 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 18, No. 2, Oct 2003, pp. 1-26 Rural-Urban Migration and Its Effects on Infant and Child Mortality in Ghana Adansi A. Amankwaa1, Al Bavon2, Paul T. Nkansah3 1Albany State University USA, 2 University of North Texas USA, 3 Florida A & M University USA Code Number: ep03008 ABSTRACT This paper examines the socioeconomic characteristics of rural-urban migrants, child mortality and maternity child health care in Ghana. Data from the 1988 Ghana Demographic and Health Survey shows that infant mortality is lower among rural-urban migrants compared to rural non-migrants. Proportional hazards model estimates reveal that the survival chances of children of rural-urban migration persist after controlling for socioeconomic characteristics. However, these advantages disappear after demographic variables are included in the model in spite of the proximity and accessibility to medical facilities enjoyed by the migrants. This finding suggests that socioeconomic and demographic characteristics of migrants could be an important determinant of the survival of children of rural-urban migrants. RÉSUMÉ Cet article examine les caractéristiques socio-économiques des migrants ruraux-urbains, la mortalité infantile et les soins de santé infantile dans les maternités au Ghana. Les données de l'Enquête démographique et de Santé du Ghana de 1988 ont montré que la mortalité infantile est plus faible parmi les migrants ruraux-urbains que parmi les non-migrants ruraux. Des estimations du modèle aléatoire (Proportional hazards Model) ont montré que les chances de survie des enfants issus de l'immigration rurale-urbaine augmentent si on prend en compte les caractéristiques socio-économiques. Cependant, quand on fait intervenir les variables démographiques dans ce modèle, ces avantages disparaissent malgré la proximité et l'accessibilité des centres médicaux. Ce résultat prouve que les caractéristiques socio-économiques et démographiques des migrants constituent un déterminant important de la survie des enfants issus des migrants ruraux-urbains. INTRODUCTION Much of the academic research on migration in West Africa has been focused either on spatial and labour movements (Zacharial and Conde, 1981; Caldwell, 1968) or infant mortality and socioeconomic factors (UN, 1982). Until recently, most studies of migration in sub-Saharan Africa (SSA) were concerned with selectivity, determinants and consequences of human movement (Caldwell, 1986; UN 1973, 1991; Gaisie, 1975; Findley, 1997; Makinwa-Adebusoye, 1990; Chant and Radcliffe, 1992; Chant, 1992). Of particular concern was the strong positive relationship between migration and selectivity; this relationship is one that is fully documented in the literature. Although few studies have underscored the importance of infant survival in migration research (Brokerhoff, 1990), progress has been hampered by the recent reversals in the economies of sub-Saharan countries. Thus understanding this changes is a prerequisite for understanding the confluence of migration and infant and child survival. This notion is evident in the National Academy of Sciences studies in SSA countries indicating that economic reversals erode gains in mortality (National Research Council, 1993). Given the striking trend in the economic reversal in SSA during the 1970s and 1980s (UN, 1982), there is the need to refocus research on migration and its beneficial effect, particularly on infant and child survival. Because rural-urban migration has been found to benefit infants and children (Brokerhoff, 1990), this relationship needs to be reexamined within the context of the recent economic crises. In fact, when we deal with health and survival, we tend to assume that movement from rural to urban areas is beneficial because urban areas are favoured in terms of services, as rural-urban mortality differentials tend to show urban advantages. We can only come to this conclusion if we ignore the significant contribution migration and economic growth make to urbanization. Given that migration involves considerable dislocation and disruption, there is a strong possibility that it has negative effects on health and subsequently on infant and child survival, particularly during times of economic crises. Indeed, research on migration and infant mortality is an important, yet much neglected, topic in studies of the effects of migration on infant and child survival. The objective of this study is to examine the influence of migration on the relative risks of infant and child survival by controlling for selectivity and adaptation characteristics. The principal objectives are to investigate how selectivity and adaptation characteristics affect infant and child survival of rural and urban migrants within the context of Ghana economic crisis1. Migration might impact on health negatively because it is such a disruptive experience. However, it is possible that this disruptive experience is minimized because migrants are such a selective group in terms of motivation who are able to adapt after a while and also because most migrants move to destinations with better health services. This implies that to see the impact of migration induced disruption on child health, we have to control for the selective characteristics of migrants, the time they have had to adapt and the differences in access to infrastructure that exists between origin and destination areas. Theoretical ArgumentsTheories attempting to explain infant and child survival in sub-Saharan Africa can be divided into three broad categories: disruption, selection and environmental perspectives. According to disruption theory, migration disrupts jobs, family and community attachments. In the absence of economic crises, migrations from rural to urban areas can enhance survival by introducing the migrant to new job opportunities, community, and better health services. Previous studies indicate that people move to cities because of perceived benefits such as better education, income, and health (Caldwell, 1986 ; Brockerhoff, 1990). The growth of cities in developing countries due to human movements is based on this premise. Disruption due to migration has a positive effect on individuals’ income-generation ability and hence on their access to adequate diet, shelter, and health care services that can promote healthy life. Because migration represents a major disruption and requires a significant period of adaptation, life style and health related behaviour may be affected by the migration process itself. Factors usually associated with disruption are education, occupation and migration itself. Indeed, disruptions during the time of economic crises tends to exacerbate the beneficial effects of health because of the migrant’s exposure to harsh economic realities. One would expect then that the level of disruptions on infant and child mortality, in the face of economic crises, should be affected negatively.The second type of explanation relates migration to selection. Selection theory argues that occupation, education, and wealth explains a person’s propensity to migrate (Caldwell, 1986). Rural to urban migration is related to the concept of selectivity, which in turn is beneficial to infant survival. Underlying this principle of infant survival is the recognition that rural-to-urban migration consists of people who are, more often than not, well educated, possess better occupational skills, have considerable wealth, and are mostly young compared to nonmigrants. As a result, rural-urban migrants have greater ability to adapt to their new environment. In the case of infant survival, selectivity theory suggests that as migrants adapt to their environment, health status of infants and children depend largely on access to health care services and technology. Because selectivity theory emphasizes the characteristics of the migrants, it implies that in those societies where there are economic opportunities, the beneficial effects of selection will be enhanced. A critical idea related to selectivity is the notion of homogeneity of rural populations, and this needs to be taken into account for any investigation of the phenomena. Rural population in Ghana is essentially homogeneous in terms of life style, educational level, occupation (predominantly agriculture), high fertility and little access to technology. Given these characteristics, it is expected that selectivity may be less important than urban adaptation in the relationship between migration and infant mortality. The third explanation, which is perhaps one of the most popular explanations for infant and child survival, has been that of migrant adaptation or environmental approach. The term migrant adaptation implies contact with urban environment through social interaction and increased exposure to new ideas may lead to changes in attitudes, life style, and motivations. According to this view, migrants in an urban setting may be poised to adapt to urban living conditions by changing their behaviour. Such changes are deemed necessary for the enhancement of the survival of children. In fact, previous studies suggest that maternal child-care behaviour, the quality of household facilities and fertility (such as birth interval and birth order) is among the most important types of adaptation that are associated with infant mortality. For example, there is evidence to suggest that care of women during pregnancy has a positive effect on neonatal mortality (Hecht and Cutright, 1979; Ahmad, Eberstein and Sly, 1991; Silverman, 1970). Yet, in developing countries where most births take place at home (Omran and Standley, 1976) with little understanding of disease transmission among infants (Garenne and van de Walle, 1985), exposure to risk is high. Toilet facilities and type of drinking water are used as control variables to account for risk of mortality. Because unsanitary toilet facilities and drinking water are expected to be negatively associated with survival, good drinking water and sanitary toilet facilities are assumed to increase the likelihood of infant and child survival. One manifestation of migration would be to enhance survival, particularly if the movement is from rural to urban. Environmental theory stresses not only adaptation to urban living conditions by changes in maternal behaviour but also in terms of longer birth intervals and birth order. These necessities may stem from the physical or social environment (Graves, 1991; Durham, 1992). Some sort of maternal behaviour, for example, is necessary and because of the differences in social environment to which migrants must adapt. In urban areas where population density is high, small families would be valued. Therefore, demographic factors will be added to the analysis to complete the assessment of the adaptation theory. Previous ResearchMuch of the evidence for migration perspective in sub-Saharan Africa (SSA) consists of examples of determinants and consequences. Most findings on internal migration and urbanization in Ghana suggest that thousands of people move from one place to another. For example, Opoku (1990) examined migration in Ghana and showed that 18% of the population in all the regions in 1982 were in-migrants compared to 36% in Accra. Caldwell (1986) using “push-pull model” to examine migration in Ghana, found that 14% were urban-rural migrants while 11% were rural-urban migrants. His analysis shows that education, gender and age play an important role in migration. Attending school in a town or city in Ghana tends to be very critical in rural-urban migration, rather than education per se. In Ghana, most of the secondary and post-secondary schools are located in cities and towns, as such the desire to pursue a higher education implies movement, not because they have received schooling in rural areas. Indeed, people may move to the city or town simply to attend school. Thus, education is associated with the predisposition to migrate. Evidence suggests support for the determinants of rural-urban migration perspective, but the impact of migration on infant and child mortality is still not clear. Previous studies suggest that demographic factors are important determinants of infant and child survival in developing countries observed that in traditional societies, demographic factors have more impact than the socioeconomic factors. However, they concluded that demographic factors are important during infancy and childhood, but social factors such as parent’s education appear to be important predictors of infant mortality risks. Furthermore, early studies of migration in Ghana suggest that people who move from one place to another are younger, on average, than nonmigrants (Caldwell, 1986). For example, Caldwell’s analysis suggests that most rural-urban migrants are young, usually 15 and 34 year-olds. Although the study contains useful explanation on migration patterns in Ghana, the hypothesis is yet to be tested empirically on infant and child survival. One reason for that is the lack of an adequate conceptual framework, which the present study supplies. Most of the past work has focused on gaining an understanding of the role selectivity plays in the migration process. Based on historical experience of migration in Europe and elsewhere, this perspective asserts that selectivity plays a major role in the process of migration. In fact, selection effects like a set of pre-migration factors such as occupation, education and wealth have been used as explanatory factors for a person’s propensity to migrate. Not only are SES factors related to the predisposition to migrate, but may be more likely to lower infant and child mortality risks. Thus, an observed association between migrants’ status and survival of children may, in fact, be due to SES characteristics. The implications of selective migration for survival have received more attention than the negative effects of disruption on relative risks of childhood mortality. Previous research, for example, shows that a woman’s migration has a strong negative association with her children’s risk of death. Brockerhoff (1990), Farah and Preston (1985) and Mensch, Lentzner, and Preston (1985) suggest four factors that may help explain this relationship. First, it is argued that positive selection of migrants from population at origin such as education, wealth, income and age, among others, are important traits in enhancing survival of their children. Second, differences in community characteristics in addition to disease environment between origin and destination areas are strongly related to the health status of the child. The presence of survival related facilities in urban areas suggest that migrant children have better chances of surviving than those residing in rural areas. Third, it has also been argued that difficulties faced by migrants in adapting to their new environment may also affect the survival status of their children. Finally, the survival status of the children of migrants is found to be associated with the disruption caused by the move itself. This means that to see the impact of migration induced disruption on child health, we have to control for the selective character of migrants. The major thrust of this thesis is that the predisposition to migrate reflects not only the individual’s SES and demographic characteristics but also, infant and child mortality may vary across migrant groups. Although migration tends to elevate mortality in the transition phase, due to disruption, migrant women never achieve child mortality rates as urban natives. Brokerhoff (1990), for example, shows that children of urban migrants experienced higher mortality risks than urban nonmigrants before they attain the age of 5. The study also shows that the survival chances are higher among rural-urban migrants than rural nonmigrants. His study gives further support for understanding variations in mortality and hence the relative risk of dying within migrant and nonmigrant groups, but does not reflect the characteristics of infants and children during a period of economic instability. Furthermore, there are other measures of migration that are very important that we cannot estimate given the form of our data. For example, the GDHS does not contain information on frequency of moves, date and place of birth, or reasons for moving. In spite of the limitations, previous place of residence, usual place of residence and type of place of residence have been frequently used to measure migration status (Caldwell, 1986; du Toit, 1990). Our measurement of migration status in this study is limited to usual and previous place of residence, since previous place of residence, usual place of residence, and type of place of residence have been considered to be a general indicator of migrants’ status. Other studies (Goldstein and Goldstein, 1981; United Nations, 1973, 1991) find that place of residence affects childhood mortality. Moreover, and perhaps, very important for health and survival reasons, migration may help to reduce mortality risks (Brockerhoff, 1990). While most of these studies give us an understanding of the wider perspective on the link between migration and childhood mortality, there is still the need to look closely at particular countries in great detail for us to fully understand how migration impacts on children. Certainly, migration plays a role in child survival, and these studies have found evidence of both positive and negative impacts of mortality risks for children. The process of migration may directly improve child survival, even without the positive aspects of selection and adaptation, if the move involves relocating in a good climatic region or if there is equitable distribution of health services to all residents. The general lack of a health care infrastructure in most parts of the countryside suggests that there is a continued reliance on traditional methods of infant care. Further, social services such as electricity, pipe borne water, and sanitation are unavailable to a large segment of rural residents but are available to most urban dwellers. Perhaps the most important factor, Ghana’s economic crises may be particularly important in exposing children to a large variety of potential infections because of the general lack of health care services and medicine, inadequate nutrition, and poor environmental hygiene. Such situation was more prevalent in the urban than in rural areas during Ghana’s economic reversals. For example, among the rural population, people still prefer to consult with native herbalists and healers when they are ill. The rationale for this is that diagnosis and remedies prescribed by these traditional healers are compatible with cultural beliefs (Ofosu, 1988). Typically, rural residents are more likely to seek the help of herbalists and native healers than urban dwellers. However, since there were also crises in the health care services in the cities and towns, urban residents constitute a high risk group. Because urban residents depend mostly on modern health care services, their continuous exposure to inadequate health care service increases the likelihood of infection and hence survival. Again, mortality risks of infant and children of rural-urban migrants may be higher than urban natives and urban-rural migrants because of their inability to meet the high cost of health care. Urban-rural. The term “urban” as used in this paper refers to settlements in which there are 5,000 or more residents (UN, 1994). This is the official definition used in the 1960, 1970 and 1984 censuses in Ghana. Most urbanites, as in most African countries, live in towns in which an “urban” way of life or amenities are limited and in some instances not available. Between urban and rural settlements lies a richly variegated social gamma of rural and urban patterns, in which a town may sometimes have rural characteristics. Therefore, survival chances of infants and children are expected to vary greatly, given the heterogeneity of Ghana’s cities and towns, in terms of population and living conditions. Our study employs 1988 Ghana Demographic and Health Survey (GDHS) and Cox proportional models, which has been tested to be robust, to:
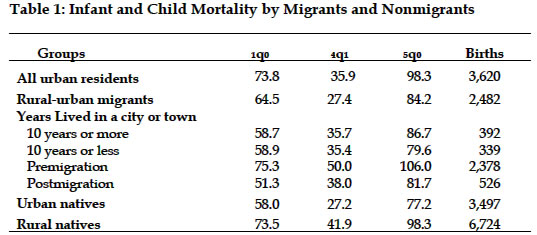
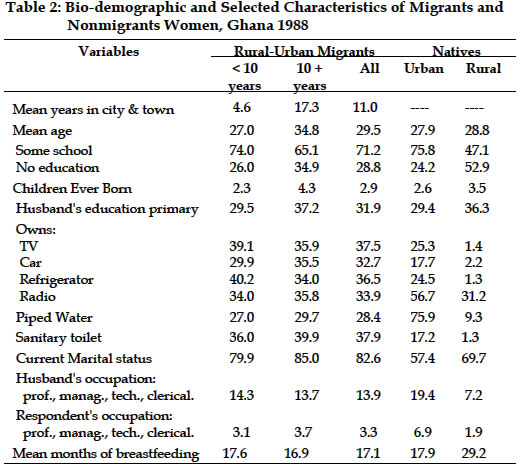
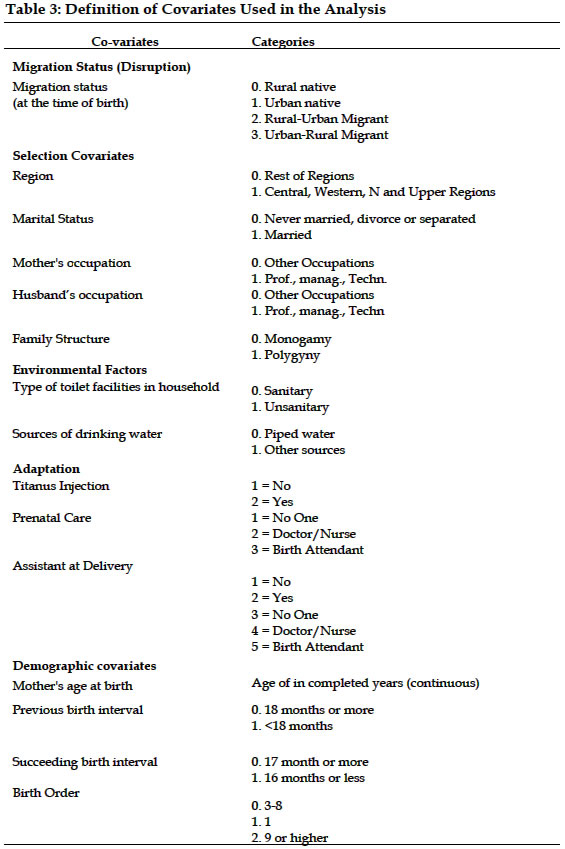
DataThe data for this paper is part of a much larger study designed to describe and to understand the social and demographic aspects of developing countries. Briefly, the Demographic and Health Survey provide detailed information on maternal and child health, mortality, birth histories and characteristics of eligible women ages 15-49 and their spouses. This study converts maternal database to birth database from GDHS 1988 to examine infant and child mortality disparities among migrants, rural natives and urban natives. A sample of 12,933 births is used in the analysis. By using births rather than maternal data, one not only can examine the importance of the relative risk of rural-urban mortality disparities, but also analyze differences in outcomes resulting from rural-urban migration. Given the social structure of Ghana, infants live with their mothers, at least, for the first four years of life. The norms and values in Ghana typically demand that the woman take care of the newly born infant, rather than the man or any other member of the extended family. Child fostering is not a viable option -- in Africa with children under age 5. The role of a mother thus has a community-wide meaning. This is because in a typical Ghanaian tradition nurturing is the sole responsibility of the mother. Yet, despite these expectations, many children are fostered after the age of 4 or older. In order to gain a better idea of how migration affects mortality, we examine infant and child mortality among migrants and nonmigrants. Table 1 presents infant mortality rates and numbers of births by migrant and non-migrant groups. The concept rural-urban migrant refers to urban migrants whose previous residence is village or countryside. Migrants who lived in city or town for less than 10 years are classified as recent migrants. Table 1 shows that mortality rates before age 5 among children of rural-urban migrants is slightly higher than among urban natives (84.2 and 77.2 per 1,000, respectively) and higher for longtime migrants than for natives. There are at least two distinct mortality patterns operating in urban areas in Ghana. The estimated rates are affected by age heaping at 12 months. This problem is partly corrected by using age at death of 15 months for infants as a cut-off point for infants and 65 months for children. There is evidence to suggest that rural-urban migration reduces infant and child mortality. Children of migrants who recently moved to the city or town experience a mortality rate between the ages of 1 and 5 of 82 per 1,000, compared with 106 for children born before migration as shown in Table 1. This decline confirms the general mortality decline in Ghana. While rates for each group are relatively lower, the difference between recent and long-term migrants is about the same. Thus, mortality rate among children of rural-urban migrants is lower than among rural nonmigrants, especially between the ages of 1 and 5 (Table 1). The observable difference can be attributed in part to the migrant selection. For instance, the mortality rate of 87 per 1,000 of migrant children between the ages of 1 and 5 is lower than that of rural native children (98 per 1,000). Yet, while mortality differentials exist between rural and urban natives, these differences are less apparent for both short and long term migrants, as shown in Table 1. For example, between first and fourth year (4q1) mortality rates are about the same (36 and 35 per 1,000)2. Evidence of Migrant Selectivity and Adaptation CharacteristicsTable 2 presents evidence of socioeconomic and demographic characteristics of migrants and nonmigrants characteristics, which have been found to be associated with selection and adaptation of migrants to urban environment. The results in Table 2 show that rural to urban migrants appear to have received some education; 71.2% of migrants, compared with 47% of rural nonmigrants, had some education (primary, middle, secondary or higher). The relevance of education in the determination of mortality levels has been widely discussed in the literature (Caldwell, 1986, 1990). It has been assumed that, at least at the individual level, education is a source of valuable wealth of knowledge at the disposition of the mother to take care of the health needs of the infant and/or child. In addition, it is believed that higher education promotes awareness and use of available health care services. In the recent past, Caldwell (1986) argued that educated mothers exercise more authority within the extended family and are more likely to seek modern health-care for infants and children than follow traditional norms and practices. Educated mothers may adopt superior child-care practices. On the other hand, women who are less educated may be more likely to adopt modern child-care practices associated with higher mortality. In what follows, we investigate whether infant and child mortality is lower among migrants than nonmigrants. It is important to note that the measure of migrant and nonmigrant include migration status, early urban exposure and socioeconomic characteristics. Although urban residents may have survival advantage over rural residents, rural-urban migrants may be at a disadvantage, in spite of the expected benefits to be derived from health services (for example, their proximity to doctors, nurses and health services). The main reason for this is because urban residents and migrants were greatly affected by the economic difficulties than rural residents. Method and Explanatory Variables In our multivariate analysis, the variable of interest is migration status and its effect on mortality. Migration status is an inclusive measure of child and maternal characteristics specifically constructed to take into account selection effects. Because rural-urban migration is a general indicator of mother’s movement and the number of years lived in an urban area, there is concern about mortality risk differentials of children born in rural areas and exposed to rural risk 5 years, to urban risks, compared to children with mixed rural-urban exposure. In this study, we analyzed migration status as follows: for children of migrants born before their mother’s migration, the period of exposure to mortality is attributed to the previous settlement type. Urban-rural residence is modeled as a time dependent covariate to distinguish the effects of urban and rural exposure on migrants’ child mortality. We then create four categories of migrant’s status: urban natives, rural natives, rural-urban-migrants, and urban-rural migrants. We demarcate those who are rural natives (i.e., nonmigrants) as the reference category. Table 3 presents a list of the variables and their measures. The four categories allow for the assessment of the important aspects of rural-urban migrants, urban native and rural natives. In this study, four sets of factors expected to influence mortality, as described earlier, include migrants status, socioeconomic characteristics, environment (type of drinking water, toilet facilities within household) and demographic characteristics. As noted, the variables include measures of selection and adaptation. Individual socioeconomic characteristics and fertility related variables contribute to measures of selection and adaptation. The explanatory variables are chosen to capture the effects of selection and adaptation, within the context of migration, on infant and child mortality. First, because of the presumed advantages enjoyed by migrants, children of rural-urban migrants are more likely to survive than nonmigrants. Residential background is one of the important measures of selection and adaptation. The use of residential background is predicated on the assumption that earlier exposure to urban living may facilitate migrant selection and quick adaptation to urban environment than first time rural-urban migrants. Previous exposure to urban way of life is a reflection of an individual’s ability to utilize urban services and institutions (i.e., in terms of location and use of hospitals, clinics, etc.), as well as changes in behaviour concerning food preparation and personal hygiene. These factors are thought to enhance infant and child survival. We measured selectivity and adaptation using respondents’ socioeconomic characteristics. All things being equal, husband or mother’s education has been found to reduce the risk of infant mortality. For example, the infant mortality rate of children of highly educated mothers is about 68% lower than that of uneducated mothers. Thus, the mother’s level of education indicates greater access to modern information, which in turn facilitates adaptation to urban environment. Illiteracy also denotes, in most instances, general lack of crucial information that could create problems of urban adjustments and could negatively affect the quality of child care. Polygyny is recognized to be correlated with infant and child mortality, but it has important ramifications on migration. Polygyny as a marriage pattern is considered to have developed within populations as a positive adaptation to environmental constraints by enhancing maternal and child health through postpartum sexual abstinence, prolonged breastfeeding, and longer birth intervals between pregnancies. One important role polygyny plays in traditional Ghanaian social structure is longer birth spacing, which has been found to reduce fertility at the individual level (Pebley and Mbugua, 1989). Both Preston (1980, 1985), and Santow and Bracher (1984) argue that there is a link between lower fertility and mortality. Moreover, polygyny is not only more prevalent in rural than in urban areas, it also tends to encourage migration. The importance of environmental factors such as piped water, sanitary toilet facilities (flushed toilets) on infant and child survival have been discussed in demographic literature. Availability of good drinking water and access to clear toilet facilities within the household is vital in reducing water borne diseases and other infections from unsanitary toilet conditions. Increased access to piped water contributes to mortality decline in many developing countries (Casterline, Cooksey and Ismail, 1980; DaVanzo and Habicht, 1986). Finally, the demographic control variables are age at first birth, preceding birth interval, and birth order. Age at first birth is measured in single years ranging from 18 to 49. Preceding birth interval is a dichotomous dummy variable, which is measured as less than 18 months and 18 months or more. Preceding birth interval is measured as less than 18 months and 18 months or more. Birth order is categorized into three groups: 1-2, 3-8, and 9 or higher. Analytic StrategyThe proportional hazards model, developed by Cox (1972), allows one to estimate the effects of individual characteristics on survival time without having to assume a specific parametric form for the distribution of time until the event occurs. This model has been used to study mortality survival analysis of husband and wife (Brockerhoff, 1990; Smith and Zick, 1994) and recidivism (Barton and Turnbull, 1981; Linster and Patterson, 1987; Rhodes, 1986). In the study, we examine the impact of several explanatory variables on infant mortality in Ghana using Cox proportional-hazard models. One reason for including explanatory variables in a survival model is simply to make predictions that are more accurate; the existing literature suggests quite clearly that individual characteristics, previous experiences, and environmental factors help to predict infant mortality (Brockerhoff, 1990; Mensch, Lentzner, Preston, 1985). Table 3 presents the various explanatory variables used in this analysis; the variables relate to migration selection, adaptation and environmental setting and are expected to have an impact on infant mortality. First, is the positional hypothesis of a link between rural-urban migration and infant life chances; urban residence confers survival advantages because of proximity to health related infrastructure, housing and better nutrition. This hypothesis implies that infant mortality is lower among children of women who reside in the city or a town than among rural nonmigrants. This selection hypothesis would suggest that the children of migrant women are related to migrant selection and adaptation, and thus, are more likely to experience lower infant mortality than are nonmigrants because of other characteristics associated with differential mortality. This hypothesis requires that determinants of rural-urban migrants be held constant when the effect of migration status on infant or child survival is examined. Any infant mortality disadvantage of urban migrants relative to urban nonmigrants should be obvious when selection and adaptation characteristics are held constant. As such, it might be expected that socioeconomic and demographic variables included in the models should account for much of the infant and child mortality differential among rural and urban natives. Thus, the study examines the general relationship between migration status and infant/child mortality in Ghana, and the extent to which selectivity may account for this association, and the role behavioural characteristics play as linkages between these constructs. For an individual with a (row) vector of demographic and socioeconomic characteristics, the proportional hazard model assumes a hazard rate of the form: where ho(t) is a completely unspecified baseline hazard function. Thus, the model assumes that the hazard functions of any individuals differ only by a factor of proportionality, but puts no further restrictions on these hazard functions. Given these assumptions, advantages and limitations of the proportional-hazard models developed by Cox (1972), which have been clearly documented in several studies (Chung, Schmidt and Witte, 1991) the model is specified as: where ln[h(t)] is the risk of death; ln(h) is the unspecified baseline hazard; Mig symbolizes native/migration status at the time of the survey. PriorSE denotes a set of socio-economic characteristics of migrants prior to the time of migration and are thought to be causally associated with infant mortality; post-migration characteristics are said to be related to socioeconomic and fertility-related variables which are also thought to be causally related to infant and child mortality, are symbolically represented by PostSE and Fert.
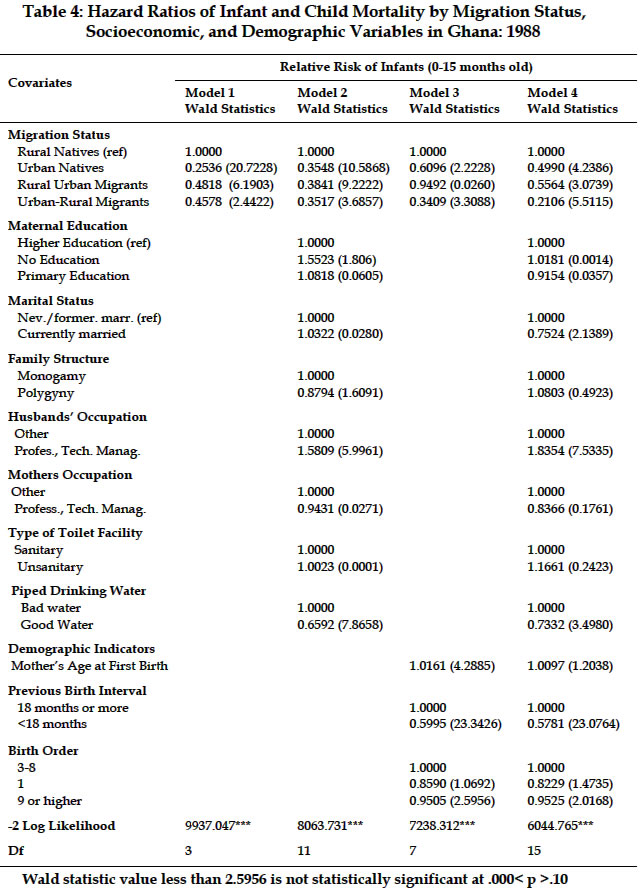
The vectors The dependent variables are measures of death during the first year (infant mortality, i.e., 0q1) or first four years (child mortality, i.e., 0q4). Death indicates the time from birth until death measured in months. Second, the censoring variable equals 1 if the infant/child died during the 15 months or 65 months and equal zero otherwise. The analysis is a series of Cox proportional hazard regression equations including in sequence migration status, socioeconomic characteristics and demographic factors. This will allow for an assessment of the direction and magnitude of the pattern of infant and child mortality by migration status, including the extent to which selection and adaptation help to account for variability in infant or child mortality. RESULTSPredicting the Relative Risks of MortalityIn keeping with the causal nature of the conceptual model, the analysis examines the relative effects of migration status on infant or child mortality holding constant the effects of all other variables in the model (i.e., socioeconomic and demographic characteristics). Results of estimating proportional hazard models are given in Table
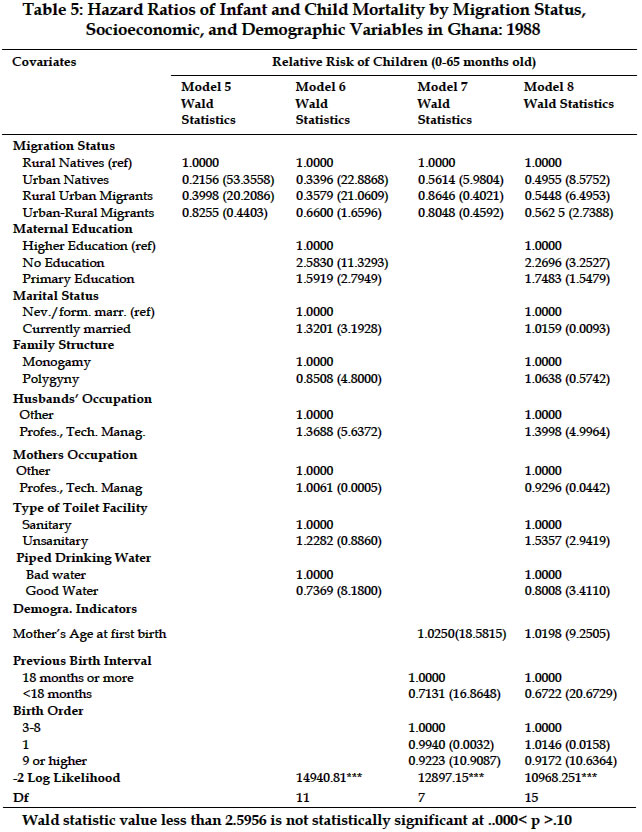
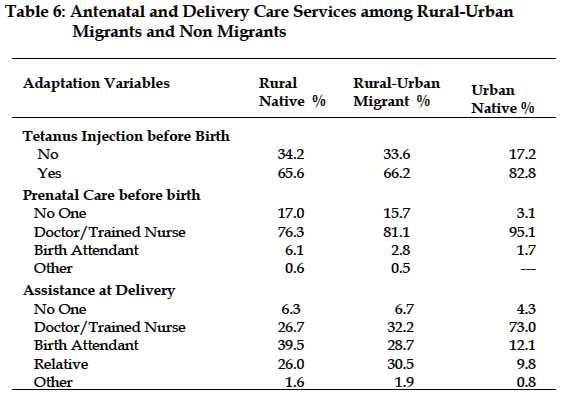
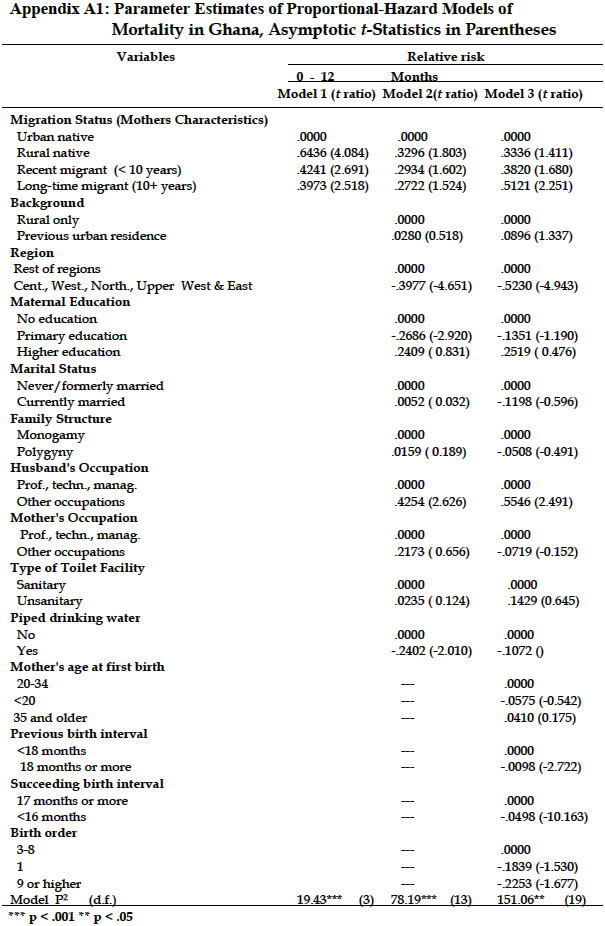
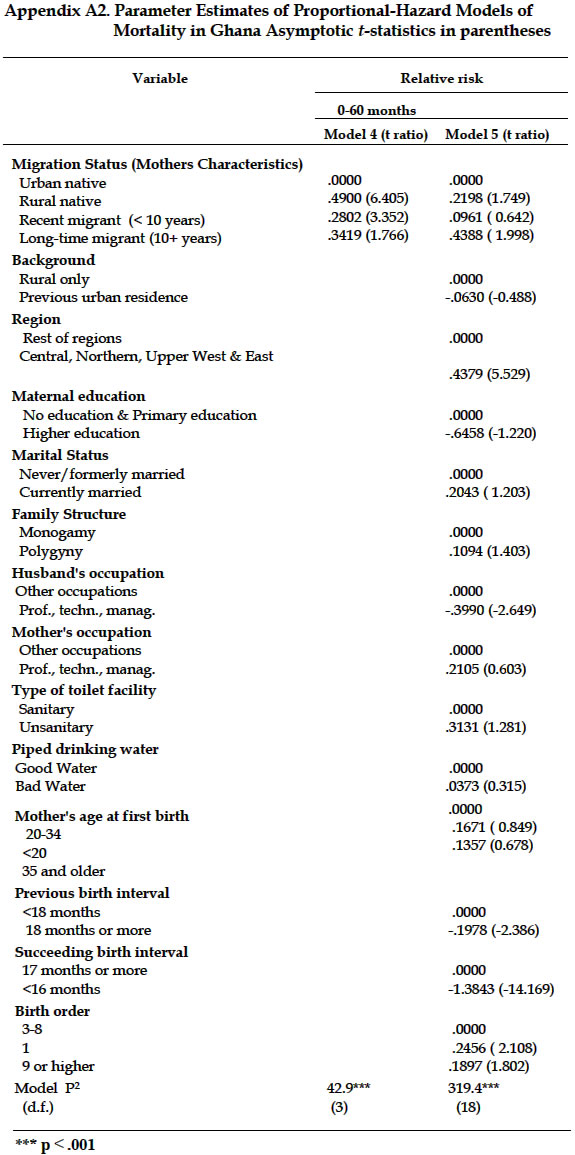
4 for the analysis of GDHS. Models 1 and 4 display the relative risks of infant and child mortality. The asymptotic t ratio for each coefficient - the estimated parameter divided by its asymptotic standard error - is also presented. These t ratios are asymptotically distributed as standard normal, under the null hypothesis that the corresponding coefficient equals zero. In interpreting these results, note that a positive element in the vectors Child-level measures refer to the unique set of child and maternal characteristics that affect the risks of death. To test the impact of selectivity on the association between children’s migration status and mortality risks, we modeled the effects of migration status, socioeconomic selectivity variables and demographic controls on the risks of mortality. Infant mortality and MigrationThe results in Model 1 display the baseline migration status and infant mortality. With no controlled variables, the risks of infant and child mortality are lower among urban natives than among rural natives, rural-urban migrants, and urban-rural migrants. Specifically the risk of mortality is higher among rural natives than among rural-urban and urban-rural migrants. However, the risk of infant mortality is lower among rural-urban migrants than urban-rural migrants. The hypotheses of interest are tested in models 2, 3, and 4. For infant mortality, these models demonstrate the impact of the socioeconomic, selectivity, and demographic factors on the association between mortality and migration status. Wald statistic value less than 2.5956 is not statistically significant at .000< p >.10 When we included socioeconomic characteristics, we find a slight reduction in the magnitude of the coefficients, but a strong migration status effect remains. These findings suggest that migration status is an important predictor of infant and child survival controlling for education, occupation, and household facilities. The analysis shows consistent effect of survival advantage among urban natives and rural-urban migrants compared to rural natives (the omitted category). For example, compared to those who are urban natives, those whose mothers are rural natives exhibit 65% lower risks of dying, those who are rural-urban migrants show 62% lower risk while urban-rural migrants exhibit 65% lower risk (Model 2). In model 3, we introduce demographic indicators without socioeconomic variables. With the inclusion of demographic factors without socioeconomic covariates, the estimated coefficients of migration status appear to have reduced influence on mortality risk (compared with model 2). However, the estimated coefficients of age at first birth, birth order, and birth interval are statistically significant from zero. These demographic variables do appear to affect mortality risks. For example, the age at first birth has a positive coefficient (β=.016), implying that there is approximately a 2% increase in hazard for each unit increase in age at first birth. Model 4 includes the full set of independent variables. Once again, the migration status effect is consistent with expectations but also produces dramatic results from those of Model 3. For example, infants whose mothers are urban natives have reduced their risk function of death by 50%, rural-urban migrants by 46%, and urban-rural migrants by 79%. Child Mortality and MigrationTable 5 provides results for the relative risk of child survival and migration status. We estimated four models using similar controls and format as with infants and migration status. As table 5 indicates, among children of urban natives, rural-urban migrants, and urban-rural migrants, the hazards are lowered by 50%, 46%, and 44% respectively, relative to rural natives (Model 8). Furthermore, the inclusion of demographic indicators in Model 8 has statistically reduced the effect of migration status on child mortality risks. The demographic factors produced mixed evidence. Birth interval and birth order are the two variables that provide the strongest evidence. Longer birth intervals decrease the risks of infant and child mortality; the effect is stronge when the birth interval, for example, is long than when it is short. This finding provides support to the idea that demographic factors, such as birth interval and age, are also responsible for the association between migration status and child mortality. Whereas the mortality effects of birth interval and birth order are similar, the mortality effects differ by mother’s age at first birth. We consider the age of mother at first birth to be a risk factor. It appears that the mother’s age at first birth has a significant effect on risk of child mortality. There is evidence, however, that as the age at first birth increases, her infant’s risk of mortality decreases, all else being equal. Wald statistic value less than 2.5956 is not statistically significant at ..000< p >.10 Adaptive Mechanism: Antenatal, Health Care Delivery Services, and MigrationFinally, the results in Table 6 show the distribution of antenatal and delivery care services among rural-urban migrants and non-migrants. The data indicate that urban natives and rural-urban migrants take better advantage of the health care services than rural natives. In particular, 82.8% of urban natives received tetanus injection before birth compared to 66.2% among rural-urban migrants and 65.6% among rural natives. In addition, rural-urban and urban natives are more likely to see a doctor or trained nurse for prenatal or delivery care compared to rural natives. CONCLUSIONS AND DISCUSSIONSIn this paper, we used Cox proportional hazard model to explore the relative effects of migration status on infant and child survival in Ghana from 1974 to 1988. The results show that migration is associated with infant and child mortality risks. Differences in infant mortality in terms of migration status persisted even after socioeconomic characteristics are held constant. It is possible that rural-urban migrants exhibit distinct behaviours such as maintaining sanitary conditions, good nutrition, utilizing health care facilities and norms that are consistent with urban living arrangements. The results also uncovered evidence of slightly lower risk of infant and child mortality among urban-rural migrant children than infants and children of non-migrants (rural natives). This finding also suggests that the risks of dying are less pronounced among children of mothers who have resided in a city or town for more than 10 years than among their short-term peers (see Appendix A1 and A2). A more important explanation for the difference in mortality risks during late 1970s and 1980s was that short term migrants are more likely to face the crunch of the economic crises compared to long term rural-urban migrants. However, the results show small mortality risk differential between rural-urban migrants and urban natives. This small mortality difference may be attributed to the overall economic crises in Ghana where urban residents and rural-urban migrants may have similar experience with urban natives having a small adaptive advantage over the latter. While it is shown that selection factors have come to play an important role in shaping survival, the survival advantages enjoyed by the children of migrants tend to disappear when age of the mother, previous and succeeding birth intervals, and birth orders are held constant. These findings underscore the importance of adaptation factors in order to understand which factors affect infant and child health outcomes during the period of economic crises. In view of the situation, policy should seek to improve the standard of living by providing employment opportunities for women in the modern sector. However, more work is needed to examine the negative effects of economic crises on the adaptive mechanisms of rural-urban migrants. In conclusion, policy makers must therefore realize the need for policies that address in a responsible manner the presence of rural-urban migrants in urban area. At the same time policymakers can assume their commitment to developing and improving health care services in the rural areas. Future ResearchIndeed, our understanding of the effects of socio-economic and demographic factors on infant and child mortality is far from complete. The behavioural link between rural and urban place of residence, and individual socioeconomic and fertility related characteristics of pre and post-migration behaviour, and the effects on infant and child mortality, are issues that remain to be addressed before any firm conclusions may be drawn. Notes
REFERENCES
ACKNOWLEDGEMENTSWe are grateful to the Center for the Study of Population, Florida State University for providing the funds for the purchase of the data from Demographic and Health Surveys, MD and Kermit Rose for his help in data extraction. The views expressed in this paper are mine and should not be attributed to the Government of Ghana. We benefited from the comments of Ike Eberstein, professor of Sociology, Florida State University, Tallahassee, FL, Kofi D. Benefo, Lehman College NY and an anonymous reviewer. The usual disclaimer applies. Copyright 2003 - Union for African Population StudiesThe following images related to this document are available:Photo images[ep03008a2.jpg] [ep03008t6.jpg] [ep03008t1.jpg] [ep03008t2.jpg] [ep03008t3.jpg] [ep03008t5.jpg] [ep03008a1.jpg] [ep03008t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}