 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 18, No. 1, April 2003, pp. 81-95 Residential Density and Adolescent Reproductive Health Problems in Ibadan, Nigeria ADEBOYEJO A.Thompson1 and ONYEONORU I. P. 2 1Department of Urban and Regional Planning,
Ladoke Akintola University of
Technology,
Ogbomoso,
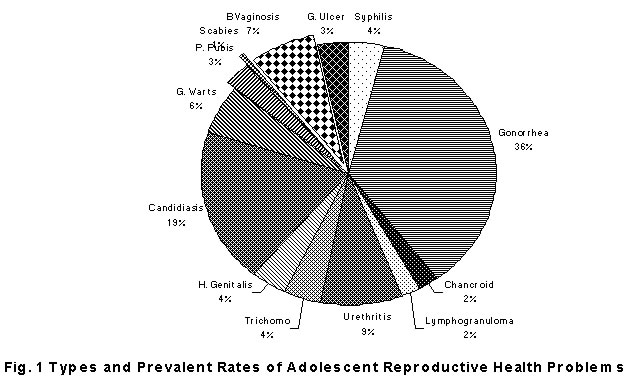
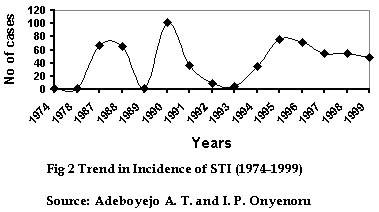
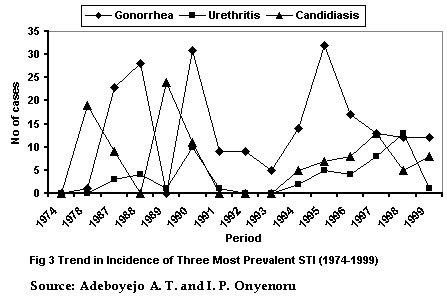
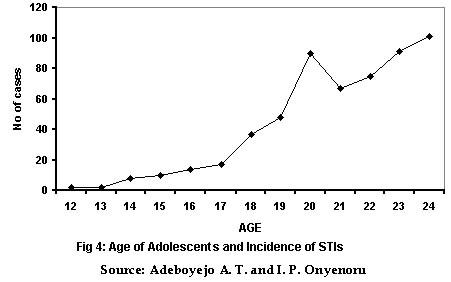
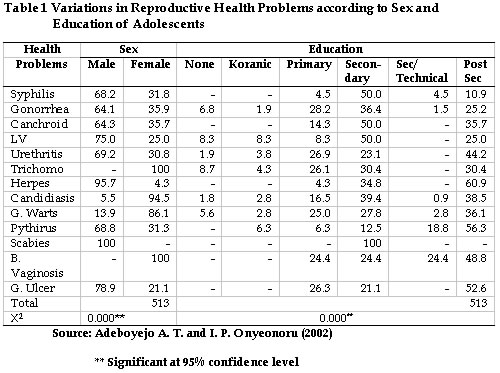
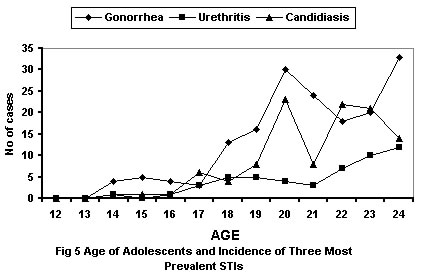
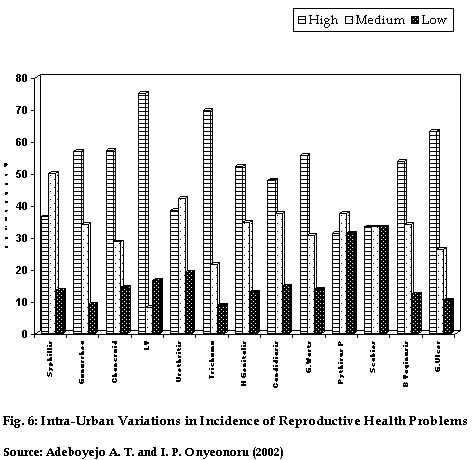
Nigeria Code Number: ep03006 Abstract Within the framework of the home environment which adolescents live, this paper analyses the components of adolescent reproductive health problems, the incidence, prevalent rates, as well as their intra urban variations. The socio-economic and the home environmental correlates of the most common infections are also examined. The study which was based on analysis of hospital records of diagnosed cases reveals that, three most common STIs among adolescents in the study area are Gonorrhea, Candidiasis, and Non-Specific Urethritis. The incidence is highest among adolescents in the high density but low class residential areas than their counterparts in the medium and low density areas. Prevalent rates were found to be highest among adolescents in the 17 to 24 ages and that male adolescents were more affected in all cases than their female counterparts. The trend in incidence between 1974 and year 2000 is a fluctuation which tends more towards increase than decline. Résumé Dans cet article, l'auteur analyse les éléments constitutifs des problèmes de santé de la reproduction des adolescents dans leur milieu environnemental, l'incidence de ces problèmes, leur taux de prévalence ainsi que leurs variations dans les villes. Les rapports qui existent entre les facteurs socio-économiques, environnementaux et résidentiels des infections les plus courantes sont étudiés. Cette étude qui se fonde sur une analyse des relevés de cas diagnostiqués d'hôpitaux, montre que les trois MST des adolescents les plus fréquemment rencontrées dans la zone d'étude sont le gonorrhée, le Candidiasis et diverses forme d'uretérite. L'incidence est plus élevée parmi les adolescents de basse classe et vivant dans les zones de forte densité que ceux des classes moyennes mais vivant dans des zones de densité faible. Les taux de prévalence étaient plus élevés parmi les adolescents dont l'âge était compris entre 17 et 24 ans et les adolescents de sexe mâle étaient plus affectés dans tous les cas que leurs partenaires de sexe féminin. La tendance de cette incidence entre les années 1974 et 2000 est une fluctuation plus marquée vers l'augmentation que vers la baisse. Introduction The differentiation of the urban landscape into residential densities or neighbourhoods is an inevitable consequence of urban development, and, a net outcome of the complex processes involving individual and family choices and preferences of housing needs, financial capabilities, existing housing supply, information flows and, housing market manipulations. In several ways (whether physical structure, housing quality, ownership patterns, household structure, environmental quality etc.), residential densities differ from each other, but all are important because of their impact on behaviour and implications on health and well-being. As Timms (1976,) categorically stated, "the behaviour of most individuals is set within a neighbourhood context and, even if life involves association with actors from outside the immediate locale, neighbours remain a constraint to be reckoned with" Although there is a dearth of empirical work on residential density and reproductive health, nevertheless, there are few studies on the relationship between density and overcrowding and incidence of social problems or social pathologies (Faris and Dunham 1939, Bagley et al 1976; Giggs 1973) among others. For instance in Netherlands, Levy and Herzog (1974) related hospital admissions, delinquency and illegitimacy among others with density. Again Schmitt (1966) found clear links between density and such problems as family disorganisation, physical illness and mental breakdown in Honolulu. The fact that there is a close association between incidence of truancy, family breakdown, infectious and communicable diseases and residential density has also been reported (Bagley et al 1976; Giggs 1973). Similarly in a study of incidence of social problems in inner London and Isle of Wight (UK), Rutter et al (1974) showed that the problems were much higher in London While adolescents reproductive health issues particularly within the context of urban living environment has not been given much research attention, there is a growing body of literature on adolescents' sexual expression in Nigeria. It has been observed for instance that, youngsters do not only live in separate residencies within cities, they increasingly practice premarital sex (Feyisetan, et al 1994; Orubuloye, et al 1991), at an early age, and, with multiple partners (Isiugu-Abanihe, 1994; Makinwa-Adebusoye, 1992). Nigeria Demographic and Health Survey (1992) indicated that Nigerian girls had their first sexual encounter at the median age of about 16 years. Similar findings were made in the study conducted by Adegbola and Babatola (1999) in Lagos State where the first sexual intercourse for males was found to be 16 years - about a year younger than the average for females. Makinwa-Adebusoye and Feyisetan (1994) observed that 82% of females and 72% of males had intercourse by age 19 while 80% of the male students studied in Ile-Ife were found to be sexually active in the past one year with more than half reporting sex with multiple partners. Commenting on the high rates of adolescent fertility in Nigeria, Makinwa-Adebusoye and Odumosu (1998), expressed concern that urban adolescents continue to record high rates of illegally induced abortion with little regard for their own reproductive health. Unmarried girls in Ibadan city were twice as likely to be practicing contraception as married women in spite of the refusal of hospitals and family planning clinics, at that time, to provide services for the single (Caldwell,et al 1992) In his analysis of a sub sample of 1540 adolescents and young adults aged 15-24, years derived from the 1990 Nigeria Demographic and Health Survey, Isiugu-Abanihe (1994) revealed that 38% of the adolescents were sexually experienced. Exposure to pre-marital sex was observed to increase with age, from less than 10% at age 15, to 77% at age 24. Mean age at first sexual encounter was 16.7 years with little variations among socio-cultural characteristics. Multivariate analyses of the sample also show that sexual exposure, coital frequency and sexual activity vary considerably with such variables as residence, ethnicity, educational attainment, work status and current age. An important observation on adolescent sexuality with serious reproductive health implication is to the effect that, sexual activity is not only high, but it may perhaps be on the increase among unmarried youths in urban areas of Nigeria (Nichols, et al, 1986; Gyepi-Garbrah, 1985; Omu, et al, 1981). If the above observation is a truism in Ibadan, a pre-colonial urban centre, it implies that, the youths in this part of the country are dangerously exposed to Sexually Transmitted Infections (STIs) and by implication HIV/AIDs infection. Our position in this paper is a case for prevention, detection and treatment of STIs as a strategy for the prevention of HIV infection. Reproductive health issues as the ones affecting adolescents, no doubt should be of colossal public health importance in both the developed and developing countries. The morbidity associated with STIs, their complications and implications, particularly the spread of HIV/AIDs and the socio-economic costs of such issues as teenage pregnancies and abortions compel a greater research attention and more pragmatic solution. Against this background, the possibility of the influence and impact of aspects of the home environment on adolescent sexuality and reproductive health, as well as the prospects of residential density-specific intervention programmes provide scientific motivation for this study. The types of reproductive health problems discussed here are essentially STIs. However other reproductive health problems encountered in the hospital case notes used for the study, particularly those of bacterial Vaginosis, Genital Ulcer Disease (GUD) and Pelvic Inflammatory Disease (PID) are discussed to provide a vivid picture of the scope of adolescents reproductive health issues in the study area. Data Sources and Methodology The analysis is based on secondary data sources, the hospital record of relevant cases, which were collected from the STC clinic of The University College Hospital, UCH, Ibadan. The hospital is a referral teaching hospital, with scope of service extending beyond the city location. The method of data collection involved review of hospital case notes, from the most current cases. The constraints of age of respondents (12 to 24 years), their geographical location within the city1, the very busy schedule of the hospital, coupled with the non-chronological method of arranging case notes, compounded the process of search and replacement of case notes. In all, a total of 513 relevant cases were extracted after going through about 25 years record (1999 to 1974). The relevant information was then collected with the aid of a structured questionnaire designed for the purpose. The data was processed with Statistical Package for Social Sciences (SPSS). Results and Discussion Components of Adolescents Reproductive Health Problems It is obvious from the illustration in figure 1 that the STIs reported among adolescents in the study area range from the traditional venereal diseases of Gonorrhea and Syphilis to the bacterial, parasitic and viral syndromes associated with Chlamydia trichomatis, Bacterial vaginosis and Trichomona vaginalis. The three most prevalent are: Gonorrhea, (32.5 %), Candidasis of the genitals (17.2%) and Non - specific urethritis (8.2%). The presence of these STIs, it has been reported, has serious implications for the malignant systemic infections caused by Human Immunodeficiency Virus (HIV) (United States CDC, 1998). Data on HIV/AIDS is though officially not available, suffice to say here that, adolescents in this part of the world are not untouched with the scourge of the dreaded disease. This is reinforced by the fact that, such STIs as Chancroid, Syphilis, Trichomoniasis, Bacterial Vaginosis, found in this study area, have been linked to an increased risk of HIV/AIDs (Feldblum,1998, Osmond, 1998). The observation by the World Bank (1993) to the effect that STIs are the second most frequent cause of sickness and death among females of reproductive age in developing countries calls for more consciously formulated policies targeted towards improving adolescents' reproductive health in the country. Growth Trend of Stiother Reproductive Health Problems The result as illustrated in figure 2 shows that there was a sharp increase in total number of observed cases from near zero in 1974 and 1978 to about 70 in 1987 and 1988. The highest number of cases (102) were observed in 1990. However, there was a gradual decline in incidence during the five year period spanning 1995 to 1999, when reported cases decreased from the 1995 figure of 76, to 49 cases in 1999. The interpretation of the growth trend should be treated with caution as the observed pattern tends to reflect more of the history of data or record keeping in the hospital than actual number of reported cases. First, it should be noted that apart from one case in 1974 and 1978, no other case was reported or recorded between 1974 and 1977, and between 1979 and 1986 when record keeping was probably at its infancy stage or the case notes had simply been stacked away. The fact that the history of comprehensive record keeping dates back to about two decades ago is borne out by this finding. The profile described above also highlights the inconsistent nature of data keeping in developing countries generally. Otherwise, that only one case was reported in 1989, while 66 and 102 cases were recorded, respectively in 1988 and 1990, defy any scientific explanation. For conclusive remark on the growth trend of reproductive health problems in the study area, we rely on the pattern observed for the short period between 1995 and 1999 during which global concern for societal health status, particularly the scourge of HIV/AIDS necessitates serious attention on more accurate and comprehensive record keeping of reported cases of Sexually Transmitted Diseases. Thus the decline in incidence of STI during the period is perhaps consequential upon the various awareness campaigns on the scourge of HIV/AIDS and promotion of safe sex practices. Even then, the rate of decline which is just about 35% for the five year period may be too small to be regarded as a feat. Figure 3 shows the trend of three most prevalent ST1 in the study area. The figure reveals that, apart from Gonorrhea cases which show almost imperceptible decline during the period, the profile of Urethritis and Candidiasis is a fluctuation, which altogether tends more towards increase than decline. For future research using this type of data from the sources consulted here, it is suggested that the selected period should not go beyond 1995 for scientific reason of reliability and practical implication of policy formulation and programme implementation. Relationship between Age, Sex, Education, and Reproductive Health Problems Age Specific Incidence of Reproductive Health Problems Observations on age - specific incidence of reproductive health problems as illustrated in figure 4 show a positive correlation (r= 0.952) between age and incidence of health problems. A P- value of 0.000 shows that the relationship is highly significant. In order words, to a very significant extent, the higher the age of adolescents, the higher the incidence of ST1 and other reproductive health problems. However, the fact that cases of STI were observed among 12 and 13 years old adolescents is a disturbing trend, which confirms early exposure to sexual experience among adolescents (Isiugu-Abanihe, 1994; Makinwa-Adebusoye, 1992;) . The particular cases reported among these ages were: Bacterial vaginosis and Trichomoniasis for age 12 and, Genital Ulcer and Genital Warts for age 13. The profile of the different ages on the three most prevalent ST1s shows similarly positive correlations where r values are 0.894, 0.903 and 0.831 respectively for Gonorrhea, Urethritis and Candidiasis. The P value of 0.000 in each case shows that the observed relationship is very significant. Figure 4 reveals that incidence of Gonorrhea span all ages from 14 to 24. In other cases of Urethritis and Candidiasis, age 17 mark the onset of widespread of these ST1s (see figure 4). Variations in Incidence of Health Problems According to Sex and Education of Adolescents Table 1 shows the variations in reproductive health problems according to sex and level of education of adolescents. Variations in each of the socio - economic variables are tested with Chi-square. The result shows that the difference between male and female respondents with respect to incidence and prevalence of the reported health problems is statistically significant. For most of the problems, male adolescents had more than half of cases of Gonorrhea (64.1%), Syphillis (68.2%), Canchroid (, Lymphogranuloma (75.0%) and Urethritis (69.2%),. The only exception were cases of Trichomoniasis, Candidiasis of the genitals and Genital warts, where the female adolescents had a larger proportion of 100, 94.5 and 86.1% in that order (table 1). It can be concluded that the male adolescents featured more prominently in most of the cases of reproductive health problems than their female counterparts. They therefore appear to be major sources of acquisition and medium of transmission of STIs among adolescents in the study area. The profile of different educational groups of adolescents on the various health issues shows that the secondary school adolescents were most affected. For instance 1 out of 2 cases of Syphilis and Chancroid were secondary school students. Furthermore all cases of Scabies were recorded among secondary school adolescents. Further analysis reveals that secondary school students (39.8%) had the largest proportion of Gonorrhea cases, followed by traders (28.6%) and adolescents in the civil service (13.6%). This observation is largely true of cases of Candidiasis and Non-specific Urethritis where secondary school youngsters had 55.0 and 51.9% respectively. Intra-urban Variation in Reproductive Health Problems The observations of intra-urban variations in incidence of reproductive health problems as shown in figure 6 are that: a)
The high density residential areas had the
highest proportion of cases of Gonorrhea (56.8%); Chancroid
(57.1%); Lymphogranuloma Venereum (75.0%);
Trichomoniasis (69.6%) Herpes genitalis (52.2%)
Candidiasis (47.7%) Genital warts (55.6%)
Bacterial vaginosis (53.7%) and Genital Ulcer (63.2%). What can be concluded from the above analysis is that reproductive health problems, particularly cases of ST1s are most acute among adolescents in the high density areas, followed by those in the medium density areas. These areas are inhabited largely by the low and medium classes in the society. Although several studies have established a relationship between incidence of social problems and residential densities (Rutter et al, 1974; Giggs, 1973; Bagley and Jacobson, 1976), the question of what aspect of life in the inner city that predisposes city residents to such problems is a fundamental one. According to Walmsley (1978), while it is not difficult to see how the inner city, with its high density living may foster the spread of infectious and contagious diseases such as whooping cough, it is less clear however to establish a link between inner city living and other social problems like mental illness (and in our case incidence of STIs). Thus the question of the nature of relationship between residential densities and adolescent reproductive health remains a matter of conjecture. It is hypothesized here that, since large cities generally are known to attract migrants, the first port of call for new entrants is the high density areas, where accommodation is relatively cheaper. Although social ties is partially maintained, but new entrants are without adequate support mechanisms that would enable them meet with basic necessities. Consequently, the need for economic survival predisposes them to indulge in various anti-social behaviour. In order words, the need to alleviate acute economic stress that is pronounced in the high density areas make residents to indulge in unsafe health practices with attendant health implications. Again, the concentration of socio-economic activities as markets, motor parks, shops and low-skilled job opportunities like Vehicle Spare parts and Electronic shops as well as Food shops in the high density areas, makes the inner city to be very attractive to new migrants and others who are socio-economically least equipped to compete successfully in the job market, in the housing market and also in the education system. The very nature of life in the high density areas - crowding, high pedestrian flows or high pace of life, high level of interpersonal relationship, in the context of highly congested (space wise) and socio-economically depressed environment - could predispose youngsters who by nature are adventurous and with tendency for high risk behaviours to incidence of STIs The point therefore is that the core areas of our urban centers need greater attention with respect to awareness campaign and promotion of safe sex practices as well as education on reproductive hea Conclusion / Policy Suggestions The range of STIs found among adolescents in the study area is wide, including those linked with increased HIV/AIDS infection such as Chancroid, Syphilis, Trichomoniasis and Bacterial Vaginosis. Data on HIV/AIDS is though officially not available, suffice to say here that, adolescents in this part of the world are not untouched with the scourge of the dreaded disease. Continued suppression of data on this important issue at the official circle should not be seen by policy makers and other health advocates as absence of a health problem which is already assuming an epidemic proportion. The need to make adolescent reproductive health an object of positive policy is premised on the fact that:
The suggestions offered here are aimed at modifying National health programmes such that adolescents reproductive health care should build on the foundation of National Primary Health Care Delivery systems. To this end, a Comprehensive Adolescent Reproductive Health Care is suggested. This will include Counseling about sexuality, reproductive education, screening and treatment for reproductive tract infections. Attention should be given to providing full information on reproductive biology. An important observation is that, in the third world generally and Nigeria in particular, the political commitment to adolescents sexuality and reproductive health is very weak, if at all it exists. The establishment, and reinvigoration, (where rudiments exists) of Youth Development Centres, is suggested. Two types of such centers are envisaged: Continuing education centers and vocational training centers (for out of school adolescents). Their activities will include provision of counseling and reproductive education services. This is because as has been shown in the extended version of this report, (Adeboyejo A. T. and I. P. Onyeonoru (2002) reproductive health care needs of the adolescents in Nigeria are not necessarily hospital or clinic based Family Planning Programmes. The youngsters have associated the clinics and their services with "Families only". Even then service providers in such clinics in most cases do not welcome any unmarried person. There is the need for strong adolescent sexuality and reproductive health advocates, similar to Women's Health Organisations such as International Women's Health Coalition. Such advocates must show a good understanding of adolescent sexuality and reproductive problems and must be able to provide counseling and education services. There is the need for the government and general public to face the facts of adolescent sexuality and reproductive health. Consequently a National Commission on adolescent sexual health be set up. The body should come up with concensus statements about adolescent sexual health, draw up culture specific policies and pragramatic intervention programmes. We are aware of the possible public skepticism and antagonism to the provision of sexuality and reproductive health education to unmarried adolescents. Nevertheless, it is possible to develop appropriate programmes and activities with the support and cooperation of Family/Life Planning Associations and Non-Governmental Organisations. References
Copyright 2003 - Union for African Population Studies The following images related to this document are available:Photo images[ep03006t1.jpg] [ep03006f3.jpg] [ep03006f1.jpg] [ep03006f5.jpg] [ep03006f4.jpg] [ep03006f2.jpg] [ep03006f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}