 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
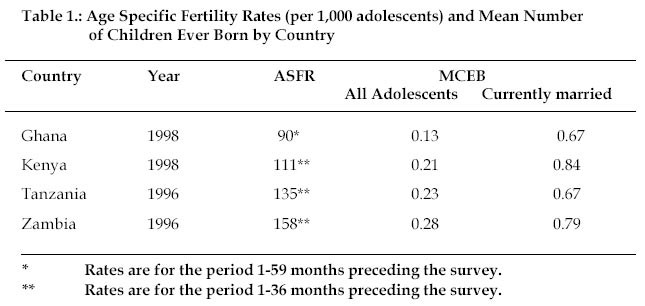
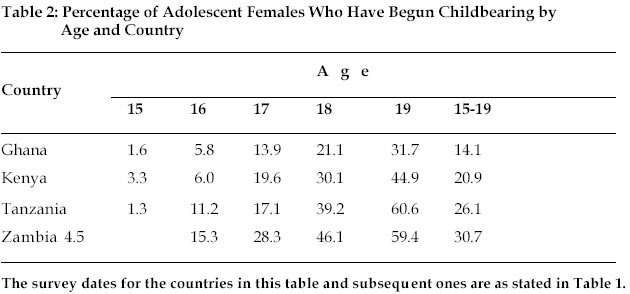
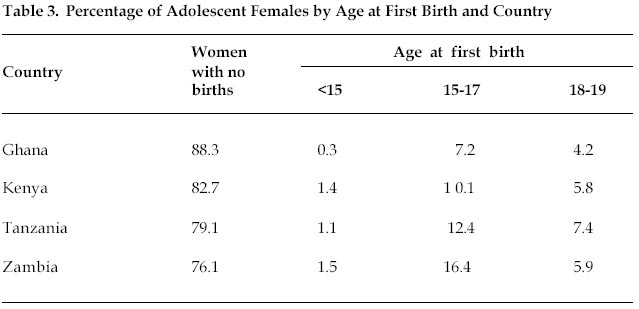
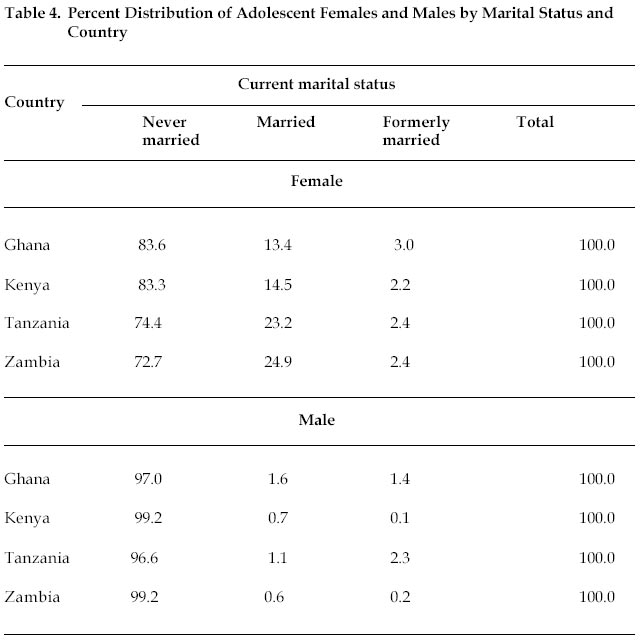
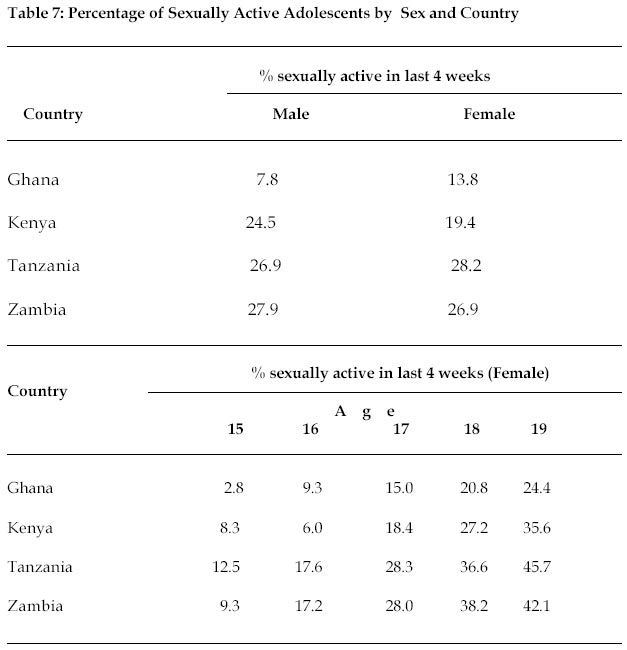
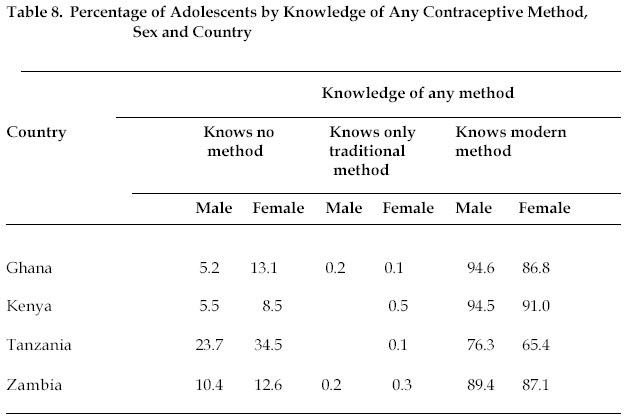
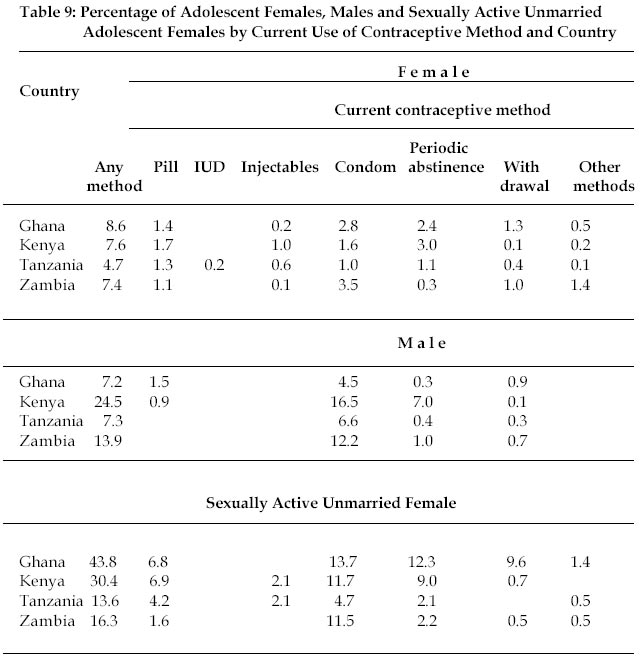
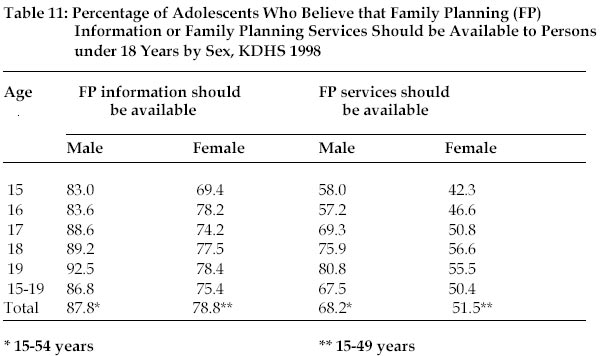
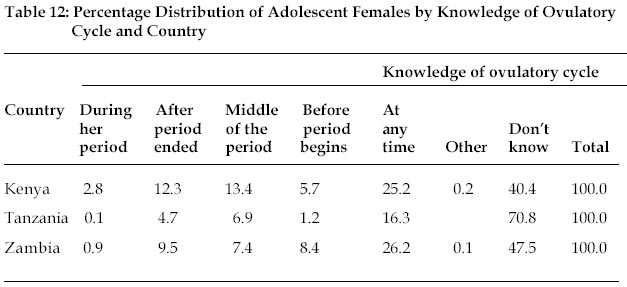
African Population Studies, Vol. 17, No. 2, 2002, pp. 81-98 Adolescent Fertility and Reproductive Health in Four sub-Saharan African Countries E.O. TawiahRegional Institute for Population Studies, Legon, Ghana Code Number: ep02011 Abstract Using Demographic and Health Survey (DHS) data for Ghana (1998), Kenya (1998), Tanzania (1996) and Zambia (1996), the paper has examined adolescent fertility and reproductive health in the four sub-Saharan African countries. Adolescent fertility is highest in Zambia and lowest in Ghana. Age specific fertility rate for adolescent females (15-19 years) ranges from 90‰ Ghanaian female adolescents to 158‰ Zambia adolescent females. Adolescent females’ contribution to total births ranges from 10% in Ghana to 13% in Zambia. At age 19 years, the percentages of adolescent females who have started childbearing were 61 in Tanzania, 59 in Zambia, 45 in Kenya and 32 in Ghana. In Ghana and Tanzania, a larger percentage of adolescent females than males have had sexual intercourse, while the reverse holds for Kenya and Zambia. Contraceptive knowledge is high but its use is low among adolescent males and females. Adolescent females have low levels of knowledge about some aspects of reproductive health. The proportions of adolescent females who correctly mentioned that a woman is most likely to conceive in the middle of the ovulatory cycle were 6.9% in Tanzania, 7.4% in Zambia and 13.4% in Kenya. The knowledge base in reproductive physiology of in and out-of-school adolescents should be strengthened. Sexuality education and other emerging issues such as human rights, harmful practices and violence should be integrated into population education and reproductive health programmes. RésuméEn partant des données de l'Enquête démographique et de santé (EDS) du Ghana (1998), du Kenya (1998), de la Tanzanie (1996) et de la Zambie (1996) cet article examine la question de la fécondité des adolescents et la santé de la reproduction dans les quatre pays de l'Afrique sub-Saharienne. La fécondité des adolescents est plus élevée en Zambie et plus faible au Ghana. Le taux de fécondité des adolescents (de 15 à 19 ans) lié à l'âge va de 90‰ chez les adolescentes ghanaennes à 158‰ avec les adolescents de la Zambie. A l'âge de 19 ans, le pourcentage des adolescents ayant commencé à avoir des enfants était de 61 en Tanzanie, 59 en Zambie, 45 au Kenya et 32 au Ghana. Au Ghana et en Tanzanie, il y a eu plus d'adolescentes que d'adolescents à avoir eu des rapports sexuels alors que c'est l'inverse au Kenya et en Zambie. La connaissance de la contraception est élevée mais son utilisation est faible à la fois chez les adolescents et adolescentes. Les adolescentes ont des niveaux faibles de connaissance de certains aspects de la santé de la reproduction. Le pourcentage des adolescents qui ont dit avec justesse qu'une femme tombe en grossesse plus probablement au milieu de son cycle menstruel était de 6,9 % en Tanzanie, 7,4 % en Zambie et 13,4 % au Kenya. La connaissance des adolescents entrant ou sortant de l'école de la physiologie de la reproduction doit être renforcée. L'éducation à la sexualité ainsi que d'autres phénomènes récents tels que les droits de l'homme, les pratiques nocives et la violence doivent être intégrés dans les programmes d'éducation à la population et de la santé de la reproduction. 1. Introduction Adolescent fertility and reproductive health has become a matter of serious health concern worldwide particularly in view of human immuno-deficiency virus (HIV) and acquired immune deficiency syndrome (AIDS) pandemic as well as levels of teenage pregnancy, illegal abortion and childbearing, health and economic consequences. Various international fora such as the 1994 International Conference on Population and Development (ICPD) held in Cairo, Egypt, the 1997 African Forum on Adolescent Reproductive Health in Addis Ababa, Ethiopia and the 1999 World Youth Forum at the Hague, Netherlands have addressed adolescent and youth sexual and reproductive health issues. A number of studies have also focused on adolescent fertility and reproductive health in the region (Ajayi et al., 1985; Nabila and Fayorsey, 1995; Ngalinda, 2001; Population Impact Project, 2001). Early pregnancy and childbirth of an adolescent mother forecloses educational and employment opportunities. At the national level many public and private institutions and organizations in sub-Saharan Africa have held numerous seminars, workshops and conferences not only to highlight adolescent sexual and reproductive health issues but also more importantly devise programmes and strategies to combat teenage pregnancy. A case in point is the introduction of family life education (FLE) into school curriculum at the primary and secondary levels of education in Ghana. It is envisaged that arming young children with adequate knowledge of reproductive health matters will help pave the way to responsible parenthood and also enable them make responsible decisions that affect their lives. The estimated percentage of the population under 25 years in sub-Saharan Africa in the year 2000 was 64.1 (United Nations, 1998). This suggests that a tremendous number of adolescents and youth are at or are reaching reproductive age and are potential candidates for early motherhood. It is quite obvious that neglecting the reproductive health needs of adolescents and the youth who form a significant proportion of the population of sub-Saharan Africa will have long-term adverse effects on the capabilities of our next generation, in particular the women. Ensuring a better future for adolescents and youth is therefore a goal which must be vigorously pursued (Population Impact Project, 2000). The terms “adolescents” and “teenagers” are used interchangeably in this paper. The concept of adolescence has been variously defined as “the state or process of growing up” or “the period of life from puberty to maturity” depending upon the subject-matter being studied (United Nations, 1989). This underscores the difficulty of identifying a specific period of life as the adolescent period. Then, too, variations in social and cultural settings between countries and biological differences concerning age of physical maturation make different connotations to the meaning of adolescence in different societies. Comparison between countries is therefore made in the context that the age group used to define the adolescent period in this paper (15-19 years) cannot be representative of all countries’ practical definition of adolescence. This paper’s definition of adolescents as persons aged 15-19 years is somewhat limited by the fact that the Demographic and Health Surveys collected information from female respondents aged 15-19 years and male ones aged 15-59 years. It does not tally with World Health Organisation’s definition of adolescents to cover ages 10-19. The purpose of the paper is to provide a comparative study of adolescent fertility and reproductive health in Ghana, Kenya, Tanzania and Zambia. Its main focus is on adolescent females but where data permit a comparative analysis of adolescent females and males has been made. The paper attempts to provide answers to the following questions: (i) What is the extent of sexual exposure of adolescents? (ii) What is the magnitude of adolescent fertility? (iii) What is the level of knowledge and contraceptive use among adolescents? 2. Data Sources The data for this paper are derived from the 1996 Demographic and Health Surveys (DHS) of Tanzania and Zambia and the 1998 Demographic and Health Surveys (DHS) of Ghana and Kenya. Availability of current DHS data is the main criterion used for selection of the four sub-Saharan African countries. The four data sets which are nationally representative samples of men and women collected information on the following topics: respondent’s background characteristics, reproductive history, contraceptive knowledge and use, antenatal, delivery and postnatal care, infant feeding practices, child immunization and health, marriage, fertility preferences and attitudes about family planning, husband’s background characteristics, women’s work, knowledge of HIV/AIDS and sexually transmitted infections (STIs), as well as anthropometric measurements of children and mothers. In addition, each country included some topics of special interest. For example, both Kenya and Tanzania collected information on maternal mortality and female circumcision. It is worth mentioning that the four Demographic Health Surveys did not collect much information on adolescent reproductive health per se. A component of reproductive health which got much treatment is family planning. Apart from Ghana, the three other surveys collected information on knowledge of the fertile period which gives an indication of whether respondents are conversant with some reproductive health matters. 3. Results 3.1 Adolescent Fertility Levels Two indicators of level of adolescent fertility namely; age specific fertility rate (ASFR) for age 15-19 and mean number of children ever born (MCEB) to women aged 15-19 years are used in this analysis. Table 1 provides information on age specific fertility rates and mean number of children ever born for the four selected countries. Although a good body of evidence suggests that fertility is falling in these countries, age specific fertility rates for adolescents are still relatively high by world standards. ASFR varies from 90‰ Ghanaian adolescent females to 158‰ Zambian adolescent females. In other words, fertility in Zambia is 1.8 times higher than it is in Ghana. Kenya occupies an intermediate position. Analysis of adolescent females’ contribution to total births in the five years preceeding the survey was 10% in Ghana. The correspondings percentages for total births in the last three years before the survey were 11.8% in Kenya, 11.6% in Tanzania and 13% in Zambia (figures not shown). With regard to MCEB, it is noted that Zambian adolescent females have the highest fertility, while Ghana is at the rear. Analysis in terms of currently married adolescent females shows that Ghana and Tanzania trail behind Kenya and Zambia. Kenya has supplanted Zambia at the first position. 3.2 Adolescent Motherhood Early pregnancy and childbirth of an adolescent tends to give rise to high school drop-out rates, low self-esteem, low employment opportunities and lower productivity. Table 2 presents percentage of adolescent females who have begun childbearing by age. There are wide variations among countries. In Zambia, 31% of adolescent females have begun childbearing compared to 26% in Tanzania and 14% in Ghana. In Kenya, it is one out of every five adolescent females. Analysis in terms of single years of age shows that Tanzania has the smallest percentage (1.3%) of 15-year-olds who have begun childbearing followed by Ghana (1.6%), Kenya (3.3%) and Zambia (4.5%). At age 19, Tanzania has overtaken Zambia with 61%. It is significant to note that Tanzania registered the largest percentage increase between ages 18 and 19, 22 percentage points. Early motherhood in Tanzania by age 19 seems to have been precipitated by marriage, low educational attainment and other factors. The proportions currently married at age 19 are 30.4% in Ghana, 37.5% in Kenya, 47.4% in Zambia and 48.7% in Tanzania (figures not in table). Addition of a percentage of 6.9 of formerly married to that of the currently married means that one out of every two Tanzanian adolescent females has been exposed to the risk of childbearing, whereas the corresponding percentage for Ghana is 36. Low educational attainment might also have contributed to early motherhood in Tanzania. Whereas only 7.5% of 19 year-old Tanzania adolescent females have attained secondary education, the corresponding percentages are 70 for Ghana, 31 for Kenya and 35 for Zambia (figures not in table). 3.3 Age at First Birth As already noted, early childbearing of an adolescent female has social, health and economic costs which the adolescent is invariably unable to cope with. Pregnancy of a still-growing girl means an increase in nutritional requirements, not only for the growth of the foetus, but also for the mother herself (Friedman, 1985). A good body of evidence also shows that women who have their first birth early in life tend to have more children than those who start childbearing later. Information on adolescent females by age at first birth is presented in Table 3. Whereas 0.3% of Ghanaian adolescent females have their first birth under 15 years, the percentage for Zambia is 1.5. However, among 18-19-year-olds Tanzania emerges as the country with the largest percentage (7.4%) followed by Zambia, Kenya and Ghana in that order. 4. Sexual Exposure 4.1 Entry into Union In most of sub-Saharan Africa, marriage signals the beginning of sexual activity and the onset of a woman’s exposure to the risk of childbearing. Table 4 presents percentage distribution of adolescent females and males by current marital status. As expected, the proportions of married adolescent females are much higher than those for males. This phenomenon may not be unrelated to lower female educational attainment. For instance, the percentage of uneducated adolescent females ranges from 2.9 among Kenyan adolescents to 16.4 among Tanzanian adolescents. The corresponding male percentages range from 1.8 in Kenya to 9.2 in Tanzania (figures not shown in table). The proportion of married adolescent females ranges from 13% in Ghana to 25% in Zambia. It is worthy of note that one out of every four Zambian adolescent females is currently married and this obviously has fertility and reproductive health implications. 4.2 Sexual Exposure Among Adolescents Early sexual exposure has health implications for the adolescent mother and is also a key indicator of adolescent’s potential risk for unplanned pregnancy, abortion and sexually transmitted infections. Table 5 provides information on proportion of adolescents who have had sexual intercourse. Increasing age is associated with increasing sexual activity. For example, in Kenya, the proportion of adolescent females who have had sexual intercourse rises from 16% among the 15 year-olds to 73% among the 19 year-olds. In Ghana and Tanzania, a larger percentage of females than males have had sexual intercourse, whereas the opposite is the case in Kenya and Zambia. Among the four countries, Zambia registered the highest percentages. The percentage of 19 year-old females who have had sexual intercourse ranges from 68 in Ghana to 84 in Zambia. Zambia is notably characterized by early initiation of sexual intercourse. For example, one out of every four 15 year-old Zambian males has had sexual intercourse, while 89% of 19 year-old Zambian males have had sexual intercourse. Sexual initiation among adolescents has also been reported in a study of 14 countries comprising four from sub-Saharan Africa, two from Asia, six from Latin America and Caribbean and two from developed countries (Great Britain and United States) (Singh et al., 2000). 4.3 Sexual Exposure Among Unmarried Adolescents Sexual intercourse among unmarried adolescent females in the absence of effective contraception increases the risk of pregnancy and childbearing with their attendant socio-economic and health consequences. It is seen in Table 6 that a much higher proportion of never married adolescents in the three East African countries have had sexual intercourse than is the case for Ghana. Zambia has the largest proportion of adolescents who have had sexual intercourse. Except in Ghana, unmarried adolescent males have been more exposed to sexual intercourse than their female counterparts. In both Kenya and Zambia, more than one out of every two unmarried adolescent males have had sexual intercourse. 4.4 Frequency of Sexual Intercourse All the four countries collected information on recent sexual activity defined as sexual intercourse in the four weeks preceding the survey. Information on the frequency of sexual intercourse can be used to complement measures of exposure to the risk of pregnancy. Table 7 shows percentage of sexually active adolescents. In Ghana and Tanzania, adolescent females were more sexually active in the four weeks before the survey than their male counterparts, whereas the reverse is the case in Kenya and Zambia. In Tanzania and Zambia, one out of every four adolescent males and females was sexually active in the four weeks preceding the survey. The lower panel of Table 7 provides information on recent sexual activity for adolescent females by age. There is a positive relationship between recent sexual activity and age of adolescent females. For instance, the percentage of Tanzania adolescent females who had sexual intercourse in the four weeks before the survey increases from 12.5 among the 15 year-olds to 45.7 among the 19 year-olds. However, the Kenyan pattern displays a percentage decrease among the 16 year-olds after which it conforms to the general pattern already depicted. 5. Contraceptive Knowledge and Use 5.1 Contraceptive Knowledge Information on adolescent female and male respondents’ knowledge of contraception was collected in two ways. Respondents were first asked to mention “ways or methods” of contraception that they had heard about spontaneously. Interviewers then described methods not mentioned spontaneously to see if respondents recognized the method. Knowledge of a family planning method is defined as having heard of a method. Table 8 shows percentage of adolescents by knowledge of contraception. In general, contraceptive knowledge is very high among adolescents. Knowledge of modern methods of contraception is more predominant than any other method among adolescents. There are sex differentials according to contraceptive knowledge. A larger proportion of adolescent males than females in each country has knowledge of contraception. The percentage who has knowledge of modern methods ranges from 76.3 in Tanzania to 94.6 in Ghana among adolescent males, whereas for females it ranges from 65 in Tanzania to 91 in Kenya. It is also seen that knowledge of modern contraceptive method is highest in Kenya and lowest in Tanzania. 5.2 Contraceptive Practice Adolescent sexuality in most of sub-Saharan Africa has raised a lot of eyebrows in view of low contraceptive use, unplanned pregnancies and sexually transmitted infections including HIV/AIDS. One of the more serious challenges facing family planning programmes particularly in sub-Saharan Africa is to address the reproductive health needs of adolescents as they initiate sexual activity and are exposed to the risk of pregnancy (Blanc and Way, 1998). Table 9 shows percentage of adolescents by current contraceptive use. Except in Ghana, current contraceptive use is much higher among adolescent males than females. For males, it ranges from 7.2% in Ghana to 24.5% in Kenya. In general, use of modern methods is higher than that of traditional methods. Among females, the predominant contraceptive method in Ghana and Zambia is the condom, while in Kenya and Tanzania it is the pill. The most predominant method used by males in all the four countries is condom. With regard to adolescent males, contraceptive use is highest in Kenya followed by Zambia, Tanzania and Ghana in that order. In Kenya, one out of every four adolescent males has used any contraceptive method, the predominant contraceptive method being condom. For females, Kenya ranks second after Ghana. It is seen in Table 9 that 1.5% and 0.9% of adolescent males in Ghana and Kenya respectively reported using the pill which is a female contraceptive method. It is possible that these males are reporting on behalf of their female counterparts. The third panel of Table 9 provides information on current contraceptive use by sexually active unmarried adolescent females. The overall use of a contraceptive method is highest in Ghana and lowest in Tanzania. The percentage of sexually active unmarried adolescent females using a family planning method rises from 14% in Tanzania to peak at 44% in Ghana. Apart from Ghana, current use of a modern method of contraception is higher than use of a traditional method of contraception. The most widely used modern method of contraception is the condom followed by the pill. With the exception of Tanzania, one out of every 10 sexually active unmarried adolescent females used condom. Periodic abstinence is the most predominant among the traditional methods. As expected, contraceptive use among sexually active unmarried adolescent females is higher than it is among married teenagers . Blanc and Way (1998) reported similar findings based on DHS data for the early 1990s for 19 sub-Sahara African countries. In Ghana, 44% of sexually active unmarried adolescent females are currently using a family planning method compared to a contraceptive prevalence rate of 25% for currently married adolescent females. The corresponding percentages are 14% and 9% in Tanzania (figure not in table). 5.3 Main Reason for Using Current Source In order to design family planning programmes to meet the needs of adolescents it is important for family planning programme managers and implementers to differentiate between access-related reasons and service-related reasons. Apart from Zambia, Ghana, Kenya and Tanzania collected information on the main reason for selecting the place where contraceptors get family planning services instead of the other place they know about. In general, the main reason for using current source of supply of family planning services is that female contraceptors do no know about any other source. As shown in Table 10, access–related reasons are more important than service-related and other reasons. The second main reason given by adolescent females and currently married adolescent females is “close to home”. The pattern for the never married sexually active adolescent females is similar except that in Kenya, a service-related reason such as “staff more competent, friendly”, is the second main reason given. The third reason given is cost-related except in Kenya where “wanted anonymity” features prominently. 5.4 Family Planning for Youth The debate concerning whether family planning services should be made available to adolescents, particularly sexually active adolescents has been raging on in many sub-Saharan African countries. The 1998 KDHS offers a unique opportunity to examine what people think about family planning for the youth as well as the adolescents’ own viewpoint. Although the information on family planning for the youth from the KDHS cannot be said to be representative of the other three countries, it does provide food for thought for family planning managers and implementers. Respondents were asked whether they thought it was acceptable for young persons under 18 years to be provided with family planning information and family planning services. Table 11 provides information on the percentage of adolescents who believe that persons under 18 years should be provided with family planning information and family planning services according to sex. The percentages of female respondents who believe that family planning information and family planning services should be available to persons under 18 years are 78.8 and 51.5 respectively. The corresponding percentages for male respondents are 87.8 and 68.2. As shown in Table 11, adolescent males think that family planning information should be provided for persons under 18 years more than their female counterparts, 86.8% compared to 75.4%. With regard to provision of family planning services to persons under 18 years, 68% of adolescent males are in favour compared to 50% of adolescent females. 5.5 Knowledge of Ovulatory Cycle A basic knowledge of reproductive physiology is useful for the successful practice of coitus related methods such as withdrawal, condoms or barrier methods but it is especially important for users of natural family planning also called periodic abstinence or the rhythm method (Central Statistical Office et al., 1997). The successful practice of natural family planning depends in part on an understanding of when during the ovulatory cycle a woman is most likely to conceive. Except in Ghana, in the three DHS, all women were asked, “During which times of the monthly cycle does a woman have the greatest chance of becoming pregnant?” Table 12 provides the results for adolescent females. Level of knowledge of the fertile period is very low among adolescent females. It is relatively highest in Kenya and lowest in Tanzania. The percentage of adolescent females who correctly mentioned that a woman is most likely to conceive in the middle of the ovulatory cycle varies between 6.9 in Tanzania and 13.4 in Kenya. In Tanzania, 71% of adolescent females said they did not know when the most likely time was, while 16% said “anytime” was most likely. At least, 40% of adolescent females in Kenya and Zambia said that they did not know the most likely time of ovulation. 6. Conclusion Although overall fertility levels in most of sub-Saharan Africa have begun to show signs of decline in the last decade or so, adolescent fertility is relatively high in the four countries. ASFR ranges from 90‰ among Ghanaian adolescent females to 158‰ among Zambian adolescent females. There are variations among the four countries. However, overall general patterns can be discerned. Early onset of childbearing is characteristic of the four countries. In Zambia, 31% of adolescent females have begun childbearing compared to 26% in Tanzania, 20% in Kenya and 14% in Ghana. At age 19 years, the percentage of adolescent females who have started childbearing ranges from 32% in Ghana to 61 in Tanzania. Information on age at first birth shows that among 18-19-year-olds, Tanzania is the country with the largest percentage (7.4%) followed by Zambia (5.9%), Kenya (5.8%) and Ghana (4.2%) in that order. As expected, increasing age is associated with increasing sexual activity. In Ghana and Tanzania, a larger percentage of adolescent females than males have had sexual intercourse, whereas the reverse is the case in Kenya and Zambia. The percentage of 19-year-old females who have had sexual intercourse ranges from 68 in Ghana to 84 in Zambia. Among the four countries, Zambia registered the highest percentages of adolescent males and females, who have had sexual intercourse. In view of early sexual initiation coupled with low contraceptive use among Zambia adolescent females, it is not surprising that they have the highest adolescent fertility. This phenomenon could be linked to the upsurge of HIV/AIDS pandemic in Zambia. As is the case for the adult male and female populations, there is a yawning gap between levels of contraceptive knowledge and use among adolescents. As adolescents initiate sexual activity and are exposed to the risk of pregnancy, pragmatic programmes particularly in the area of family planning should be initiated and implemented to fully address adolescents’ reproductive health needs. The temptation for a pregnant adolescent to resort to unsafe abortion should be avoided. The 1996 TDHS showed that 72% of Tanzanian adolescent females would be unhappy if they became prgnant. The corresponding figure for Ghanaian adolescent females was 91%. Among never married Ghanaian adolescent females it was 93%. The long-running debate between the moralists and pragmatists should give way to integration of youth and adolescent reproductive health concerns into existing population, education, gender and other development policies. Our findings indicate relatively high levels of contraceptive use among sexually active never married adolescent females. This seems to suggest that family planning managers and implementers have to revisit the issue of providing family planning services to adolescents particularly the sexually active ones in view of HIV/AIDS and the sexually transmitted infections. The most widely used modern method of contraception by adolescents is condom and its use should be encouraged so as to promote safe sex among adolescents. The data on provision of family planning information and services from the KDHS, although by no means representative of the four countries, points to softening of the hard line position of the recent past. More than half of adult men and women in Kenya thought that it was acceptable for persons under 18 years to be provided with information and services related to family planning. The Kenya findings are supported by a stakeholder analysis done for five regions in Ghana which reported that 58% of opinion leaders were of the view that adolescents should be provided with family planning services (Population Impact Project, 2001). This calls for “health for adolescents” by offering more adolescent friendly services, training and re-training service providers to be more adolescent friendly or making health services cheaper and more accessible particularly in the rural areas where majority of adolescents live. The study has also highlighted low levels of knowledge about reproductive and sexual health. The proportions of adolescent females who correctly mentioned that a woman is most likely to conceive in the middle of the ovulatory cycle were 6.9% in Tanzania, 7.4% in Zambia and 13.4% in Kenya. This low quality of information on reproductive health was also found among 12-19 year-old Kenyans (Ajayi et al., 1985). The knowledge base in reproductive physiology of in and out-of-school adolescents should be strengthened. Then too, sexuality education and other emerging issues such as human rights, harmful practices and violence should be integrated into population education and reproductive health education programmes. There is the need to strengthen teacher training, parent education and community outreach. To a large extent the inter-country variations highlighted in this paper can be attributed to differences in levels of education and various sociocultural practices and beliefs in these countries. Paucity of qualitative data has not permitted examination of the social and cultural situations in the four countries that might throw some light on the intra-country differences exhibited by the DHS data. However, as a policy measure, adolescents particularly adolescent females should be encouraged to attain at least secondary education because education is good in its own right. In spite of their limitations, the four Demographic and Health Surveys have shed considerable light on adolescent fertility and reproductive health at the national level. Firstly, more detailed data should be collected on barriers to the use of contraception among adolescents and circumstances surrounding sexual initiation and decision to practise contraception. Secondly, it is also important to collect data to bridge the knowledge gap relating to interactions of adolescents with service providers. Finally, both qualitative and quantitative data collection approaches should be used to collect information on socio-cultural practices and beliefs so as to provide a more accurate picture of adolescents’ sexual behaviour and a better understanding of the circumstances surrounding their sexual relationships. References
Copyright 2002 - Union for African Population Studies The following images related to this document are available:Photo images[ep02011t4.jpg] [ep02011t3.jpg] [ep02011t10.jpg] [ep02011t9.jpg] [ep02011t12.jpg] [ep02011t11.jpg] [ep02011t7.jpg] [ep02011t8.jpg] [ep02011t6.jpg] [ep02011t1.jpg] [ep02011t2.jpg] [ep02011t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}