 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 18, No. 2, Oct 2003, pp. 69-90 Contraceptive Use Dynamics among Migrant Women in Kenya Charles Ochola Omondi1, E. H. O Ayiemba2 1Maseno University, Kenya, 2University of Nairobi, Kenya Code Number: ep03011 ABSTRACT This paper investigates the relationships between migration and the determinants of contraceptive use in Kenya based on the 1988/1989 Kenya Demographic and Health Survey (KDHS). The KDHS collected detailed information on pregnancies, contraceptive use, marriage, employment, places of residences and how long one has lived in these places of residences. The paper examines whether the contraceptive use dynamics of women who migrate characteristically differ from that of non-migrants in Kenya. The principal hypothesis of the paper is that women who migrate comprise a group who acts rationally to maximise their other lifetime aspirations at the expense of their reproductive roles. The study further assumes that through the influence of fertility process by migration characteristics, contraceptive use is also influenced. The association between the process of migration and contraceptive use dynamics is analysed using cross-tabulation with percentages and logistic regression analysis. The findings show that, in Kenya, migration influences contraceptive use among migrant women. That is, the probability of using contraception is higher among the migrant women than the non-migrants. The issue is important to researchers and policy-makers. Because fertility behaviour is influenced by change and characteristics of place of origin and destination, public policy interventions is necessary in order to account for the residential experience of women served by family planning and maternal child health programmes in different places. RÉSUMÉEn utilisant les données de l'Enquête démographique et de Santé (EDS) du Kenya de 1988/1989, l'auteur de cet article examine les rapports qui existent entre la migration et les déterminants de l'utilisation des contraceptifs au Kenya. Avec l'EDS, des données importantes sur les grossesses, l'utilisation de la contraception, le mariage, l'emploi, le lieu de résidence et la durée sur le lieu de résidence ont pu être collectées. Par cet article, l'auteur cherche à savoir si au Kenya la dynamique d'utilisation des contraceptifs par les migrantes diffère de manière significative de celle des non-migrantes. Cet article se fonde sur le principe que les femmes qui migrent sont un groupe qui agit de manière rationnelle pour profiter au maximum de la vie au dépend de leur rôle reproductif. L'étude a également comme hypothèse qu'en influençant le processus de fécondité, les caractéristiques de la migration influencent aussi l'utilisation de la contraception. L'association entre le processus de migration et la dynamique d'utilisation de la contraception est étudiée à travers des tableaux croisés entre les pourcentages et l'analyse de régression logistique. Les résultats obtenus ont montré que, au Kenya, la migration influence l'utilisation de la contraception parmi les migrantes. Cela veut dire que la probabilité d'utilisation de la contraception est plus grande chez les migrantes que chez les non-migrantes. Ces résultats sont utiles aux chercheurs et aux décideurs politiques. Puisque le comportement en matière de fécondité est influencé par les changements et les spécificités du lieu de départ et celui de destination, des mesures de politique publique sont nécessaires pour prendre en compte l'expérience des femmes assistées par les programmes de planification familiale et de santé maternelle et infantile à divers endroits. THE STUDY BACKGROUND AND OBJECTIVESThis paper has two objectives: to determine whether there is any difference between the contraceptive use dynamics by migrants and non-migrants and to identify the factors associated with migration which influence contraceptive use dynamics. Migration status has been found to influence age at marriage (Carlson, 1985; Courgeau, 1985; Smith, 1980b; UN, 1989; Van de Walle, 1992, 1993). Women who marry late tend to have fewer children than those who marry early although the causal relations have been noted to be affected by the level of contraceptive use, which weakens the importance of age at marriage in influencing fertility. In addition, differences in attitudes towards family planning differentiate the characteristics of migrants and non-migrants in their contraceptive use and may reflect rationality in behaviour that informs both mobility and fertility. The analysis of fertility determining factors and the existing differences in behaviour among different groups of women demonstrate the importance of residential characteristics (Deane, 1990). One contributory factor is the extent of contraceptive use by women of different migration status categories. Women migrating to different destinations may use and be exposed to different contraceptive behaviours. Additionally, if women leaving rural areas to urban areas are rational in their decisions to leave and innovative with respect to the types of challenges and opportunities they are seeking in urban places, they may find it more desirable than never-migrants at origin to use contraceptives to control fertility. They may seek to avoid constraints related to fertility to face the challenges and opportunities in the destination areas. They may also adapt to the fertility pattern and behaviour of those women who have spent the rest of their lives in the destination areas. However, if women migrate to urban areas because of different pressures ‘forcing’ them out of the rural areas, they may well be bringing with them not only rural fertility values, but also limited knowledge and practice of contraceptives. Differences in attitudes towards contraceptive behaviour may also characterise women migrating within and to rural areas. Rural-rural and urban-rural migrations may also influence women’s contraceptive perception and behaviour. This may as well reflect a general rationality similar to that of the rural-urban and urban-urban, in that it may inform both their reasons for migration and consequently fertility behaviour patterns. Furthermore the changes in the characteristics of women due to migration may prompt migrants to adapt certain fertility behaviour characteristics and patterns including fertility control at origin and/or destination (Brockerhoff, 1995). Therefore, in order to understand the characteristics underlying the effects of migration on fertility, it is essential to understand the factors associated with fertility proximate determinants. The association between migration and contraceptive behaviour can be either direct or indirect. The indirect association may be through the effects of the different family formation variables, which have a direct association with the use of contraception. In addition, the socio-economic, cultural and demographic fertility related factors might encourage the use of contraception, either directly or through migration status categories. Furthermore, migration per se may also have a direct effect on contraceptive behaviour. For instance, migrants may find themselves unable to continue with contraceptive use either because of lack of knowledge of where to get contraceptives in the new environment or if the method being used requires clinical attention that may not be available during the process of migrating. Use of contraceptive methods may also not be advisable if the woman is involved in migration because of their associated inaccessibility and side effects. The paper therefore, examines the contextual, intervening, and proximate variables influencing contraceptive use. For example, type of place of residence may account for the influence of characteristics of the place of residence on contraceptive use. For example, urban areas in many developing countries are often associated with higher education, better access to medical care and family planning, and other social services (Cochrane, 1989). Consequently, rates of contraceptive use have been found to be higher in urban than rural areas. Region of residence can be used as a proxy for cultural and/or traditional influences on reproductive behaviour characteristics. Region of residence has received increasing attention as a macro factor affecting contraceptive use in many less developed countries (Cleland and Wilson, 1987). Studies with this emphasis propose explanations for regional differentials in contraceptive use. A socio-economic hypothesis suggests that regions whose women have low education, limited formal-sector employment, and limited access to health and family planning outlets (supply factors) are expected to have low rates of contraceptive use. In addition, region of residence may be a proxy for ethnic or cultural boundaries that are related to acceptance of contraceptive methods (demand factors). Furthermore, the whole point about migration is that it changes the region of residence and mixes people; and many of the supply and demand factors are known for specific regions/provinces. Education level shows whether the likelihood of contraceptive use is high among educated people or not and helps in inference to the attitudes and/or perceptions to fertility regulation and desired family size, especially among husbands/partners. Age is a cohort marker and precedes other variables. Age is related in a curvilinear fashion to contraceptive use. In addition, couples are less likely to use contraception when fecundity is low, especially at the oldest and the youngest ages. Furthermore, use of contraceptive may decline at the oldest ages even among apparently fecund women because of declining frequency of intercourse due to migration. However, older women may also wish to have more children and therefore may use contraceptives less frequently. Marital status has been redefined differently to the categories used in the KDHS to capture contraceptive use. Married women who are not living with their partner/husband may have a different contraceptive behaviour from those who are married and living with their partner/husband due to their circumstance of marriage and/or socio-cultural and economic expectations. Also, unmarried women and previously married may also differ in their contraceptive perception and use between them and among the other groups. Contraceptive use is characterised by reliance on traditions mainly in the rural areas and modern methods in the urban areas. Migration may therefore lead to exposure to contraceptive for those who had not used any and to new methods for those who have been users. Independent of changes in family size preferences, non-use may result in migrants inability to obtain contraceptives in the new settings due to unawareness or inaccessibility of sources or from lack of sufficient resources to pay for the services in the new areas. Return migrants may devote less effort and resources to obtain contraceptives. DATA AND METHODSData Source Data for this study comes from the Demographic and Health Surveys of Kenya (KDHS, 1989), conducted by the National Council for Population and Development (NCPD) and the Central Bureau of Statistics (CBS) of the Government of Kenya (GoK). The DHS is an international data collection and analysis project sponsored since 1984 by the United States Agency for International Development (USAID). The Demographic and Health Surveys is a follow up of the World Fertility Survey (WFS) and the Contraceptive Prevalence Survey (CPS) projects of the late 1970s and early 1980s. They are intended to serve as a source of population and health data for policy makers and for the research community. In general, the objectives of the DHS are as follow: assess overall demographic situations of the countries or regions concerned; assist in the evaluation of the population and health programmes; advance survey methodologies; and assist the concerned governments to strengthen and improve its/her technical skills to conduct demographic and health surveys (DHS, 1991). Much of the content of the DHS is similar to that of the WFS. Similar questions were asked on factors related to birth history, recent and current use of family planning services, current breastfeeding; practice and coital frequency. However, in the Demographic and Health Surveys, marital status history does not take into account marital status at particular times in the past. This also applies to work status and occupation of women and their husbands in the past. In some key respects, the DHS is innovative. Whereas information on child mortality and its determinants is limited in the World Fertility Surveys due to its main focus on fertility, and is absent from the Contraceptive Prevalence Surveys, the DHS devotes considerable attention to both child mortality and morbidity and its related factors. In addition, the DHS has been designed within an increasing recognition that knowledge of child mortality in low income countries lags behind knowledge of fertility; that the persistence of high mortality in areas of Sub Saharan Africa, south Asia and the Caribbean inhibits sustained fertility decline; that fertility and child mortality are related at the micro-level (e.g. through birth spacing); and that factors which led to the demographic transition in areas of East Asia, such as the diffusion of family planning, rapid economic movement, political stability, land reform, migration, resettlement and urban growth, are unlikely to follow the same pattern in most contemporary low income countries, implying a need to search for other possible initiators of mortality and fertility changes. However, a distinctive feature of the DHS, integral to this study, is the inclusion of questions of residential experience, unlike in the past surveys or census. These are: type of residence for most of the childhood up to age of twelve (classified as city, town, village/countryside); number of complete years spent at the current location; for women who have lived outside their current location at sometime in their life, type of previous residence (categorised as for childhood residence). Those women who lived elsewhere at some period in time are considered as migrants. Thus the question on years of residence, combined with information of current place of residence help identify a broad array of migrant types such as: migrant status (migrants and nevermigrants); migrant categories (rural-urban, rural-rural, urban-urban, and urban-rural); and nevermigrant categories (rural natives and urban natives). In addition, migrant information can be obtained from variables dealing with current place of residence and childhood and previous residence question in the DHS (how long have you lived continuously in your current place of residence) in combination with current place of residence is used to determine the status and types. Those whose answers were "always lived" are here considered as nevermigrants, and those who answered in number of years lived at the current residences are treated as migrants. Questions on previous residence although available is not used because it is not possible to determine exactly what the previous residence means and is. Similar shortcoming is also attributed to the variable dealing with the childhood place of residence. However, the data on residential experience do have some shortcomings. The most obvious is that few temporal and spatial aspects of migration are captured. We can know migration took place, but we do not know, the duration of stay at the previous location, when the move did occur, whether during the childhood of or from a childhood residence to a non-current location, and the age at which it occurred. In short, many migrations may have occurred, but not more than one or a speculative second can be identified. The exact location of childhood and previous residence are also unavailable. Migration data may also contain misreporting of duration of current residence, and identification of migrant origins by their current status rather than former status (e.g. if village-market has become a town), particularly among older women. An additional problem is whether selective return or onward migration or mortality make migrants during a preceding period time, because literature on urban migrants, for example, documents return migration of both the successful and the unsuccessful in developing countries. The Kenya DHS utilised cross-sectional focused questionnaires to collect nationally representative sample. They interviewed women regardless of marital status, based on a stratified probability sample. The samples used a B-core questionnaire designed for countries with low contraceptive prevalence. Localities were categorised according to definitions used in the census enumeration. The Kenya Demographic and Health Surveys was designed primarily to: provide data on family planning and fertility behaviour of the Kenyan population to enable the government to evaluate and enhance the National Family Planning Policy programme; measure changes in fertility and contraceptive prevalence and at the same time study the factors which affect these changes such as age, marriage patterns, residence (urban/rural), availability of contraception, breastfeeding habits, and other socio-economic factors; and examine the basic indicators of maternal and child health in Kenya. They were not designed to be migration study. Being primarily a fertility survey, the respondents were not asked residence history. Thus this study heavily relies on the basic residence questions asked as background information in the DHS. Each respondent was asked if she had always lived in a residence to obtain information on her migration status as of the survey date. Migration was defined on a spatial criterion by asking the type of residence for most of the childhood up to age twelve (classified as city, village); for women who have lived outside their current location for a continuous period of six months or more at some time in life, their type of previous residence (categorised like childhood residence); and by temporal criterion by asking the number of complete years spent at current location. Those women who had lived elsewhere at sometime (temporal criterion) are considered here as migrants. Women living at current location for less than six months and not intending to stay have been classified as visitors and are to be excluded in the analyses. Once migration status is ascertained, a detailed residence characteristic is obtained for the migrants using the same temporal and spatial criteria. A careful examination of residential change yields information on types of migration streams, since the survey covered both rural and urban areas, duration of migration and whether migrants are recent or long-term. It is therefore possible to create a migration typology by type of migration stream or duration. An advantage derived from this is that information on multiple moves, in the form of return or onward migration may also be captured. Also, it is possible that the shift of origins and destinations from rural to urban or vice versa and the different lengths/duration of stay at the destination among movers may affect the relationship differently. STUDY SAMPLE AND SIZE A total of 7150 women of reproductive ages (15-49) were interviewed, covering 95% of the population spread over the country’s provinces, except North Eastern province and four northern districts (Samburu and Turkana in Rift Valley Province and Isiolo and Marsabit in Eastern Province). The excluded areas account for less than 5% of Kenya’s population. Out of the total number interviewed, the study uses a sample of 3638 women excluding those who were categorised as visitors as at the interview were eligible for analysis excluding those who were categorised as visitors as at the interview, who had no had sex in the last four weeks and those pregnant. The sample used includes only these women because they are the ones exposed to the risk of pregnancy and are likely to want to use contraceptives. Quality of the DataDetailed evaluation of fertility and infant mortality data from the Republic of Kenya Fertility Survey (CBS, 1977/78) after which the KDHS was patterned shows no strong evidence of data errors such as omission of births or deaths in the fertility indicators (Brockerhoff, 1995). But generally, three main types of errors to be expected in retrospective survey data are: omission of events or individuals who may affect reliability of estimated national rates and trends and reliability of estimated fertility differentials; misreporting or displacement of dates of events which could result in the problems of inaccurate calculation of fertility indicators like birth intervals and maternal age at birth, distortion of fertility trends, inaccurate number of births, and misstatement of respondents current age and; errors arising from the sample implementation (e.g. Under-coverage). The first two types of error typically result from poor recall of date, often in the distant past, and may be particularly common in the rural areas, where education levels are normally low and little importance is placed on accurate knowledge of births and deaths and changes of residents. Coverage errors are often unavoidable. Only women who have survived and did not migrate out of the country are included in the sample of migrants. This may bias estimates of fertility. More recent demographic events such as births or migrations are more likely to be reported than events more distant in time from the survey date. In the case of event history data, the distributions of dates of migration suffer from heaping for migrations during the more recent years prior to survey. Given the fact that the data used do not involve residence history, problems such as recall bias for migration may not be serious, except for the fact that some respondents may not know the exact length of stay at the current residence and may also confuse previous residence of childhood residence. Another problem of significance is residential categorisation. But this is overcome by using the categorisation designed for all other data collection surveys, rather than the respondents own residential categorisation. Thus one may consider these data to have no indication of a residence bias problem. Also, primarily a fertility survey, the DHS obtained information as at survey date from women aged 15 or over. Furthermore, the pregnancy history available in the data cannot be used because of lack of similar data on migration. Another constraint is the exclusion of the migration experience prior to age 15. Retrospective residence information was asked of women aged 15-49 at the time of the survey, the usual age criterion for most of fertility surveys. It may be argued that spatial mobility at early aged prior to age 15 exerts influence on migration behaviours and even actual mobility in the later years. Differential effects of the predictors between those with and those without migration experience prior to age 15 therefore cannot be captured. Another restriction is the one arising from the 6-month time criterion in the definition of migration. This excludes shorter duration migrations (visitors), such as those occurring several times within a year. These shorter duration may be regular, but mainly including short distance moves, the nature of which can differ from the longer duration moves: those occurring more than once but captured the 6-month rule. Implication to the studyThe Demographic and Health Surveys (DHS) provides good body of data for analysis of the relations between migration and fertility. Furthermore, the Demographic and Health Surveys has information on fertility and background variables useful for analysis designed to test the characteristics of a woman who had changed residence, obtained from data gathered by a question dealing with the length of time the respondent had been in her current place of residence and the type of current place of residence. This part of the DHS questionnaire is important especially as it can provide useful insights into the characteristics of respondents who had migrated and who had not migrated. As has been pointed out in the discussion earlier, despite the availability of the necessary data for the analysis, some information is still lacking, particularly the information relevant to the temporal aspect of the migration and fertility data, which can help in accounting for the changes occurring at a particular stage of time. Temporal information would allow more calculation than is now possible, especially in relation to the intervals between events. Additionally, such a data are essential in allowing the determination of whether migrants do in fact differ from never migrants at origin, how they differ from the host population into which they move, and how these differences change with longer duration of residence. Such migration and fertility histories would also allow assessment of whether the move itself results in longer-than-average delays in childbearing by permitting comparisons of the fertility behaviour of the migrants with women who did not at point as well as destination. However, important sociological and demographic research questions have evolved around issues of interdependencies between life events. These questions have been addressed within the framework of linear regression equation system. It is the interdependency between migration process and fertility behaviour mechanisms that is of interest. The data available for this study allows for this interdependency to be explored using descriptive and multivariate analyses handled in the respective chapters. The parameters used in the regression analyses conducted are tested for any evidence that the necessary assumptions such as multi-collinearity, interaction effects, the continuity and normalisation of the dependent variable are violated. The correlation coefficient between a pair of variables based on all cases was conducted before undertaking the main analyses. Preliminary bi-variate tables were run for each and ever model used to find out if there are variables, which are highly correlated (>0.5) to help in their elimination in the models. For example, residence variables were found to highly interact with types of migration, hence were not included when analysis took into account migration streams. The dependent variables for the logistic models are dichotomised for the logistic regression analysis. Thus, this paper uses cross-tabulation and logistic regression techniques to measure the relationship in question. Contraceptive use is the dependent variable. The independent variables include migration statuses and background variables. In addition, assessment of the relative effects of the background variables on contraceptive use while controlling for migration status is carried out. RESULTS AND DISCUSSIONCross-Tabulation Analysis This first section presents cross-tabulation analysis results of contraceptive use among women by various background characteristics (Table-1). It shows the percentage of women currently using contraceptives by selected characteristics and by migration status. Contraceptive Use Dynamics among Migrant Women by Various Background Characteristics From the results, contraceptive use is higher among migrants than the never-migrants. Among migrant categories, urban migrants have higher contraceptive use than rural migrants. In particular, rural-urban had the highest contraceptive use. Among the never-migrants, urban natives have the highest level of contraceptive use. This suggests that being a migrant disposes a woman to relatively higher contraceptive use than a never migrant. For instance, rural-rural migrants have a higher contraceptive use than the rural natives, as do the urban migrants relative to urban natives. Contraceptive use is low for women with no children and much higher for the women with a number of living children, especially more than three. The level of use of contraception seems to depend on the number of living children. Some women who do not have children may be young and not sexually active. Hence they do not need to use contraceptives because they are not at risk of pregnancy. This assertion is borne out by the fact that the proportion of women in sexual relations is fairly high for women who are still in teens. Table 1: Percentage of Migrant Women Currently Using Contraception by Background Characteristics
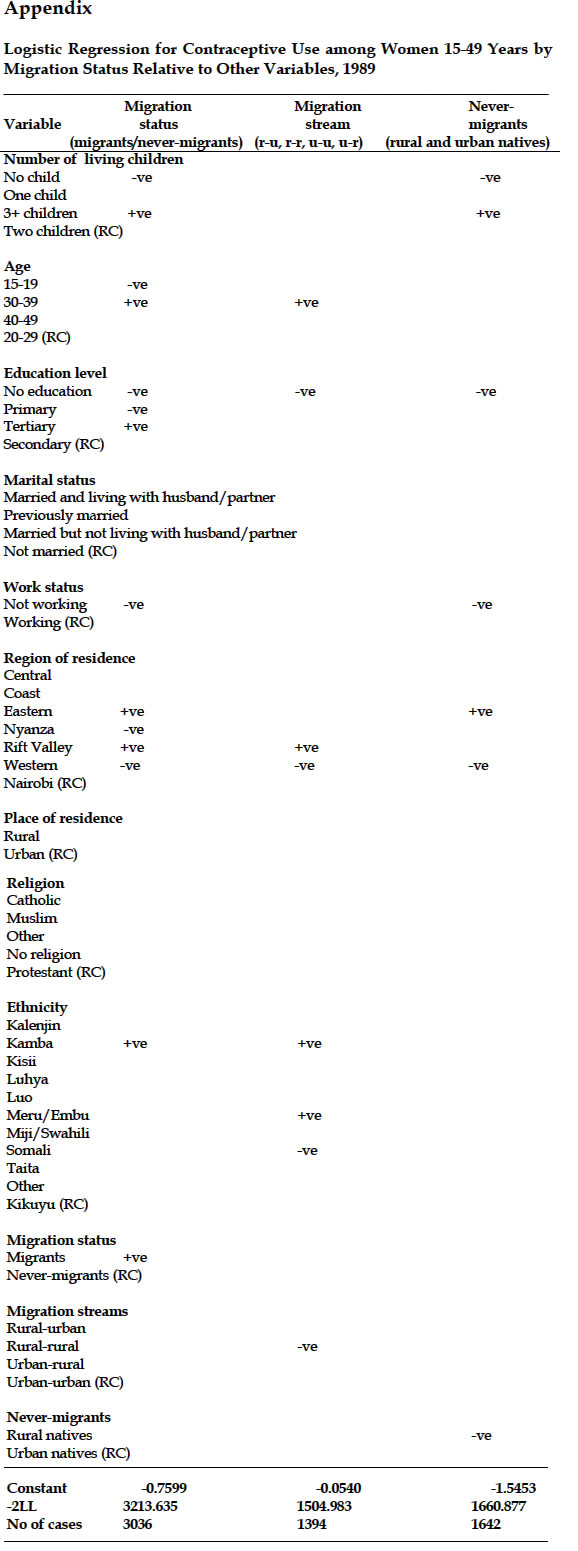
Women who have several children (3+ children) and do not wish to have more children are more likely to use contraception than their counterparts who have fewer children. Similar patterns are also noted when contraceptive use is examined by the different migration status categories. Besides, the fertility of migrants depends upon the number of children a woman has had. Contraceptive use is high among women aged 20-29 and low at younger and older ages, especially by migration categories. Contraceptive use increases for women up to age 20 years then begins to decline as the woman approaches 40 years. This is plausible because at this age women may start experiencing menopause, hence curtailing risk of conception. However, women in the twenties and thirties are more likely to use contraceptives. Similar patterns are also seen when migration status is controlled, although among rural-urban migrants contraceptive use is most common among older women, which may be a reflection of the characteristics and challenges of urban environments and may also be due to the characteristics of those who migrate to the urban areas. A positive relationship exists between contraceptive use and migration status. Almost half of the women with secondary education and over 80% with tertiary education use contraceptives compared to less than 40% of women with no-education and primary education. Similar patterns are observed when migration status categories are controlled. However, although overall difference in contraceptive use between never-migrants and migrants does not seem large, clear differences exist among the different education categories by migration status, especially between none/primary education and post secondary education of rural-urban migrants. Region of residence shows a strong differential influence on contraceptive use. The influence of regions of residence by migration status categories shows similar effects on contraceptive use. Regions in which conformity to traditional reproductive practices are weaker and are people socio-economically strong, like Central, Nairobi, Rift Valley and Eastern Province show higher contraceptive use. For example, the case for Nairobi could be attributed to urban influence and family planning availability whereas regions like Nyanza has low CPR. In these regions women are more likely to be well educated, marry at relatively high ages and discuss family planning. However, regions in which conformity to traditional reproductive practices are stronger and people are socio-economically weak, like Nyanza Province, Coast and Western Province, show relatively low levels of contraceptive use. Similar patterns are attributed to contraceptive use by regions when migration status categories are controlled. However, distinct patterns emerge by different streams that may reflect the specific characteristics of individual migrants and place of destination. Rural-urban migrants from Western, Rift Valley and Central provinces show the highest contraceptive use. Differences exist in the pattern of contraceptive use and work status. Women who work demonstrate a much higher use of contraceptives than those who do not work. Similarly, among the different migration status categories women who work show a higher level of contraceptive use than those who do not work. When migrants and never-migrants are compared, migrants who work have a higher contraceptive use than their never-migrant counterparts. Hence, contraceptive use among urban migrants and urban never-migrants is higher than those of rural migrants and rural never-migrants respectively. In general, of all the migration status categories, rural-urban migrants who are working have the highest level of contraceptive use. Women who are married but not living with their partner/husband, and those who were previously married, have higher contraceptive use than women who are married and living with their husband/partner and those who are not married. Women who are married but not living with their husbands/partners may use contraceptives to avoid being pregnant in absence of their husbands/partners lest they are accused of being promiscuous. Among previously married women, contraceptive use may be high to avoid becoming pregnant and the ensuing responsibility and cost of having to bring up a child alone. However, contraceptive use is lower among married women than among unmarried women. This may be because of the non-acceptance of contraceptive use by partners/husbands and/or the desire for more children among couples. In addition, the cultural responsibility to have children attached to marriage may militate against contraception amongst couples. Low contraceptive use by the unmarried women could be due to the fact that they are young and have no access to contraception or have their sexual behaviour institutionally or culturally controlled. They may also still be in school. Furthermore, the cost may make it impossible for them to use contraception. A similar pattern is noted when control for migration categories is instituted. However, migrants consistently have a higher contraceptive use compared to the never-migrants especially among the women who are married but not living with their husbands/partners, further reinforcing the aspect of social and physical separation and the opportunity these women may be having to determine their fertility behaviour and desires in the absence of their husbands/partners. In addition, the fact that women who are married but not living with their husbands/partners and are migrants portray very high contraceptive use may imply that migration creates an opportunity for contraceptive use among partners who otherwise would not use, let alone discuss, contraception. Among the different religious groups, Protestants have the highest contraceptive use followed by Catholics. Muslims and other religions have low contraceptive use. Those stating ‘no’ religion have the lowest. This pattern confirms results of several studies about religion and contraceptive behaviour. Protestants have been found generally to be flexible in the use of contraception in regulating reproduction unlike Catholics and the Muslims. Similar patterns are confirmed even when migration status categories are controlled for. Contraceptive use and ethnicity follow similar patterns to regional differences. Groups living in regions in which conformity to traditional reproductive practices are weaker (Kikuyu, Kamba, Meru/Embu) show higher use of contraceptives, whereas groups living in areas in which conformity to traditional reproductive practices are stronger (Luo, Luhya, Kalenjin, Kisii, and MijiKenda/Swahili) have lower contraceptive use. In general, contraceptive use by ethnicity/ethnic groups shows that contraceptive use depends upon the origin of the community of residence. However, further differentiation by different migration categories show that there is some influence on contraceptive use by migrant’s place of destination, irrespective of place of origin as can be seen among the Luhya, Luo, and Kisii of the rural-urban migrant category, although much more for the Luhya than Luo. LOGISTIC REGRESSION The effect of migration status on contraceptive use among migrant womenIn order to assess the relative importance of each variable when others are controlled, a logistic regression is undertaken. Use or None Use of contraceptives is taken as the dependent variable. The individual woman is taken as the unit of analysis. Parameters similar to the ones used in the cross-tabulation analysis are also used in the logistic regression. The analysis is done at three levels: Contraceptive use and background factors, Model 1; Contraceptive use and migration status, Model 2; and Contraceptive use and all variables, Model 3. Table 2: Effect of Migration Status on Contraceptive Use among Migrant Women. Odds and Ratios of Contraceptive Use
Effect of migration status relative to background characteristics on contraceptive useThe logistic model results in table 2 confirm findings from the cross-tabulation analysis, that being a migrant significantly increases the probability of using contraceptives compared to never-migrants. The odds ratio of migrants using contraceptives is 1.0713 compared to the never-migrants. This means that change of residence increases the likelihood of a woman using contraceptives because it may expose the migrant women to areas of high contraceptive prevalence thus making it easy to access and use. In addition, migrant women may also be selected according to the characteristics positively related to contraceptive use. The regression results show that women with more children (3+) are more likely to use contraceptives than those who have two children. This confirms the previous descriptive results that, the number of living children, especially in the developing countries where modern family planning is of recent origin, and effective family size, that is, the number of children at the time when couples start contraception, are of primary influence over the frequency and pattern of contraceptive use. One would argue that, couples in Kenya who have had as many children as they want would seek a means of preventing further births, and that those who have fewer than they desire, but who want their additional children at preferred intervals, not achieved by abstinence or extended breastfeeding, would adopt contraceptive use. Also, use of contraceptive is found to increase as a woman becomes older. Women between ages 30-39 are more likely to use contraceptives than women in age groups 20-29. This may be because these women are at an important period of their career development and may regularly discuss matters relating to and use contraception to avoid conception that may interfere with the careers. They may also be well educated, married at relatively higher ages, have three or more children, do not desire more children and hence are more likely to use contraceptives. Education is also positively related to contraceptive use. Women with tertiary level of education are 3.5 times more likely to use contraceptives than women with secondary education. Contraceptive use is noted to be stronger among women who have received secondary plus education. This may be because such women might have married at relatively higher ages; can openly discuss family planning with peers and/or husbands/partner; and desire no more children for other competing roles. A significant difference is seen between those women with no-education and primary education who are less likely to use contraceptives than those with post secondary education compared to the women with secondary education. Women who do not work are less likely to use contraceptives than those who work. This may be because women who work are relatively better educated than those who do not work. Among the regions of residence, women in Central, Nyanza are more likely to use contraceptives compared to women in Nairobi and women in Western province. This signifies the regional socio-economic and cultural differences existing in Kenya. Thus, region of residence may be important in understanding the pattern of contraceptive use in Kenya in terms of the other related factors such as the education of women and age at first marriage. Women living in urban areas were found to have a higher probability of using contraceptives than women living in the rural areas. This may be because many aspects of urban life such as greater exposure to mass media and easier access to family planning services may exert strong influence on the adoption of family planning practices in urban areas than in rural areas. However, religion, marital status and ethnicity are non-significant. Effect of migration status (migration streams) relative to the background characteristics on contraceptive use Using the same model and parameters but further sub-dividing migration status into components, results of migration streams relative to background parameters significantly relate to contraceptive use. Contraceptive use is positively related to rural-urban and urban-urban migrants. Rural-urban migrants were found to more likely use contraceptives compared the urban-urban migrants. However, rural-rural and urban-rural migration is negatively related to contraceptive use. Rural-rural migrants were approximately 40% less likely to use contraception and urban-rural was approximately 20% less likely to use contraception than urban-urban. These results imply that place of destination may be critical in determining whether a migrant woman uses contraception or not. In addition, contraceptive use is found to be more likely associated with women with several living children, old women, women with high education level, women who are married but not living with their husbands/partners, women who are working, and women living in Central Province. Women who are married and living with their husbands/partners are less likely to use contraceptives. The probability of using contraceptives is low among women who do not work. In relation to the regions of residence, women living in Central, Eastern and Rift Valley Provinces are more likely to use contraceptives than their counterparts in Nyanza and Western Provinces. Similar association to the regional differences are seen among ethnic groups who live in these regions. Effect of migration status (non-migrants) relative to background characteristics on contraceptive use Women who live in urban areas are more likely to use contraceptives than women who live in the rural localities that may imply selectivity characteristics. Rural natives have a significant negative association with contraceptive use. Women with many living children are found to be more likely to use contraceptive use so is women with high education. Women who are working have a higher chance of using contraceptives than those who are not working. In relation to regions of residence, women living in the Provinces of Nyanza and Western are least likely to use contraceptive. CONCLUSIONThis analysis has shown that migration status categories are significantly but differentially related with contraceptive use. Migrant women are more likely to use contraception than never-migrants. Urban migrants are more likely to use contraceptives than rural migrants. Among the never-migrants, urban natives have been found to be more likely to use contraceptives than rural natives. Migration between different types of locations, especially from rural to urban areas, seems to result in greater changes in contraceptive attitudes and behaviour. In addition, the fact that women who migrate to urban destinations are more likely to use contraceptives may lend credence to the hypothesis that innovative ideas or information on fertility regulation are stronger in settings which are modern, than in traditional settings and have also spread less to traditional or less modern areas. This further points to selection process of migration. Number of living children, age, education, marital status, place and region of residence, work status and religion have also been found to significantly influence the probability of using contraceptives. This study has also found that the probability of using contraception is lowest for women without a child, or those having fewer children, and increase as women appear to achieve their reproductive goals. Education was found to be a very strong predictor of contraceptive use, showing an increase in contraceptive use as educational level increases. The patterns of contraceptive use by marital status also show that married women who live with their husbands/partners have lower chances of contraceptive use compared to their counterparts who are not living with their husbands and those who were previously married. In terms of work status, women who work are more likely to use contraceptives than those who are not working. This may be because, apart from work being associated with better education and exposure to new socio-behavioural environments, work may also promote social and physical separation that may encourage use of contraceptives in different environments. The results also suggest that region and place of residence are important contributors to differentials in contraceptive use. Women are more likely to use contraception if they live in certain regions and places in Kenya, which enhances the importance of migration as one of the factors that may contribute to the changes in fertility and growth. Moreover, since the current transition to lower fertility may be attributed largely to contraceptive use in different places and regions, especially between urban and rural areas, which attach different attitudes, cultural, and social values to reproductive behaviour mechanisms, like contraceptive use, the migration factor needs to be directly considered in Family Planning programmes and policy matters. REFERENCES
Copyright 2003 - Union for African Population Studies The following images related to this document are available:Photo images[ep03011a1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}