accessible to urban women. Availability of Specific Methods at Nearest Stationary Facility Availability of specific contraceptive methods is provided in Table 3. This measure is obtained from an estimate of the distance women would have to travel to obtain a specific contraceptive method. The estimates are based on methods available at the nearest facility. In both rural and urban areas, the pill is the most widely available method of contraception. Condoms are also readily available. Sterilization and IUDs are the least available methods. Availability of all methods is greater in urban areas than rural areas. In general, access to contraceptive methods is good in Zimbabwe, although this is limited to supply methods. Access to clinical methods, IUD and sterilization are rather limited to places where there is easy access to large hospitals, which are mainly manned by doctors who have specialized training in inserting or performing the operations. Low use of clinical methods in Zimbabwe can be explained to the unavailability of these methods to most women, especially those in rural areas. Overlap of Stationary Facilities and Outreach ProgrammesAn examination of the overlap between outreach programmes and stationary facilities is provided in Table 4. The availability of CBD is defined as having a CBD visiting the cluster at least once a month or residing in that cluster. There is a substantial overlap between availability of CBDs and stationary facilities in rural areas. However, the proportion who live in a community easily accessible to stationary facility but without a CBD has increased over the period. There is a small overlap between mobile clinics and stationary facilities. Multivariate Analysis of Service AvailabilityTo assess whether the provision of family planning services increased knowledge about methods of fertility regulation in Zimbabwe, two dependent variables will be used: (i) awareness measured by the number of contraceptive methods known spontaneously; and (ii) information measured by the number of method sources known. The relationship between the dependent and predictor variables can be effectively modelled using the Ordinary Least Squares (OLS) regression, since the two dependent variables are continuous. In modelling these relationships, the hierarchical structure of the data has to be taken into account. The sample designs for the 1988 and 1994 ZDHS are multistage as described in Chapter II, where individual women (Level 1) are nested within clusters/enumeration areas (Level 2) and the clusters nested within provinces (Level 3) hence the models become multilevel represented as :
where the response variable is the number of modern methods or sources of modern methods known by woman i in the jth cluster and kth province. The terms xijk, wjk and zk are vectors of individual, cluster and provincial-level characteristics, respectively and the terms, and are the vectors of estimated parameter coefficients. To access whether the availability of family planning services has accelerated fertility decline in Zimbabwe, three dependent variables will be used: (i) evaluation measured by whether the woman has ever used any clinical method of contraception; (ii) adoption measured by whether the woman is a current user of a clinical method; and (iii) efficiency measured by whether using clinical method versus non-clinical method. The response variables in all cases are binary and logistic regression is the most appropriate modeling technique to use. In addition, because of the hierarchical nature of the ZDHS data, the model becomes a multilevel logistic regression model where women (Level 1) are nested within clusters (Level 2) and within provinces (Level 3). The models are represented by :
where pijk is the probability that a woman i in the jth cluster and kth province has ever used or is currently using a modern or clinical method. The terms xijk, wjk and zk are vectors of individual, cluster and provincial-level characteristics, respectively and the terms b, g and h are the vectors of estimated parameter coefficients. The cluster and provincial-level error terms are represented by µjk (N(0, u2)) and k ( ( N(0, v2)), respectively. In multilevel modeling, there are options for choosing a nonlinear link function for a model with a response variable with a binary outcome. In this analysis the logit function represented by log{(p)/(1-p)} is used. The proportion is assumed to have a binomial distribution represented as yij-Bin(pijk,nijk) with variance: var (yijk/pijk)=pijk(1-pijk)/pijk). In the above, pijk is the expected value of the response in the ijkth level and nijk is the denominator of the proportions. To improve the estimates obtained from the equations, which is the prediction of pijk, the recommendation by Goldstein and Rasbash (1996) is followed of using the Taylor expansion about the current estimated residuals, or posterior means, that is conditioning on these for each level 2 and higher unit and is referred to as penalized or predictive quasilikelihood (PQL). The independent variables which measure aspects of the availability of components of the family planning programme, that is availability of outreach and proximity to stationary facilities are included in the models. The models are fitted controlling for the association of the dependent variables with place of residence, woman's age, woman's education, marital status and community characteristics. These two variables are not much of interest to the discussion, but are included because of their known strong relationships with the knowledge and use measures. All variables included in the model have been recoded into either binary or categorical variables. The results of the regressions are presented in Tables 5 and 6. The coefficients for the first two columns, awareness and information, represent the initial phase of the fertility transition, where knowledge of modern contraception and sources of these methods are hypothesized to be a function of service availability. It is unfortunate that the second knowledge measure was not collected in the second ZDHS, which tends to limit any inferences or comparisons one might want to make about changes over time. None of the variables of service availability outreach show any significant impact on measures of initiation of fertility decline. Also, the impact of proximity to stationary facilities shows little association with any of the knowledge measures, except the availability of a pharmacy which stocks contraceptive. The acceleration stage is dominated by the influence of outreach programmes. In the 1988 ZDHS, IEC and CBD visits show significant impacts, where women who live in clusters without CBDs are less likely to be current users. For current use of modern methods, the influence of CBD remains significant for both surveys. Proximity to stationary facilities is only significant in the adoption phase, but the results of the two surveys are contradictory. A surprising finding is on the last regression for both surveys, where family planning clinics and hospital facilities do not show any influence on adoption of clinical methods among current users indicating that service availability does not seem to bea barrier to use of clinical methods. It would be expected that women who live far away from services would show differential use patterns on the negative side showing existence of latent demand. However, since there are no differential use patterns of clinical methods among current users by availability of outreach or proximity to stationary facilities, then it can be concluded that women using contraceptives are doing so using efficient methods. But it should be noted that this pattern is consistent with the stalling of decline if more women do not adopt clinical methods. What emerges from the last regression is a pattern where one clinical method is dominant, such that differential use patterns by service factors become insignificant. Data from the ZDHS reports show that in Zimbabwe, the pill is the dominant method used by over 75 % of current users. So, in a programme which is pill-based, service factors could be insignificant among those who have already initiated use, since resupply of oral contraceptives seems less likely to be affected by distance, time and mode of transport because at most visitation is only needed once a month. The programme in Zimbabwe recommends that pill-users are supposed to return to clinics or health facilities for routine check-ups once or twice a year. The analysis has shown that the availability of outreach programmes, especially availability of CBDs has significantly contributed towards initiating and accelerating decline and the contribution of state-run stationary facilities in the 1980s is worth noting. However, the programme has been transforming from heavy emphasis on outreach to reliance on service provision at facility level. Such a shift would only be beneficial if stationary facilities can keep the coverage which had been done by the outreach programme and probably expand to recruit more clients using clinical methods. To gain a full understanding of use patterns, the next stage of the analysis would be to examine how service availability influences choice of providers. Source of Supply and Provider ChoiceThe role of family planning programmes can be viewed from two perspectives. First, from the individual woman's point of view, family planning programmes are a means of realizing her reproductive goals. Second, from a macro-level perspective, family planning programmes are a means of fertility reduction, thereby reducing population growth. To achieve these outputs, the family planning programme must be functioning efficiently and the women should be using the methods of fertility reduction effectively. However, in reality, these outputs are not realized because of programme-specific and user-specific characteristics. In this analysis, interest is more on determining the aspects of the family planning programme which determine differential use in contraception. The family planning programme in Zimbabwe consists of a range of stationary and outreach programmes which are both privately and publicly funded and the way in which these different outlets dispense their services differ and thereby their impact on reproductive outcomes differ. In this respect, it will be inevitable to examine how these different distribution outlets differ in meeting the reproductive goals of women. If the performance of the distribution outlets differ, it would be pertinent to explore whether these differences are attributable to the different performance of the outlets or to the varying characteristics of the women who use these outlets. As the contraceptive prevalence increases in Zimbabwe, it would be useful to examine factors which will contribute to the better management of resources and increase efficiency of the programme to cope with increasing demand. With increasing demand, it is envisaged that the private sector and Non-Governmental Organizations will become more and more involved in family planning service provision. This results in a diverse group of service providers, which have different delivery systems, different efficiency levels and costs, thus each type of provider will attract different clients with different characteristics. An examination of the selection process by method-source type is an important input is seeking ways to expand family planning services, as the process of selection reflects both client and provider characteristics and perceptions. According to Khalifa (1995):
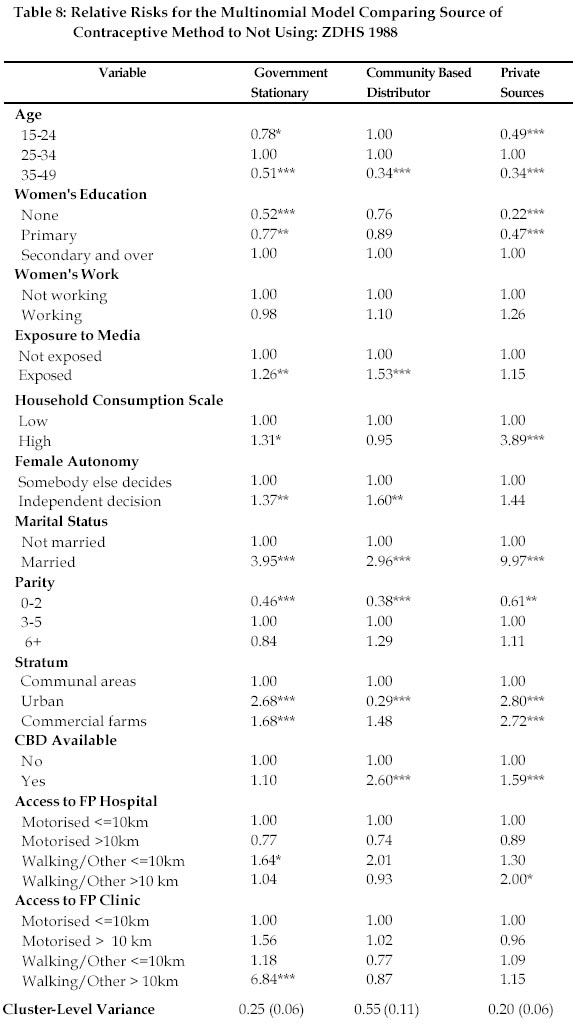
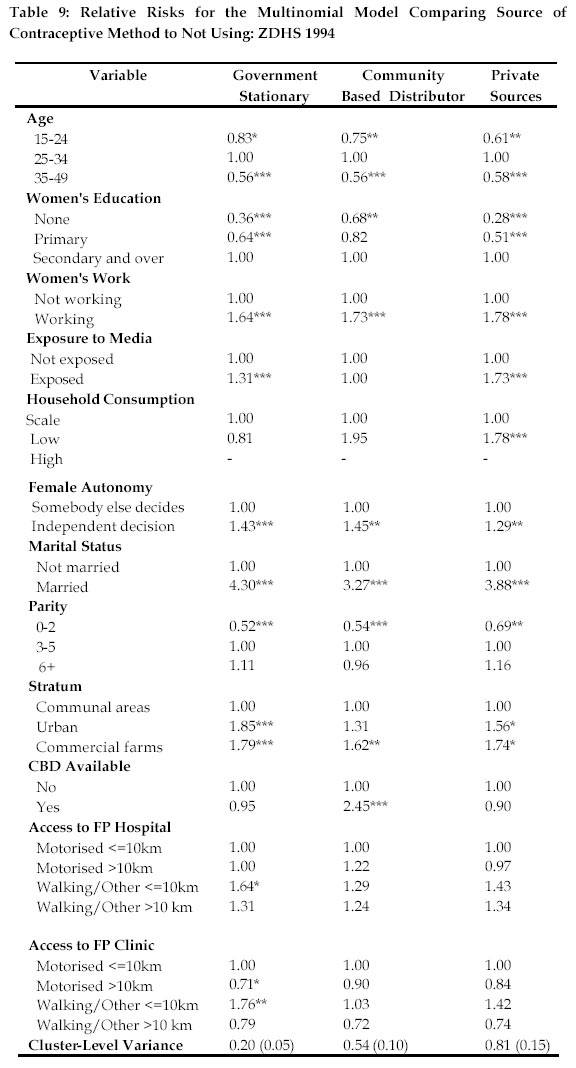
It is envisaged that by examining all these different aspects of the family planning programme, the experience from all these diverse distribution sources can be integrated to produce a programme which can effectively reduce discontinuation, failure and unmet need. In the Zimbabwean case, the sources of contraceptives can be grouped into outreach and stationary facilities, and by the means which they are financed, which are public or government owned or unsubsidized private owned. A number of hypotheses can be drawn from the above categorization. First, the decision to use either a public versus a private facility can be based on access and cost, which is normally equated with hospital user fees. If cost is a barrier to use, then it would be expected that there is less use of expensive outlets among poorer women. Second, the difference between outreach and stationary facilities would be linked to quality of care. So, use of a specific provider reflects a selection among alternative possibilities or lack of them, each which differs with respect to accessibility, cost and quality. These decisions are determined by both internal and external factors, which reflect individual characteristics, family and community attributes. Table 7 provides a cross-classification of choice of provider by method Most of the users rely on the pill form government stationary facilities followed by pill for CBDs. The role of the private sector in providing any form of contraception is very small in Zimbabwe. Analyses of the multivariate relationship between method-source and service availability factors are presented in Tables 8 and 9. The choice of provider differs markedly for the different variables, especially the characteristics of the women. Women aged 35-49 are less likely to use government stationary facilities when compared to women aged 25-34 and the results are significant at 1%. There are no statistical significant differences in the choice of CBDs between women aged 15-25 and those 25-34 in the 1988 surveys, but in the second surveys the differences are significant. Women aged less than 25 years are less likely to use pionders from private facilities. Women aged over 35 years are less likely to use any of the providers. The differences by education reveal that the less educated women are less likely to use stationary facilities from private and public sector providers. An important observation is that the choice of CBDs is actually higher for educated women (secondary and higher), which is contrary to the aim of the CBD programme which aims to provide access to those who are less privileged. This pattern has not changed between 1988 and 1994. Another important observation is high usage of both the public and private sector by women with secondary and higher education, which indicates that these women are using both sectors. The pattern of provider choice is less clear by the work status of the women between the two surveys. In the 1988 survey, there are no significant statistical differences. However, in the 1994 survey, working women are more likely to be using government stationary facilities, CBDs and private sector providers. Other indicators of social class indicate that women in high socio-economic status are more likely to be using modern contraception from both the public and private sector providers. Married women are more likely to be using both the private and public sector facilities when compared to unmarried women. Low-order parity women are less likely to be using any provider. However, although the results for high-order parity women (6+) are not significant, these women are more likely to be using methods from all providers. Use of government stationary facilities is higher in urban areas, when compared to communal areas. Also, women in commercial farming areas are highly likely to be using government stationary facilities. In the 1988 survey, use of CBDs is higher in urban areas. The differences between communal and commercial farming areas in terms of use of CBDs is significant and the odds ratios are higher for commercial farming areas. Use of private sector facilities is higher in urban and commercial areas than communal areas. Women who live in clusters with CBDs are more likely to be using pills supplied by CBDs. This indicates that CBDs are being active in motivating women to take up the pill. In the 1988 survey, women who live in clusters with CBDs are more likely to use methods supplied by the private sector. Discussion This chapter has examined the impact of service availability factors on knowledge and use of contraception, the utilisation of different family planning outlets, and the impact of the quality of care on contraceptive adoption. The models measuring the impact of service availability factors have been fitted controlling for the development level of the clusters by including community education, strata, type of transport network, and availability of other MCH facilities. The aspects of service availability are examined as having an influence on the stages of the contraceptive transition, which follows five stages: awareness, information, evaluation, adoption and efficiency. Although, the framework used here assumes a unidirectional movement through these stages, in reality this might not be the case because of counter-flows and simultaneity of events. For example, if a woman moves from one cluster to another, she would not necessarily start from stage one but would need stage 2 or a woman might acquire awareness, information and efficient use at the same time. Despite this weakness, the framework reflects the necessary conditions for contraceptive adoption. The findings in this paper do not show any influence of the service availability factors on the initiation of fertility decline. A possible explanation is that awareness of an existence of a phenomenon is a one-off event, and the measures of initiation are based on 1988 when there was already widespread knowledge of both methods and sources of supplies. According the 1988 ZDHS, almost 95 % of all women were aware of at least one modern contraceptive method, and the pattern is the same for place of residence, level of education, age of the woman and region. One suspects that if the same analysis could be done for the period immediately after 1981 when a vigorous family planning programme was initiated, then these differences in knowledge would be evident. The acceleration phase of the fertility transition is dominated by the availability of a CBD in the cluster. This gives credence to the fact that investment in the CBD programme has played an important role in the transition. The results of both surveys show that the CBD programme has produced results in the past, and continues to do so almost two decades after its expansion to embrace all population subgroups. The influence of CBDs is important in rural areas, so the continued existence of this outreach programme is justified. Also, the decision by the ZNFPC to phase out CBDs in urban areas seems logical, since their influence in urban areas has been minimal. The activities of CBDs are gradually being phased out in urban areas by natural attrition where the remaining urban CBDs from earliest years of outreach development are not being replaced as they retire or die. However, of concern is the non-expansion of the CBD programme in rural areas where it is needed most. The World Bank (1989) noted that numbers of CBDs have remained stable for some years at around 600. The original target of a network of 1000 CBDs was abandoned a few years ago due to financial constraints. Although there are still large areas throughout the country unserved or under-served by the CBD network, which at present covers only 40 percent of the population of the rural population, there are no plans for further expansion. Availability of stationary facilities does not seem to exert any influence on the stages of transition, but this should not be interpreted as though they are not important. Rather, this points to the need for placing and improving facilities in communities where use is low and strengthening existing facilities. The paper has also examined the determinants of choice of provider. There are important findings from this analysis. First, in clusters where CBDs are available, there is a significant reliance on them as a source of supply. Second, there is high usage of stationary facilities which are within walking distance. To conclude, the choice of a provider varies according to the characteristics of the woman and the proximity or availability of the provider. Use of private providers is associated with women in high social status, probably because these services are paid for and can only be used by those who can afford the fees. The policy implications are that the family planning programme in Zimbabwe still needs the outreach approach, especially in rural areas, so the government should continue supporting this aspect. Stationary facilities are increasingly becoming important in urban areas, so they should expand their capacity to provide family planning services. Private providers are also becoming important providers and social marketing should be expanded with private providers. References
* The article was written as part of a Ph.D Thesis and adapted for a paper while the author was Acting Executive Secretary of the Union For African Population Studies. Copyright 2002 - Union for African Population Studies The following images related to this document are available:Photo images[ep02009t9.jpg] [ep02009t3.jpg] [ep02009f1.jpg] [ep02009f3.jpg] [ep02009t6.jpg] [ep02009t8.jpg] [ep02009t5.jpg] [ep02009t2.jpg] [ep02009f4.jpg] [ep02009t7.jpg] [ep02009t4.jpg] [ep02009f2.jpg] [ep02009t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}