 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
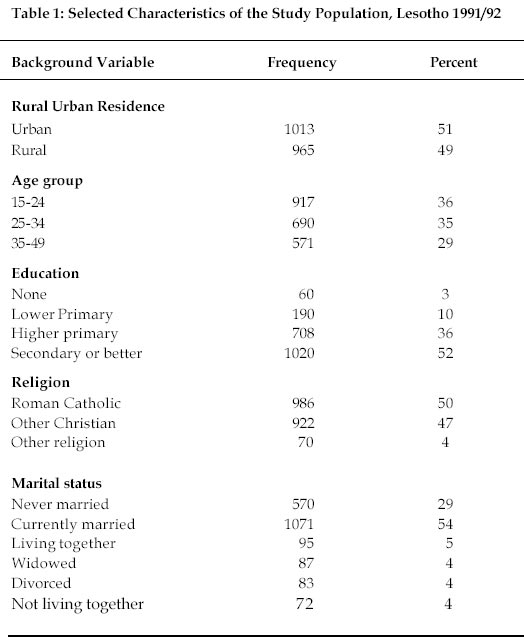
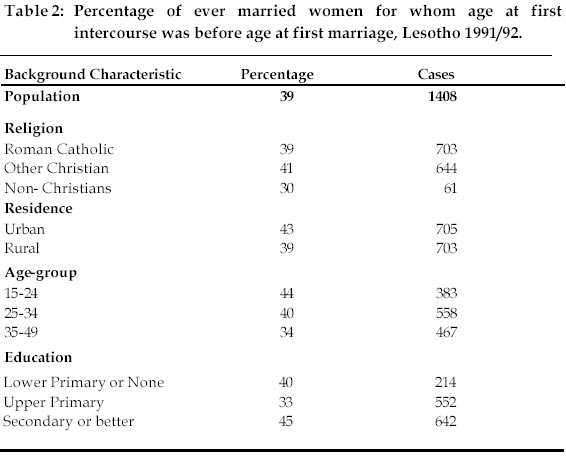
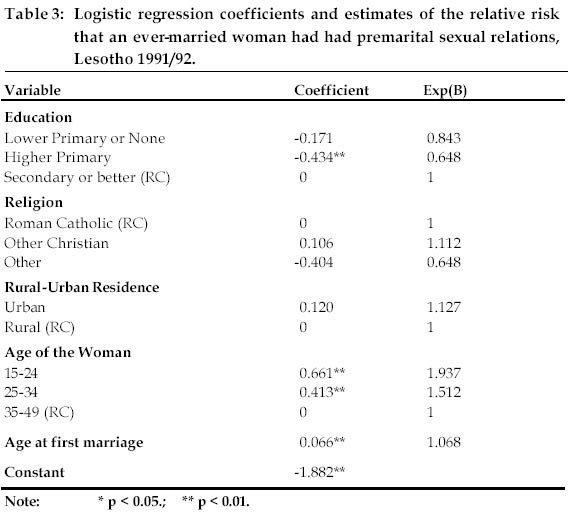
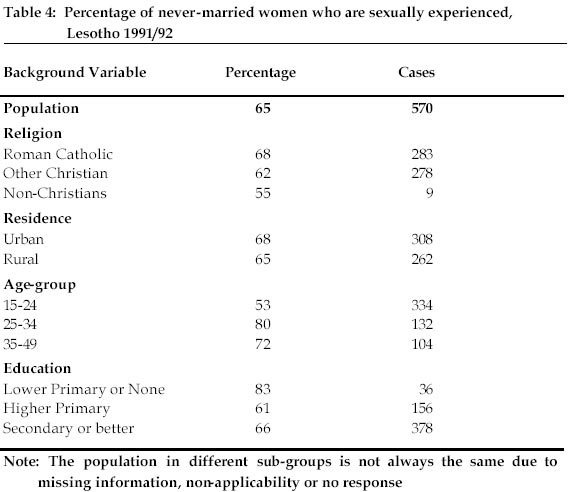
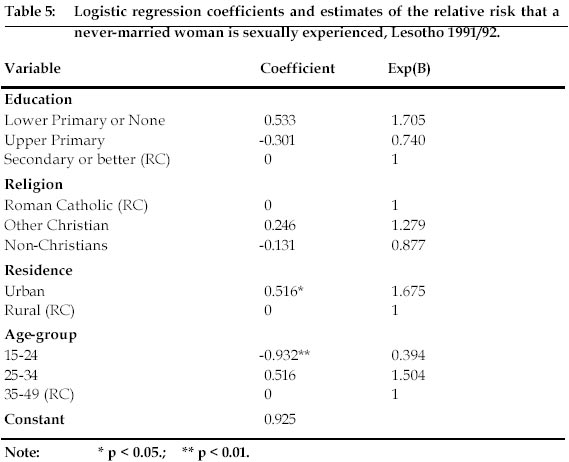
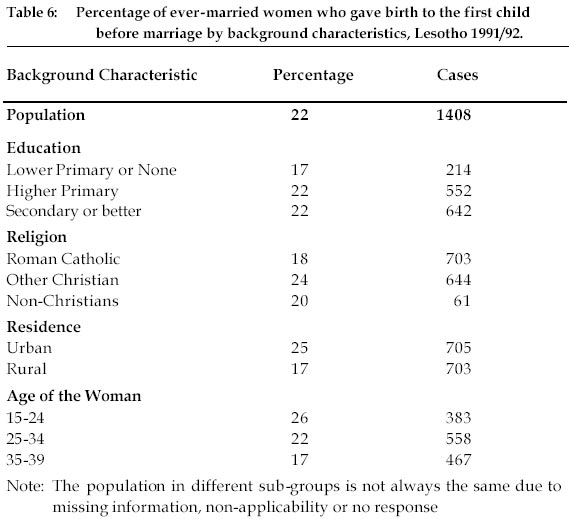
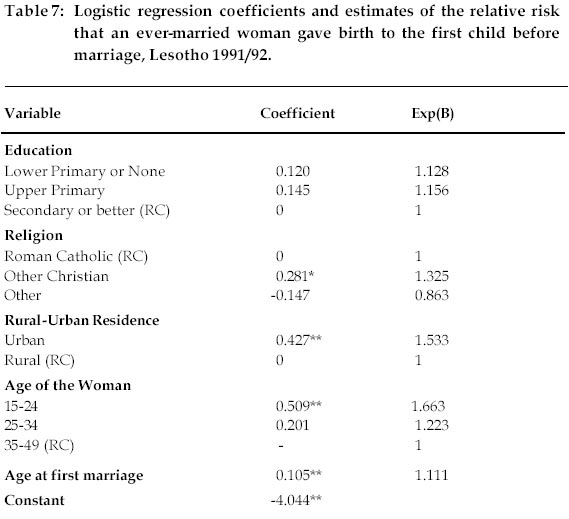
African Population Studies, Vol. 17, No. 2, 2002, pp. 99-112 Pre-Marital Sex and Childbearing in Lesotho Tiisetso Makatjane Senior Lecturer in Demography, Department of Statistics and Demography, National University of Lesotho Code Number: ep02012 Abstract This study investigated the prevalence of premarital sex and childbearing in Lesotho. The data used in the study are obtained from the Lesotho 1991/92 Demographic and Health Survey. A sample of 1978 women aged 15-49 was used for analysis. Findings indicate that prevalence of premarital sex has more than doubled between 1977 and 1992 in Lesotho. Never married women living in urban areas are more likely to be sexually experienced than their counterparts residing in rural areas. Contrary to the assertion that education is correlated with premarital sex and childbearing, the results of the study show no evidence of a relationship between education and sex and childbearing before marriage. Norms of the society discouraging sex before marriage have eroded more in urban areas than in rural areas. Hence urban environment provides a conducive environment for experimenting with sex before marriage. Résumé Cette étude examine la prévalence des rapports sexuels avant le mariage et de la grossesse au Lesotho. Les données utilisées proviennent du recensement démographique et de santé de 1991/92. Un échantillon de 1978 femmes âgées de 15 à 49 ans a été utilisé pour les besoins de l'étude. Les résultats obtenus ont montré que les rapports sexuels avant le mariage ont plus que doublé entre 1977 et 1992 au Lesotho. Les femmes non mariées vivant dans les centres urbains ont plus de chance d'avoir une expérience sexuelle avant la mariage que celles résidant dans les zones rurales. Contrairement à l'hypothèse qui veut que l'éducation soit correlée avec les rapports sexuels avant le mariage et la grossesse, les résultats de l'étude n'ont montré aucun rapport direct entre l'éducation, les rapports sexuels et la grossesse avant mariage. Les normes de la société qui découragent les rapports sexuels avant le mariage se sont plus estompées en ville que dans les zones rurales. L'environnement urbain est donc un facteur favorisant les rapports sexuels avant le mariage. Introduction Traditionally the Basotho nation attached much importance to child-bearing. Polygyny and various practices applied in the past in Lesotho provided an opportunity for a man to have many children. Some of the customs include practices such as a man marrying a woman for a fictitious son or a son who died before marriage. Sometimes a girl took the place of a dead sister or a married childless woman married another woman to bear children for her (Poulter et al, 1981; Makatjane, 1987). These practices were meant to add more members to the man's lineage. On the other hand, practices such as prolonged breastfeeding as well as sexual abstinence were meant to ensure child survival. It is obvious that Basotho were interested in both quantity and quality of children. The high value attached to procreation notwithstanding, child-bearing before marriage was not considered an acceptable option through which more members could be added to a man's lineage. A person who has sexual intercourse with an unmarried girl commits the actionable legal wrong of seduction that makes him liable to pay six heads of cattle as compensation (Poulter et al, 1981). The extent to which the punishment has been a deterrent is difficult to determine in the absence of reliable statistical data or any other empirical information. However, available information for some countries in southern Africa does suggest high incidences of pre-marital sexual practices. For instance as early as 1934, high proportions of unmarried women giving birth to children were already observable in Botswana and by 1974 the proportion of women of marriageable age remaining unmarried and the number of children born to unmarried women had substantially increased (Lye and Murray 1980: 107). It is estimated that about 100 million youths become sexually active every year world-wide (Anderson, 1994:12). This sexual activity is not necessarily accompanied by safe sex. Other than childbearing before marriage which was a preoccupation of most traditional societies when socialising the youth against sex before marriage, there is the current problem of sexually transmitted infections (STIs) and HIV/AIDS in particular. Since an increase in sexual activity among youth is not accompanied by safe sex or use of modern contraception, youth become a target for HIV and STIs. According to the figures of the AIDS Control Unit of the Ministry of Health and Social Welfare, a fifth of the reported cases of AIDS in Lesotho as of 1997 are of never married individuals (Ministry of Health and Social Welfare, 1997). As Anderson (1994:12) correctly indicates, campaigns that discourage youth from early sexual activity must speak explicitly about the danger of infection with HIV or other STIs. Studies on child mortality and marital status have documented that children of never-married persons have a higher risk of mortality than legitimate children do (UN, 1985). The higher risk of mortality for illegitimate births is normally attributed to the fact that never-married mothers are young and lack the experience of child care. Knowledge about adolescent sexuality coupled with knowledge about contraceptive prevalence among never-married mothers can go a long way in making informed policies regarding reduction of infant mortality. Maternal mortality is quite high in the developing countries and complications related to teenage pregnancy are a leading cause of death among teenage mothers world-wide (Lori, 1995:24). It then follows that knowledge about premarital sex can go a long way in assessing the consequences of premarital sex on maternal mortality. Strategies for reduction of maternal mortality can benefit more from premarital sex information as premarital sex is correlated with teenage pregnancies which in turn are related to maternal mortality. Premarital childbearing is also a social problem. Marriage among other things is a union through which children are legitimised to belong to a particular lineage. Marriage plays an important role in determining one’s place within the hierarchy of a particular lineage. Children of married women have a place within the lineage of both their fathers and that of their mothers. Unfortunately the place of children borne before marriage remains a thorny issue always resulting in the humiliation of such children during traditional gatherings where one’s position within the lineage needs to be established. The social stigma attached to both unmarried mothers and their children remains a serious social problem among Basotho. The extent to which tradition is giving in to developmental changes is not clear. It is noteworthy that constitutionally there is no discrimination against children born out of wedlock in Lesotho and their mothers are not considered minors before the law as is the case among married women. Abandoned children are a problem that is worsening every year. It is an indisputable fact that some women do abandon their children at hospitals after delivery and the number of such children is increasing with time. It is also a fact that newly born children are found abandoned in a number of places and such children are brought to hospitals for care taking. The Ministry of Health and Social Welfare's expenditure for financing the feeding of abandoned children is continually increasing. While it may not be correct to claim that abandoned children are those of never married mothers, never married mothers are more desperate for financial support for their children than married mothers. It is apparent therefore that knowledge about the prevalence of premarital sex can give an insight concerning the consequences of premarital sex both socially and otherwise. Information on induced abortion is scanty in Lesotho although hospital data suggest that incidences of incomplete abortions could be quite high. For instance from January to September 1994, more than half (54.6%) of females aged less than 24 years admitted to the gynaecology ward at QE II hospital were cases of incomplete abortion while 10% of all deliveries at the same hospital in 1992 were abortions (Ministry of Health and Social Welfare, 1994). High incidences of abortion among adolescent women have been observed in other African countries (Centres for Disease Control and Prevention, 1999). Since modern contraception use for never-married women is lowest (6 % compared to 21% for currently married women and 15% previously married ones) among women in their reproductive ages (Makatjane, 1995) yet they are sexually experienced (Mturi, Tuoane and Diamond, 1997), and their reliance on abortion is likely to be highest. In a study of court cases on abortion, reasons given for abortion (Morojele, 1991) suggest that never married women are more likely to rely on abortion than ever married women. Prevalence of premarital sex can therefore provide an indication of the unmet contraception need among never married women. This is particularly important as family planning service providers are not necessarily user friendly to unmarried women (Tuoane et. al., 1998) yet unprotected sex can expose them to unwanted pregnancies, sexually transmitted infections as well as HIV/AIDS infections. Availability of data notwithstanding, there is strong belief among Basotho that formal education is positively correlated with premarital sexual experience (Tau, 1994). It is believed that formal education has caused erosion of certain practices that were traditionally meant to discourage premarital sex which in turn would lead to avoidance of pre-marital childbearing. Most food stuffs which were not to be eaten by youth because they were believed to stimulate sexual desire are recommended by health practitioners. Checking of girls' chastity by both elderly people before marriage and the bridegroom at consummation of marriage have also eroded as a result of education (Makatjane, 1987; Tau, 1994). Lesotho 1991/92 Demographic and Health Survey provides an opportunity to examine prevalence of sex and childbearing before marriage among Basotho women and whether formal education is correlated with the prevalence of premarital sex and childbearing. Logistic regression is used to identify factors that are associated with premarital sex and childbearing. Due to data limitations, it is not possible to address most of the problems raised in the preceding paragraphs that are correlated with premarital sex and childbearing. However, the finding of this study will be informative concerning the extent of implications of sex and childbearing before marriage on health and other social problems as outlined in the preceding paragraphs. The DataLesotho 1991/92 Demographic and Health Survey is the source of data for the present analysis. The survey was a national representative sample survey covering both urban and rural households. A total of 3498 women aged 15-49 were interviewed, but, due to missing information, particularly on age at first birth and age at first intercourse, only 1978 women whose information is complete form the sample size for the analysis. However, the distribution of women with missing information by age, rural urban residence, education and religion is similar to that of the total sample suggesting that there is no group which is more affected by missing information than others. Table 1 presents the characteristics of the study population. The majority of the respondents were Christians, currently married and highly educated. Age and residence distributions showed almost equal percentages between rural and urban residence as well as among different age groups. The equal distribution between rural and urban residence suggest that urban areas are over represented in the sample and the subsequent tables are thus based on weighted data. Discussion of sex is a taboo in most societies and Lesotho is no exception. Asking people sex related information is problematic. This is further complicated by the fact that in most surveys, interviewers are normally younger than respondents. Unfortunately, there is no way of knowing how much of the non-response is due to age difference between the respondent and the enumerator if no provision was made for the interviewer to report such problems as was the case with the Lesotho 1991/92 Demographic and Health Survey. In all 39% of the respondents did not provide their ages at first intercourse, but coupled with unknown ages at first marriage, information on age before marriage could not be calculated for 49% of the respondents. Reservations about data quality notwithstanding, the survey provides useful information about correlates of sex and childbearing before marriage. Moreover, previous studies based on the same type of survey have provided informative findings (Meekers, 1994; Toroitich-Ruto, 1997). Given the large number of respondents with missing information, a certain degree of caution and skepticism should be maintained when considering the results. As indicated in the introduction, while on the one hand Basotho like most communities discouraged sex before marriage, the figures in Table 2 on sexual experience before marriage, on the other hand, show that younger women are more prone to experiencing sex before marriage than older ones. Christians have a higher percentage of women who have experienced sex before marriage compared to non-Christians while there does not seem to be much difference between rural and urban residence or is there any discernible pattern of differences among the different educational groups in terms of the percentage of women experiencing sex before marriage. However, with 39% of its ever married women reporting premarital sex, Lesotho is within the range of most countries in Sub-Saharan Africa. Comparative proportions of ever married women who became sexually experienced before marriage for some African countries are for Burundi 20%, Ghana 60%, Kenya 61%, Liberia 59%, Mali 13%, Togo 65% and Zimbabwe 48% (Meekers, 1994:52). Table 3 presents logistic regression coefficient estimates of the relative risk that an ever-married woman had had premarital sexual relations. The factors associated with the likelihood of experiencing sex before marriage are age of the woman, age at first marriage and education. Women who have completed higher primary are less likely to have experienced sexual intercourse before marriage than women who have completed secondary education or better while women aged 15-24 and 25-34 are more likely to have experienced sex before marriage than women aged 35-49. The effect of rural urban residence and religion on premarital sexual experience is not significant. In confirmation to what is suggested by the figures in Table 2 that premarital sex is increasing overtime (the percentage of women who were sexually experienced before marriage is highest among young women), after controlling for the effect of other factors, the figures in Table 3 do support an increase in premarital sex overtime. As expected, age at first marriage is positively correlated with premarital sexual experience resulting from long exposure to the risk of experiencing premarital sex. Sexual experience differences among never married women by background do not portray any difference except for education where women with no education or lower primary have the highest proportion of respondents who were sexually experienced and age where women aged 15-24 have the smallest proportion of women who were sexually experienced (Table 4). However, with 65% of the never-married women reporting that they are sexually experienced, Lesotho is one of the countries in Sub-Saharan Africa with a high percentage of never-married women who are sexually experienced. Compared to other countries in Sub-Saharan Africa where data are available, Lesotho is second to Liberia with 81% of its never-married women reporting sexual experience, then Togo with 60% while for Ghana and Kenya the percentage is around 50%, 26% for Zimbabwe and around 5% for Mali and Burundi (see Meekers, 1994:52). Contrary to the argument that formal education is associated with sexual experimentation among never married women, the statistics in Table 4 and the logistic regression estimates in Table 5 do not support this argument. According to the statistics in Table 4 never-married women with lower primary or no education appear to be more likely to be sexually experienced, while the effect of literacy does not appear to be significant after controlling for the effect of the other variables (Table 5). However, age and residence have a significant effect on sexual experience among never-married women. Never married women residing in urban areas are 1.7 times more likely to be sexually experienced than their counterparts residing in rural areas, while never married women aged 15-24 are less likely to be sexually experienced than their counterparts aged 35-49. The significant effect of age on sexual experience among never married Basotho women suggest that the length of exposure to the risk of sexual experience is more important than literacy in influencing the likelihood of sexual experience. That is, older never-married women have had a longer exposure to the risk of experiencing sex after menstruation than younger never-married women hence the significant negative effect of age on the likelihood of a never-married woman being sexually experienced. The significant effect of residence on sexual experience could be due to a number of factors. Firstly urban residence provides a conducive environment for experimenting with sex. Secondly absence of elders who otherwise would control sexuality of the young exposes the young to the risk of experiencing sexual activity before marriage. According to Tau (1994) urban parents have little time for their children due to work commitments and this gives urban children the chance to experiment with sex. Premarital ChildbearingAccording to the figures in Table 6 premarital childbearing prevalence is increasing with advancement in education while the opposite is the case with age of the women. With respect to religion there are no serious differences in premarital childbearing prevalence while according to residence the prevalence for urban women is high by 8 percentage points. However, Lesotho 1977 fertility survey results put the prevalence of premarital childbearing among ever married women at around 10% (Bureau of Statistics, 1981; Makatjane, 1987) while the figures in Table 6 put it at 22%. There is no doubt therefore that the prevalence of premarital births has increased in Lesotho. According to the figures of the 1991/92 Lesotho Demographic and Health Survey only 5% of never-married women is currently using modern contraception relative to 21% for currently married women and 15% for previously married ones (Makatjane, 1995). While the low level of family planning prevalence could be a reflection of non-availability of a full time partner (Makatjane, 1995), the high proportion of never-married women who are sexually experienced coupled with the low use of modern contraception among these women suggest a high risk of premarital childbearing leading to the doubling of premarital childbearing prevalence between 1997 and 1991/92. According to the logistic regression estimates of the effects of background variables on the likelihood of experiencing premarital birth, age of the woman, age at first marriage, religion and rural urban residence have a significant effect on premarital birth experience among Basotho women (Table 7). Other Christians are 1.3 times more likely to have experienced premarital child birth than their Catholic counterparts while women aged 15-24 are 1.7 times more likely to have experienced premarital child birth than women aged 35-49. As expected, women who marry late are more likely to have experienced birth before marriage than their counterparts who marry early. However, contrary to the held notion that education could be responsible for increasing premarital child bearing in Lesotho, the figures in Table 7 point to the contrary. After controlling for the effect of other variables, education does not have any influence on premarital childbearing among ever married women. Women who marry early experience sexual intercourse at an early age because of entering into sexual unions early hence their lower likelihood of experiencing birth before marriage. The mean age at first sexual intercourse for women whose age at first marriage is less than 20 years is 17.8 years compared to 19.1 for women whose age at first marriage is 20 years or more. Concerning women who marry late, they stay long after menarche before getting married and thus increasing the chances of experiencing childbearing before marriage leading to a significant relationship between age at first marriage and the risk of experiencing childbearing before marriage. Premarital sex is high (39%) in Lesotho while premarital child bearing among ever married women has increased from a low of 10% in 1977 to 22% in 1991/92. The increasing trend in premarital sexual experience is further supported by the figures in Table 3 where younger women (15-24 and 25-34) are more likely to have experienced premarital child bearing than old (35-49) women. Age at first marriage, age of the woman and education are significant correlates of premarital sexual experience (Table 3). Ever married women who entered into marriage late are more likely to have experienced premarital sex than women who entered marriage early. Younger ever married women are more likely to have experienced premarital sex than their counterparts aged 35-49. Among never married women, rural-urban residence and age are important factors influencing premarital sexual experience (Table 5). Never married women living in urban areas are 1.7 times more likely to be sexually experienced than their counterparts residing in rural areas while never married women aged 15-24 are 40% less likely to be sexually experienced than those aged 35-49. Age at first marriage, age of the woman, religion and rural-urban residence are significant factors influencing premarital childbearing (Table 7). Ever married women aged 15-24 are twice more likely to have experienced premarital birth than ever married women aged 35-49 while other Christians are 1.3 times more likely to have experienced premarital birth than their Catholic counterparts. As expected late entry into marriage is associated with premarital birth experience while ever married women residing in urban areas are 1.4 times more likely to have experienced premarital birth than their counterparts residing in urban areas (Table 7). Results suggest that sexual experience among never married women is becoming common in Lesotho. By delaying age of entry into marriage through schooling, education exposes women to the risk of experiencing sex before marriage. The relationship between education and sexual experience among never married women is therefore indirect. That is, educated women have a higher relative risk of experiencing sex before marriage because they have had a longer exposure period to the risk of experiencing sex before marriage through late entry into marriage resulting from staying long at school. Providing women with education beyond primary level has been advocated for in many fora because of the relationship between maternal education and mortality and fertility as well as eliminating educational differences between males and females. Since keeping girls long at school can expose them to the risk of premarital childbearing, it is important to find a solution to the problem of premarital childbearing. Family Life Education Programme, which was started within the Ministry of Education, can go a long way in addressing the problem of teenage pregnancies among a number of problems facing the youth today. Unfortunately the programme did not really take off beyond curricular development and probably piloting in few secondary schools. It is important for the government to resuscitate the programme. The programme could be made to work in conjunction with the “Youth Reproductive Health Corner”, a service introduced by the Ministry of Health and Social Welfare addressing reproductive health issues of the youth. The youth corner is a place where reproductive health issues of the youth are addressed away from the normal place where everybody usually comes for consultation. The programme is becoming very popular as it provides a conducive environment for youth. The increasing prevalence of premarital sex among never married women which is not accompanied by any form of protection against premarital childbearing has both social and health implications. As argued in the introduction, an increase in premarital sex will lead to an increase in premarital childbearing. Since in the majority of cases teenage pregnancies are a result of ignorance about reproductive health, most teenagers will try abortion once they find themselves pregnant. Since abortion is illegal, unsafe abortion will be resorted to resulting in high maternal mortality. It was also mentioned in the introduction that children of teenage mothers are more prone to mortality because teenage mothers are emotionally and psychologically ill-prepared for child care. They lack the experience and resources to raise children properly hence infant mortality is most probably going to increase as the proportion of infants born of teenage mothers increase. On the other hand, social discrimination against children born out of wedlock is likely to continue to be a problem during traditional ceremonies making such children feel insecure and bitter for being rejected within the lineage of their mothers while other children have the benefit of both their mothers and fathers lineages. While childbearing among ever married women enhances their social status within both their husbands and their own lineages, for never married women, childbearing does not improve their social standing. Although motherhood status could provide them with the emotional satisfaction that they are capable like other women to bear children, like their children they suffer a certain amount of social discrimination because of their unmarried status. In fact a childless ever married woman enjoys a better social status than an unmarried woman with children. Due to lack of proper education on reproductive health, an increase in the prevalence of premarital sex will expose teenagers to the higher risk of contacting HIV and STIs. As indicated earlier, it is high time that reproductive health is taught to teenagers. It would be ideal to introduce it in schools, at least at the secondary level of education. Resuscitating the introduction of Family Live Education in secondary schools beyond the pilot schools would go a long way in addressing reproductive and health needs of the youth. Since the Catholic Church; which owns more than a third of the secondary schools in Lesotho (Lesotho government, 1992:146); as a matter of policy is generally against use of modern contraceptives, introduction of Family Life Education in secondary schools, might have problems of being accepted in Catholic schools if modern contraceptive use is part of what has to be taught. That is, generally the concept of Family Life Education might be accepted in Catholic schools except topics discussing modern contraceptives, particularly their use. Introduction of Family Life Education in school should also be accompanied by availability of reproductive health services including family planning services in all the health centres within the country so that teenage girls can have access to contraceptives to protect themselves against unwanted pregnancies. Since as a matter of policy the Catholic church does not offer modern contraceptives in its health facilities (Lesotho Government, 1994:209), there is a need for the government to enter into negotiations to persuade all owners of health facilities to offer modern family planning services in their health facilities. This would go a long way in making family planning services accessible to the majority of the women particularly those living in the rural and remote villages. This is particularly so because church owned health facilities are a sizeable proportion (about 40%) yet some of them might not be offering modern family planning services as a matter of policy. This would further provide a conducive environment towards making the policy of government of making modern contraceptives available to most women of reproductive ages a reality. References
Copyright 2002 - Union for African Population Studies The following images related to this document are available:Photo images[ep02012t4.jpg] [ep02012t7.jpg] [ep02012t2.jpg] [ep02012t1.jpg] [ep02012t6.jpg] [ep02012t5.jpg] [ep02012t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}