 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 18, No. 2, Oct 2003, pp. 105-132 Use of Family Planning in Lesotho: The Importance of Quality of Care and Access Maletela Tuoane1 Ian Diamond 2 and Nyovani Madise2 1National University of Lesotho, Lesotho, 2 University of Southampton, United Kingdom 1Acknowledgements: Maletela Tuoane was partly supported by the Population Investigation Committee (United Kingdom) research fund to collect the Facility Survey data. Code Number: ep03013 ABSTRACT This paper aims to identify social and demographic factors affecting contraceptive use and methods choice and also explore whether, net of these factors, contraceptive behaviour of Basotho women is affected by the family planning environment in which they reside. The study uses multilevel models and data from three sources: 1995 Lesotho Safe Motherhood Initiative Women’s Health Survey, information collected in 1997/98 on the facilities of family planning clinics in some areas of Lesotho, and focus group discussions of users of contraceptives. Women aged 20-29, with at least two living children, and those with secondary or higher education have the highest probability of using modern methods. Community differences in use of contraception are explained by provider bias, access to a facility, and the type of facility. Excerpts from focus group discussions indicate that the quality of care is also important in influencing the decision by women to use contraception. RÉSUMÉ Dans cet article, l'auteur cherche à identifier les facteurs sociaux et démographiques susceptibles d'influencer l'utilisation de la contraception et le choix des méthodes. Sur la base de ces résultats, il cherche à établir si le comportement des femmes basotho en matière de contraception est influencé par l'environnement de planification familiale dans lequel elles vivent. Pour ce faire, l'auteur utilise les modèles multiniveaux, ainsi que des données provenant de trois sources: le Lesotho Safe Motherhood Initiative Women's Health Survey de 1995, les données collectées en 1997/98 sur la disponibilité des centres de planification familiale dans certaines régions du Lesotho et les Focus Group d'utilisatrices des contraceptifs. Les femmes âgées de 20 à 29 ans ayant au moins deux enfants vivants ainsi que celles qui ont été jusqu'à l'enseignement secondaire ou supérieur sont celles qui utiliseront les méthodes modernes le plus probablement. Les facteurs qui expliquent les différences constatées dans l'utilisation de la contraception sont l'influence du fournisseur, l'accès à un centre et le type de centre. Des extraits de Focus Group montrent que la qualité des soins est également un facteur important dans la prise de décision par les femmes d'utiliser la contraception. INTRODUCTION Use of contraceptive methods allows women to postpone pregnancy, alter the timing between pregnancies, or avoid pregnancy completely (Hawkins et al., 1995). Couples can choose from a range of contraceptives and the decision to use and to choose a particular method can be influenced by decisions made at various levels: at national and regional level, at community and clinic level and at individual level. At the national level, policies are set concerning the methods to be included and excluded from public and private family planning programs. At the community and clinic level, resources and administrative decisions influence the relative accessibility of particular contraceptive methods, and at the individual level, people desiring to avoid or delay an additional birth make decisions about which method to adopt (Davidson, 1989). Therefore, understanding factors affecting family planning in Lesotho, particularly the importance of quality of care and access, is necessary for informed population program policy formulation. BACKGROUND Lesotho is an independent mountainous country in southern Africa sharing all its boundaries with South Africa. It occupies an area of 30,355 square kilometers making it one of the smallest land locked countries in Africa. The Basotho (people of Lesotho) are a homogeneous group, identified by one language, Sesotho. They have one tradition relating to marriage, child up-bringing and other traditional practices. In the past, they have been noted for having the highest literacy levels in southern Africa (World Fertility Survey, 1981) and the country is normally considered unusual because females are more likely than males to be educated (Lucas, 1992). Lesotho has a limited resource base; water is the only major natural resource in the country and is currently being developed through Lesotho Highlands Water Project. The other main resource is migrant labor to South Africa, which has had a notable impact on Lesotho’s demography in the past few decades. Prior to 1977, miners signed contracts of up to two years and remained absent from their families for periods averaging 16 months. However, in the recent past, the number of migrant workers has been declining due to South Africa’s policy of internalization of labor and the fact that migrant workers are allowed to return home for long weekends at frequent intervals (United Nations Population Fund, ND). Currently, a typical mineworker visits home at least once every three months and visits are usually made during the weekends (Central Bank of Lesotho and Bureau of Statistics, 1995). For a long time, little was known about fertility in Lesotho. Since the 1977 Lesotho Fertility Survey, undertaken under the auspices of the World Fertility Survey, Lesotho has reported moderate levels of fertility by sub-Saharan African Standards, around five children per woman, accompanied by very low levels of contraceptive use. These moderate fertility levels have been attributed mainly to long periods of postpartum abstinence as a result of lengthy absence of young adult males working in South Africa (Mpiti and Kalule-Sabiti, 1985). From 1977 until the last few years, fertility was thought to be constant and there has been little evidence of an increase in the use of contraception. Lesotho has a population policy that aims to achieve replacement level fertility by 2011, thus reducing the total fertility rate to 2.2 children per woman (Lesotho Government, Ministry of Economic Planning, 1994). As contraception has been identified as one of the most important proximate determinants of fertility in developing countries (Donaldson and Tsui, 1990), the government of Lesotho aims to raise the contraceptive prevalence rate (the Percentage of women of reproductive age, married or living in union, that use contraceptive methods) to about 70 to 75% by the year 2011. In 1991, a short-term goal was to raise the contraceptive prevalence to 31% by 1996. However, in 1998, contraceptive prevalence in Lesotho was estimated at 23%, indicating that the short-term aim has not been achieved. Although there has been some increase in contraceptive prevalence in Lesotho, it still falls below that required in order to achieve replacement level fertility which the government hopes to have by the year 2011. Contraceptive prevalence for Lesotho is much lower that that observed for other neighboring countries such as South Africa (50%) and Botswana (33%). In order to achieve the goal of Lesotho government, the patterns and factors associated with contraceptive behaviour of women in Lesotho need to be understood. Delivery of Family Planning Services in LesothoThe Ministry of Health and Social Welfare (MOHSW) has overall responsibility for the management of the national family planning program in Lesotho (World Bank, 1994). Family planning services are offered by both public and private health facilities. The MOHSW and the Lesotho Planned Parenthood Association (LPPA), an affiliate of the International Planned Parenthood Federation (IPPF), are the main providers of family planning services. Other agencies that offer family planning services include private hospitals and the Red Cross. In addition, there is social marketing of condoms through pharmacies, supermarkets, bars and nightclubs. The LPPA has been in operation since 1968. Since the launch of LPPA, the IPPF has been the major donor providing more than 90% of the funding for the program and general administrative services (Lesotho Government, Ministry of Economic Planning, 1995). The other service delivery activities of LPPA include the piloted community based family planning services for the national program and, on a small scale, employment based-family planning services. The government of Lesotho was initially cautious about offering modern methods of contraception due to a fear of negative response from the general public (World Bank, 1994), but it became directly involved in family planning in the late 1970s when it adopted primary health care as the cornerstone of its health delivery system. Since 1988, the government assists LPPA by providing a direct grant through an allocation in the MOHSW budget and by authorizing that project funds from donors be channeled directly to LPPA. Theoretical FrameworkThe study uses an adaptation of the demand and supply theoretical framework for evaluating family planning programs proposed by Bertrand et al (1995). This framework proposes that a range of factors that include individual factors, societal factors, external development assistance as well as political and administrative systems in a country, indirectly affects contraceptive practice through demand for family planning services and value and demand for children. All these have an effect on fertility and other health outcomes. The demand side of the framework includes individual and societal factors, which generate the demand for family planning services. At an individual level, factors such as parity, age, personal beliefs, the level of education and socioeconomic status are associated with the likelihood of using modern contraception (DaVanzo et al., 1989; Tanfer et al., 1992; Bertrand et al., 1995; Leite, 1997). Societal or community factors such as fertility preference, attitudes towards family planning methods may also affect the demand and uptake of modern contraception. Nationally, policies and development programs may influence fertility preferences and the demand for family planning services. On the supply side contraceptive practice may be influenced by: policy and administrative factors such as political commitment, resource allocation and regulations; organizational factors which include infrastructure, public-private partnerships, and delivery systems; operational factors and service outputs including management, training, supervision, IEC, access, and quality of services. The choice of family planning methods can be influenced by supply factors such as the availability of methods and the provider’s bias, but choice may also be influenced by individual characteristics. For example, women at different stages of the reproductive life may prefer different methods; women at the start of their childbearing years may prefer to use less permanent methods while older women, with several surviving children may want long-term or permanent methods such as sterilization. Rumors about potential side effects may also influence choice. It is clear that many factors influence contraceptive practice, operating at various levels of social organization. Many studies have identified individual level determinants of contraceptive use such as age, parity, level of education, and approval or disapproval of family planning by their partner. Similarly many researchers have acknowledged that community and service factors such as access to contraception and the quality of care can impinge on individuals’ decisions to use or not use modern methods or the choice of methods (Akin and Rous 1997; Koenig et al., 1997; Steele et al., 1999). Steele et al. (1999) used multilevel models on cross-sectional data from the women and the service availability modules of the Morocco Demographic and Health Survey (DHS) to model the influence of service factors on individual contraceptive use. Mensch et al. (1994) used two data sets (Peru DHS and Situation Analysis) to investigate the impact of the quality of family planning services on the ability of women from Peru to achieve their reproductive intentions. They found that quality of care has an impact in reducing unwanted and unplanned births. However, other studies found that the effect of service quality variables had no strong effect on contraceptive use in Nigeria (see for example Feyisetan and Ainsworth, 1996). A limitation of the service availability modules of DHS is that there is little information on the infrastructure of the facilities, the operation, or indeed on provider bias. DATAThis study combines data from several sources to identify individual and service level determinants of contraceptive use and method choice using multilevel techniques. The objectives of the study will be achieved by using both quantitative and qualitative data to analyze the patterns of contraceptive behaviour in Lesotho. The quantitative information may allow us to picture the patterns of contraceptive behaviour in terms of both individual and community characteristics. The ancillary qualitative information may allow us to further understand the cultural factors associated with contraceptive behaviour and family planning, giving answers and posing questions about the interaction of availability, accessibility and actual use of contraceptive methods and family planning services. The individual-level data are from the 1995 Lesotho Safe Motherhood Initiative Women’s Health Survey. The service information was collected during an audit of facilities at service delivery points across the country and through interviews with the service providers. Finally, excerpts from focus group discussions of users of contraception are used to provide group-level information of the experiences of women at family planning clinics. The Lesotho Safe Motherhood Initiative Women’s Health Survey (LSMI-WHS) was carried out by the Ministry of Health and Social Welfare, in collaboration with a country team from the World Health Organization, and the Lesotho Bureau of Statistics. The fieldwork for this nationally representative survey was conducted from January to March 1995 using two-stage sampling. In the first stage, systematic sampling was used to select 60 primary sampling units (30 from rural areas and 30 from urban areas) from the 1986 population census sampling framework. In the second stage, systematic sampling was used to select households within the selected primary sampling units. For the study to be representative of Basotho women, the rural and urban samples were weighted to represent proportions in Lesotho. The study population comprised all women aged eleven years and above and with a total sample size of 4,389 women. However, this paper uses data on those women in the conventional age-range of 15 up to 49 years. Only non-pregnant women and those who had ever had sex were included in the analysis. From the total sample, 1228 women were out of the age range of 15 to 49, 720 had never had sex and 216 were pregnant. A further 163 women were excluded because of missing information, leaving 2062 women for the analysis of determinants of contraceptive use, while the analysis of method choice was restricted to the 698 women who were contraceptive users. The audit of facilities offering family planning services was done between December 1997 and February 1998. In total, 38 facilities were visited representing about 41 % of all facilities in the country, excluding services offered by private doctors. The 38 facilities were selected from the communities that were sampled in the LSMI-WHS survey. The Facility Survey was designed and conducted especially to be linked with the LSMI-WHS to provide a more comprehensive picture of the family planning facilities in Lesotho. To link these data sources, it would be ideal if the data referred to the same areas and time period. The audit of the facilities, the interviews with the providers, and the focus group discussions were conducted almost three years after the LSMI-WHS fieldwork. The nearest service delivery points to the communities from the LSMI-WHS were selected and information collected on the services provided and the facilities available. Based on the primary sampling units (communities) selected in the LSMI-WHS, facilities were identified from which data on the delivery of family planning services were collected. It is noted that the collection of the Facility Survey data was conducted almost three years after the LSMI-WHS data were collected. It is possible that within these three years there could have been changes in the provision of services. To link the two data sets, providers were asked if there had been any changes in service provision in the three years prior to the Facility Survey. A total of three facilities were excluded from the analysis due to major changes that had occurred in the provision of family planning services in one facility and inaccessibility of two facilities. The rest of the service delivery points were reported not to have had any changes since 1995 and, therefore, it was concluded that the current service environment was the same as that which prevailed when women sampled in the LSMI-WHS adopted contraception. The audited facilities serve 57 of the 60 communities that were included in the LSMI-WHS survey, therefore, the three communities from which data was not available were excluded from the LSMI-WHS data. The data collected include a list of equipment for family planning provision, supply of contraceptives, availability of water, electricity, seating, and privacy (visual and auditory). The number of trained staff, record keeping, and evidence of aids for information, education and communication were also recorded. Using a structured questionnaire, service providers from these facilities were interviewed to find out about their practices when providing methods of family planning. Seven focus group discussions were conducted: four in urban areas of Maseru district and three in the rural areas. These focus group discussions were among women who were using family planning methods and the aim was to find out their views about the quality of service at their family planning clinics. Because contraceptive prevalence is low in Lesotho, it is rather difficult to find many women who are using modern methods of contraception particularly in the remote rural areas. Therefore the focus group discussions were restricted to women living in Maseru district, which has the highest contraceptive prevalence rate. It was also impossible to select women who were using family planning methods randomly, so a snowballing approach was used. In rural areas, where women were more secretive about their use of contraception, assistance was sought from the family planning providers in recruiting users of contraception. METHODS OF ANALYSIS Multilevel models are generally used to analyze data that have a hierarchical structure, such as the LSMI-WHS. It would be expected that women living in one cluster might have common influences such as similar attitudes towards contraception, or similar access to family planning services. An integral aspect of multilevel models is the ability to separate the variation in the response of interest into variation attributable to individual level factors and that which is attributable to higher level contextual factors (Rice and Leyland, 1996). The statistical software MLn was used for the analysis. MLn is a program for fitting multilevel models to data with an n-level hierarchical or nested structure. Second order penalized quasi-likelihood estimation was used for both the analyses of contraceptive use and method choice. The use of contraception is conceptualized as a two-step process: first, the decision to use contraception and then, among users, the choice of method. At both steps, the data from the quantitative survey fall into a hierarchy of individual women nested within communities. For the first step, the dependent variable is the current use of contraception and multilevel logistic regression is used to identify individual or community level determinants. The formulation of the multilevel logistic regression is given by the following equation:
Where, πij is the probability that woman i in community j uses contraception; x´ij are vectors of individual and community characteristics; β is a vector of estimated parameter coefficients associated with xij; and µj are the random effects representing unobserved factors operating at community level. The dependent variable for the second step is contraceptive method choice with three categories: pill, other methods and injectables. For this analysis, multinomial logistic regression is used on a data set of 698 current users. The reference category for the dependent variable is injectables. The model fitted for the multilevel multinomial logistic regression takes the form:
Where, m = pills and other methods πmij is the probability that woman i in community j uses pills or other methods; π3ij the probability that woman i in community j uses injectables (reference category); x´ij is a vector of individual and community characteristics; βm is the vector of parameters associated with xij for pills and or other methods; and µmj are the random effects representing the unobserved factors operating at community level for pills or other methods. The multilevel logistic and multinomial regressions first include individual characteristics in the model. The rationale for this approach is that the individual level characteristics help to explain the demand for contraception. The service factors operate on the supply side of the equation model and the residuals at the community level may be thought of as indicating the existence of other unobserved factors at that level. The significance of these residuals can be gauged by constructing simultaneous confidence intervals for each of the communities. The interpretation, used to determine whether any two communities have significantly different average contraceptive use or choice of method, is based on the examination of whether the associated confidence intervals overlap. If they do not overlap, the differences are statistically significant at the chosen level (see Goldstein and Healy, 1995). The second part of the analysis will include community level variables from the facility survey in order to explore whether, net of demographic and social factors, the decision to use contraceptive methods and choose a particular contraceptive method is affected by the family planning environment in which a woman lives. Definition of VariablesTwo types of analysis are employed in this paper: contraceptive use and method choice. The dependent variable for the analysis of contraceptive use is use or non-use of contraception, while for the analysis of method choice the dependent variable is use of injectables versus use of pills and other methods. The explanatory variables include characteristics of the women and characteristics of the family planning facilities. These variables have been chosen to reflect the factors that might be expected to be associated with contraceptive use and method choice in Lesotho. For the characteristics of the family planning facilities, some of the variables are selected as indirect explanatory variables. As noted by Mensch et al. (1994), demographers have long been interested in developing indicators from survey data that assess, even if indirectly, the efficacy of family planning programs. The individual woman characteristics include age, number of living children, education, marital status, partner’s education and partner’s work status, region and type of place of residence and whether or not a woman had a regular partner at the time of the survey. In both analyses, all two-factor interactions are tested. The characteristics of the family planning facilities which were included in the analysis are presence of family planning facility in the community, type of family planning facility, number of methods available, presence of maternity care or services, whether or not staff member was trained in family planning provision, provision of some methods of contraception and whether or not provider imposed restrictions in providing contraceptive methods. RESULTS Determinants of Contraceptive Use Preliminary ResultsTable 1 summarizes the use of contraception by a number of socio-demographic characteristics and community level variables. Overall, 29% of women exposed to the risk of conception use contraceptives. The relationship between use of contraception and the number of living children follows the usual inverted U-shape with the highest proportion occurring among women with two living children. A similar pattern is observed for maternal age. More than half of the women with post-secondary education were using contraception. The pattern of use by the partner’s education and work status shows that use of contraception is highest when the partners have secondary or higher levels of education and are working. If the partner is not working, contraceptive use is less likely. Differences are also observed in contraceptive use between women’s region and type of place of residence. Women living in Maseru, the capital, and those in the southern part of Lesotho have the highest contraceptive use and those in the mountain region the lowest. As expected, urban dwellers use contraceptives more than their rural counterparts. The family planning environment in which a woman lives is important. As expected, women living in communities where there is a family planning facility tend to use contraceptives more than those who have to travel to another place for the services. Also, women who have access to LPPA clinics have higher contraceptive use, followed by those who have access to both LPPA and a hospital. All LPPA clinics are in urban areas, which could explain higher contraceptive use among women with access to LPPA clinics. Table 1: Percentage of all Woman Currently Using Contraception by Selected Individual Characteristics, LSMI-WHS, 1995 and Lesotho Facility Survey, 1997/98
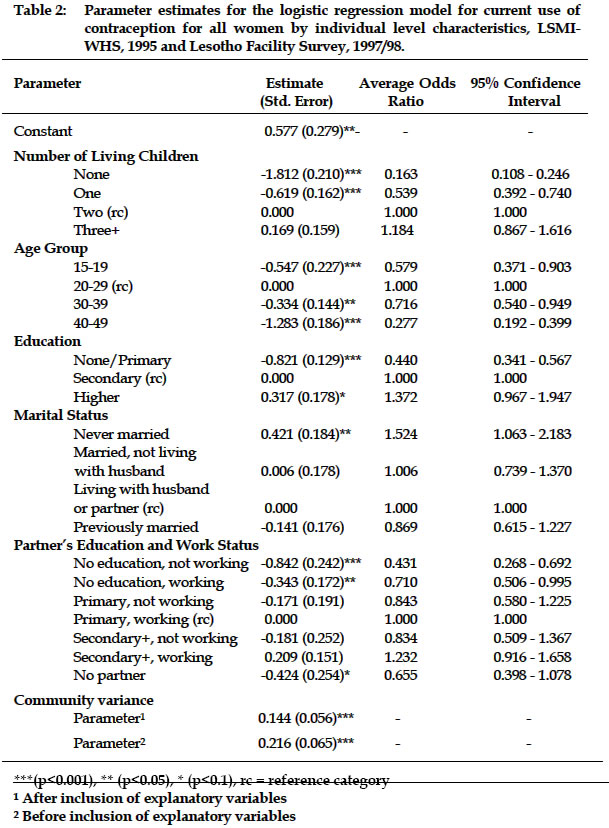
Note: The Percentage of users is based on weighted data Logistic Regression Results In order to assess the relative importance of each predictor of contraceptive use a multilevel logistic regression analysis was carried out. The significant factors found to affect the use of contraception for Basotho women are the number of living children, age, the level of education, marital status, partner’s education and the work status of partners. It should be noted that partner’s education and work status were only significant as a two-way interaction but not as individual variables. The results of the logistic regression are provided in Table 2, which shows the parameter estimates of the best-fitting model, together with their standard errors, odds ratios and the 95% confidence intervals of the odds ratios. The coefficient labeled community effect is the multilevel variance. The inverted U-shape relationship observed in the preliminary analysis between contraceptive use and age is confirmed, as is the positive relationship with women’s education. Women in the age group 20-29 have significantly higher contraceptive use than all other age groups. Among the other age groups, a significant difference is only observed for women aged 30-39 and those aged 40-49. Women aged 40-49 have the lowest average odds ratios, reflecting a decreasing need for contraceptive use among the oldest group of women. Younger women, those under 20, had the lowest levels of use (17% of women aged 15-19 were sexually active at the time of the survey. There are potentially many reasons for this but in focus group discussions, young women who had sought family planning methods reported that they were sometimes ridiculed by service providers, which could help to explain their low use of contraception even though they are sexually active:
The woman’s level of education is a very strong predictor of contraceptive use showing an increase in contraceptive use as education increases. A significant difference at the 5% level is observed between women with none or primary education and at the 10% between women with secondary education and those with higher education. Those with none or primary education are, on average, less than half as likely to use contraceptives as those with secondary education. This, therefore, indicates that with higher levels of education, women appear to demand contraception and to be autonomous enough to obtain and use it. A positive relationship is also observed between contraceptive use and number of living children. The results of the effect of the number of living children on contraception use for Lesotho are as expected. Contraceptive use is at its lowest when women start their reproductive career, increases as more of them use contraception for child spacing and increases even further as they achieve their reproductive goals and use contraception for limiting purposes. In addition, family planning providers were found to be discouraging women with no children from using injectables, pills and IUDs. No significant difference is, however, observed between women with two or more children, indicating that it is after having two children that the need to use contraception becomes apparent. The power of providers in influencing women to use contraceptive methods was observed in the focus group discussions:
Generally, women whose partners are working have higher contraceptive use than women whose partners are not working and contraceptive use increases as the education of their partners increase. The highest relative odds of using contraceptive methods are observed for women whose partners attained secondary education and are working and the lowest is observed for those whose partners have no education and are not working. This probably reflects high knowledge of contraception and potentially high opportunity costs of unplanned pregnancy for the more educated partners and for those working. However, education of the partner seems not to play a significant role in influencing contraceptive use for women whose partners are not working as shown by the overlapping confidence intervals in all these categories. Women with no partners are about a third less likely to use contraceptive methods than those whose partners have secondary education and are working. Marital status is also observed to influence the decision to use contraceptive methods. Women who had never married have the highest average odds of using contraceptive methods as compared to all ever-married women. Those who have never married are 52% more likely to use contraceptive methods than those who are living with their husbands or partners. This may reflect a higher motivation to prevent births among unmarried women who are sexually active. Having a premarital birth may reduce their chances of getting married or of continuing their education. Although unmarried women may be highly motivated to use contraceptive methods, it was evident from the focus group discussions that providers sometimes make it difficult for them to use contraception, and in addition, parental attitudes are particularly negative. For example:
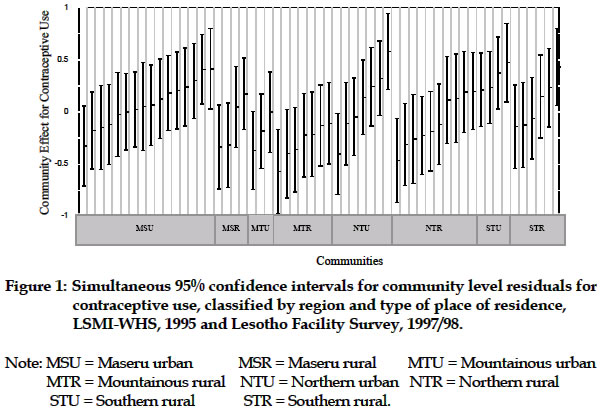
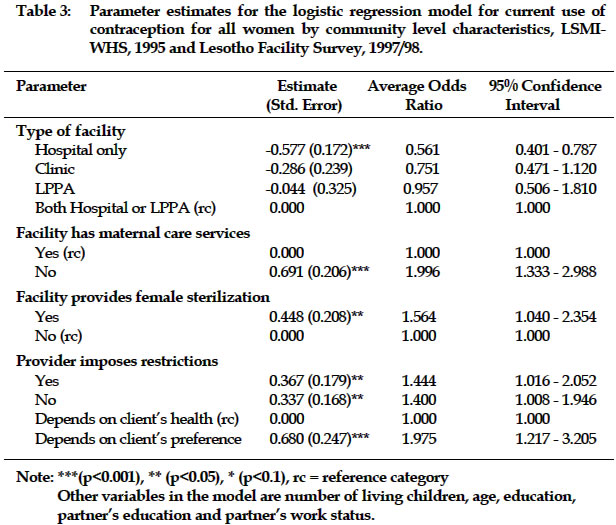
The community level variances are given at the end of Table 2, indicating significant parameter estimates, before and after the inclusion of social and demographic variables. It is noted that the community level variance decreased after the inclusion of the explanatory variables. This shows that the significant explanatory variables explain some variation between communities and also between women. The significant community variance indicates that even after controlling for social and demographic factors, there still remains unexplained variation at the community level. In order to determine the extent of inter-community variation in contraceptive use, confidence intervals are constructed and shown graphically in Figure 1. Figure 1 shows simultaneous 95% confidence intervals for community level residuals for contraceptive use, by region and type of residence. It is clear from the figure that there is no difference within communities in the same regions as all the confidence intervals in each region overlap, except in the northern region. Differences are, however, observed for different communities in different regions, with some communities in Maseru and the southern region having higher confidence intervals that do not overlap with lower confidence intervals in the mountainous region, indicating that communities in Maseru and the southern regions have relatively higher rates of contraceptive use. It is also observed that among the communities whose confidence intervals do not overlap, the higher ones are in the urban areas and the lower ones in the rural areas, also showing that urban communities have higher contraceptive use than rural communities. This variation between communities led to the next stage of research: to investigate if the delivery of family planning services differs for different communities and has a marked impact on prevalence. For example, women living in an urban community may have easier access to family planning services, have wider choice of method available to them or have better quality of services, compared to women living in rural communities. The results from the audit of facilities show that pills, injectables and condoms were offered in all clinics that were visited and the IUD was offered in about 90% of the facilities. Family planning services were offered at least five days a week and nearly all facilities open between 0800 hours and 1630 hours. Most of the facilities had basic amenities such as water, electricity, and privacy for medical examinations. Many of the providers of family planning services were nursing sisters or nursing assistants and all were females. Nearly one third of the providers received no formal training specifically on the provision of family planning methods. However, about 77% of all the providers had attended in-service training in family planning provision in the ten years prior to the survey. Four variables, namely, the type of facility, availability of maternal care or delivery services, availability of sterilization and provider bias were significant. These are presented in Table 3. It should be mentioned that, after the inclusion of the community variables, the following individual level variables remained significant: the number of living children, age, educational level and partner’s education and work status. Marital status, however, became insignificant indicating that the observed differences in contraceptive use by marital status could be explained by the community factors, that is, the distribution of women by marital status may be different in different communities. A similar pattern of contraceptive use by community level variables as presented in the preliminary analysis is evident from Table 3. Women who live in communities served by LPPA clinics have the highest chances of using contraceptive methods but are not significantly different from those who have access to both LPPA clinics and hospitals. The odds of using contraceptive methods for women living in communities served exclusively by hospitals are nearly half those of women living in communities served by both LPPA clinics and hospitals. Women living in communities served by both LPPA and hospitals are mostly urban women and therefore have easier access to family planning services. Availability of maternal care services in facilities reduces the odds of using contraceptive methods. Women who live in communities where there are no maternal care services are twice as likely to use contraceptive methods as those who live in communities where the facilities provide maternal care services. The World Bank (1994) argued that where family planning services are offered as an integral part of maternal and child health and family planning (MCH/FP) in Lesotho, family planning often receives inadequate attention, partly because of the shortage of staff and the emphasis put on curative functions by the clinics. This also became evident in the focus group discussions when one woman indicated that:
In addition the World Bank (1994) regarded LPPA as having relatively greater experience in proper counseling of clients which improves quality and reduces drop-outs as it is able to draw on the more extensive experience of the IPPF and generally follows its procedures. Women who live in communities where sterilization is offered are more likely to use contraception than those who live in communities where it is not offered. Facilities that provide female sterilization offer all other methods of contraception available in Lesotho, except vasectomy and diaphragm. Therefore, it can be concluded that facilities that offer sterilization give women a wider choice of contraceptive methods that encourages their adoption and continuation, as they are able to meet the needs of different women. Women living in communities where providers indicated that there were no contraceptive methods that they would never recommend but left the choice of contraceptive methods to their clients’ preference, had the highest average odds of using contraceptive methods. Removing unnecessary medical requirements to using family planning safely and effectively can improve access (Robey et al., 1994). Bertrand et al. (1995) discussed access, quality and medical barriers in family planning programs. They suggested that to maintain quality standards, tests and procedures that are medically justified in family planning should be retained and strengthened but those, which are not medically justified, should be eliminated. This is a characteristic of the better facilities. For example, it was clear from the focus group discussions that some providers do not offer certain methods without any justification:
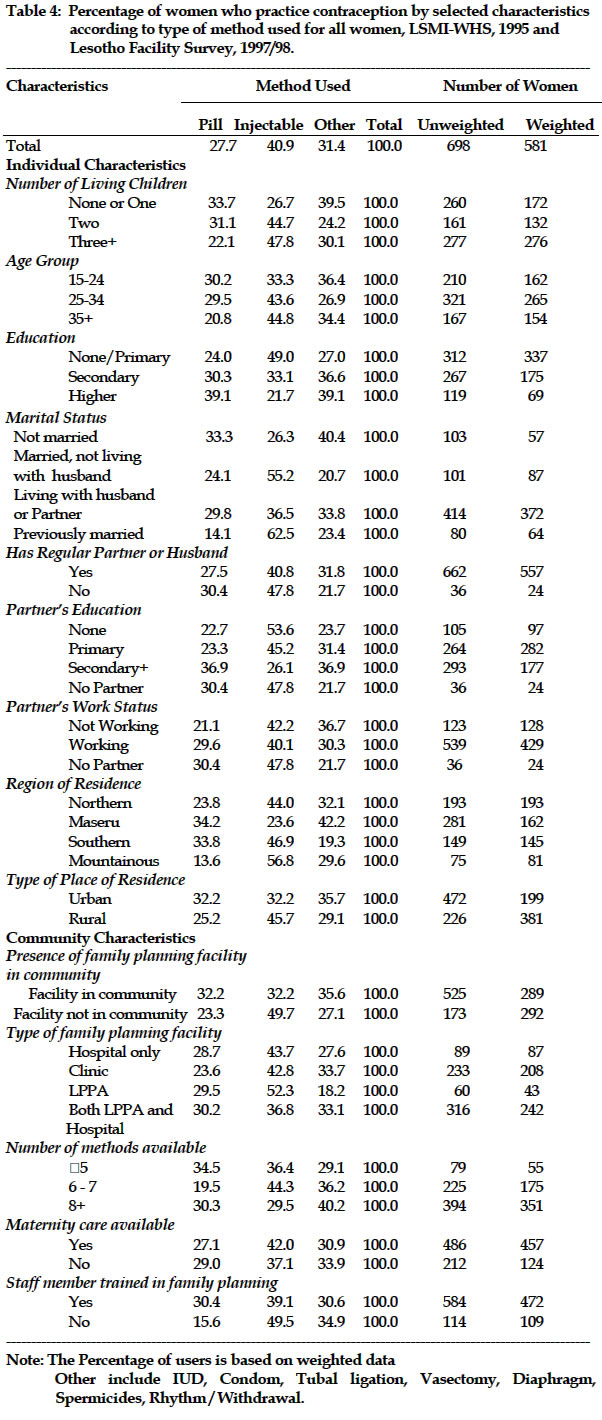
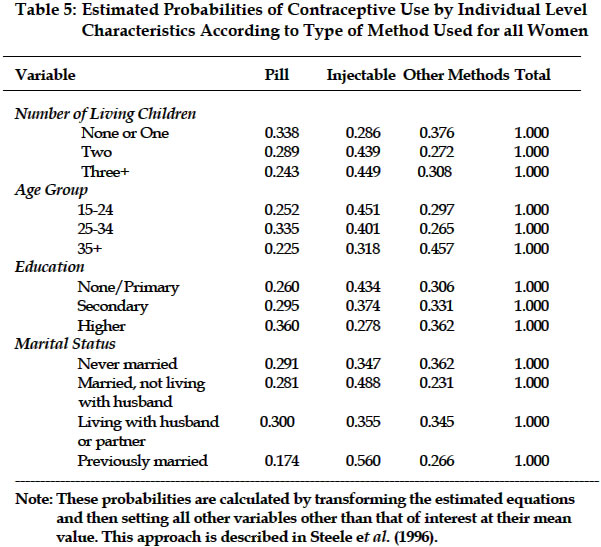
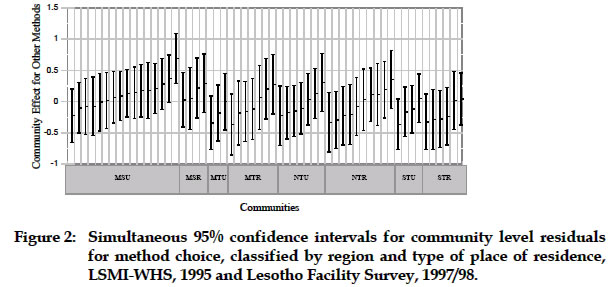
The community variance, which was significant in the model with the individual characteristics only, was reduced to zero when community level variables were included in the model. This suggests that the differences in the odds of using contraception between women living in different communities are mainly due to the different types of facilities available in communities, availability or non-availability of maternal care services, provision of sterilization and provider bias. While individual factors largely explain the variation in contraceptive use within communities, community factors explain the variation in contraceptive use between communities. Contraceptive method choice It is known that a good contraceptive method mix is a characteristic of successful family planning programs and that knowing what affects the choice of methods is useful in guiding the motivational and service provision aspects of the program (Bulatao, et al., 1989). Therefore, it is important to study the factors that affect method choice in Lesotho. Preliminary Results Table 4 shows the Percentage of women who currently practice contraception by selected socio-demographic and community level characteristics according to type of method used. Two methods are particularly common: injectables, used by 41% and pills, used by 28% of all users. All other methods (Intrauterine device, condoms, female sterilization, vasectomy, diaphragm, spermicides, withdrawal, abstinence and other methods) are aggregated as there are relatively few cases for each method. The IUD (10.2%) and condom (9.7%), however, represent relatively higher Percentages of users compared to the other methods but the number is still too small for them to be considered separately. Female sterilization and vasectomy were used by 2.4% of current users; diaphragm and spermicides by 1.2%; rhythm and withdrawal represents 5% of current users; and the remaining Percentage represents other traditional methods. The popularity of injectables and pills in Lesotho is comparable to other countries in southern Africa. In the family planning program of the Republic of South Africa, injectables are relatively more important. For example, a study of 2,290 women aged 15-49 in Transkei (sub region of South Africa) in 1994 revealed that 58.1% of current users were using injectables and 28.9% were using pills (Chimere-Dan, 1996). The popularity of the injectables is also evident in Malawi where they formed 41.0% of all current users in the Queen Elizabeth Central Teaching Hospital in Blantyre in 1993 (Lema et al., 1994). As one would expect, a woman the number of living children has and her age influences the type of contraceptive method she chooses. A positive relationship is observed between number of living children and the use of injectables whereas the Percentage of women choosing pills decreases as the number of living children increases. In the case of age, injectables are the widely used methods by women aged 25 and above of whom more than 40% use them. Younger women use other methods more. Pills are used less by women aged 35 and above. Education is also observed to influence the type of method a woman chooses. There is an increase in the Percentage of women who choose the pill and other methods as the educational level of women increases while the reverse is true for injectables which is used less as educational levels increase. This tends to be the case even in the case of partner’s education. The majority of women with none or primary education and of those whose partners have none or primary education tend to use injectables while the majority of those with higher education and of those whose partners have higher education tend to choose the pill or other methods. Injectables are the most widely used method for married women who are not living with their husbands and for previously married women of whom more than 50% use them. Women who are not married and those who are living with their husbands/partners use the other methods more. Place and region of residence are also observed to have an influence on the choice of contraceptive method used. The majority of women living in the northern, southern and mountainous parts of the country tend to use injectables whereas women living in Maseru are more likely to use other methods. In the case of type of place of residence, a higher Percentage of women in the rural areas choose injectables while those in the urban areas seem to be distributed almost evenly for the different methods. There are also differences observed in method choice by the family planning environment in which a woman resides. Women who live in communities where there is a facility that offers family planning tend to use other methods and the choice between the pills and injectables is the same. Almost half of those who live in communities without a family planning clinic use injectables. There are no differences in the choice of family planning methods by the type of service delivery point. In communities where a staff member has not trained specifically in family planning there is low use of the pill. This is also the case where there are between five and six methods of family planning methods available to women. The use of other methods increases as the number of available methods increases. Multinomial Logistic Regression Results As with contraceptive use, multivariate analyses are essential to assess the relative importance of each variable while controlling for the others. In this case a multilevel multinomial logistic regression was undertaken with the predictors listed in Table 4. The socio-demographic factors that were found to influence the choice of contraceptive method significantly are age, number of living children, education and marital status. For ease of interpretation of the parameter estimates, the probabilities of choosing a particular method are estimated and these are shown in Table 5. The choice of a particular method varies noticeably by age and the pattern is not similar to that observed in the preliminary analysis. This pattern changes possibly because of controlling for the number of living children since older women are the ones who would have more children. The probability of using injectables decreases steadily with age while the probabilities of using other methods are broadly similar for women aged less than 35 though increasing sharply at older ages. The use of the pill has an inverted U-shape pattern with age. Injectables are the most popular method chosen by women aged less than 35 while other methods are popular for those aged 35 and above. The high probability of choosing other methods by older women may be associated with a high use of IUD and tubal ligation, which are very popular among older women, as they tend to use contraception for limiting purposes. Similarly, the high probability of women aged 25-34 choosing injectables or pills may be because they use contraception for spacing and as such, a reversible method would be most appropriate. The high probability of using injectables for young women may be associated with the fact that these women may have difficulty in complying with method use requirements such as taking a pill daily or using a condom in which case a more lasting or non-intercourse related method would be ideal. In addition, injectables offer a large degree of secrecy as no one else can tell if a woman is using it. For the young women who were using injectables in the focus group discussions, this was cited as one of the reasons for choosing injectables over other methods:
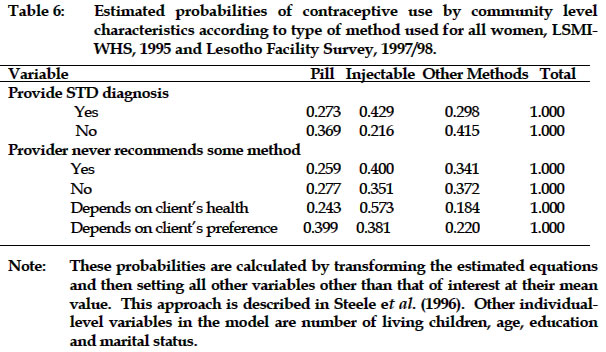
However, other evidence from the facility survey and the focus group discussions showed that some providers do not encourage injectables for young women. More than a third of the providers said they do not give an injectable to women less than 20 years of age. The number of living children a woman has also influences her choice of contraceptive method. The probability of choosing injectables increases as the number of living children a woman has increases, with a steep increase observed from none or one child to two children. The probability of choosing the pill decreases steadily as the number of living children increases. The use of other methods is popular for women with one or no children while injectables are popular for those with two or more children. This can possibly be explained by the fact that women with more children tend to prefer more permanent and less cumbersome methods as their main reason for using contraception tends to be more towards limiting. The probability of choosing injectables is minimal (less than 20%) for women with no children and this could be due to the possible reluctance of these women to opt for a method which may delay the return of fertility (which is on average 10 months from the date of last injection with Depo-Provera (WHO, 1996), the widely offered type of injectable in Lesotho). Also, it is evident from the focus group discussions that some providers do not provide injectables to women with no children:
In the case of education, it is observed that the probability of choosing a particular method of contraception varies, particularly for women with none/primary education and for those with post-secondary education. As educational level increases, so does the probability of choosing the pill and other methods with wide differences between the two methods at lower levels of education, which narrows at higher levels. The probability of using injectables, however, decreases with increasing education. The decreasing probability of using injectables as education increases may be explained by the fact that educated women may be more worried about the possible harmful side effects of injectables which less educated women may not be aware of. Considering marital status, choice of contraceptive method seems to differ across all the methods in the different categories. The probability of choosing injectables is highest for married women who are not living with their husbands or partners and previously married ones. For women living with their partners and those never married, the choice seems to be almost the same for each of the three methods. Previously married women are less likely to choose the pill. The high probabilities of choosing injectables for married women not living with their husbands may imply that these women opt for methods that offer a high level of secrecy given the fact that their husbands may be against the use of contraception. In the situation of previously married women, methods which are highly effective and also offering some level of secrecy may seem more appropriate as they are, culturally, not expected to have children let alone being sexually active explaining the high reliance on injectables for these women. As well as looking at the individual level differences that affect the choice of a particular method over others, community level differences are also considered. The community variance for the difference between other methods and injectables (reference category) is significant at a level of 10% (estimate = 0.150 and standard error= 0.082) but that for the pill was zero. This indicates that there is no variation at community level between the choice of pill over injectable whereas some significant difference is observed between the choice of other methods over injectables. Thus, after controlling for socio-demographic factors of individual women, there is no real variation in the decision to use pills as opposed to injectables whereas there are differences observed in the choice between injectables and other methods and, implicitly, differences between pills and other methods. Simultaneous confidence intervals have also been constructed in this section to allow for multiple comparisons between communities. It is only sensible to do this for the difference between injectables and other methods whose community effect was significant at 10% level. If the 95% confidence intervals overlap for any communities, then there is no evidence, at the 5% level, that there is some difference in the rate of choosing other methods over pill. Figure 1 shows the estimated community level effects for the difference between the choice of other methods over injectable when individual level characteristics are controlled. It is clear that there is no difference in the rate of choosing other methods over injectables between different communities in the same region as indicated by the overlapping confidence intervals in each region. There is, though not very pronounced, some differences observed in the rate of choosing other methods over injectables between communities in Maseru and those in the Mountains. Whereas no apparent difference is observed between all other regions or specifically, all other communities, as the confidence intervals seem to overlap. This may reflect uneven availability of contraceptive methods in some regions, particularly between Maseru and mountainous areas. Community level variables were included to establish if the family planning environment in which a woman lives could affect her choice of contraceptive method. Two provider variables are found to be significant in influencing method choice, net of the demographic and social factors of the women and these are whether or not the service provider diagnoses sexually transmitted diseases (STDs) and whether or not there are any methods she would not recommend under any circumstances. The results are given in Table 6. It should also be noted that all the individual factors significant in the individual level model remained significant after including community factors and that the random parameter becomes zero, which shows that the community variables included together explain all the variation observed at the community level. Women who live in communities where providers indicated that they did not provide STD diagnosis have a higher probability of choosing the pill and other methods and less of injectables. The reverse is true for women who live in communities where providers said they provided STD diagnosis. The providers who offer STD diagnosis in Lesotho are normally highly qualified nurses, such as nurse clinicians and nursing sisters who may have more tasks to do and as such, administering injectables would be a lot easier than administering the pill or other methods. Those who do not provide an STD diagnosis, or who are less qualified, may be more comfortable providing pills as even non-medical providers can safely offer oral contraceptives, unlike injectables where a person needs to be trained to give injections and to handle needles and syringes properly. Providers were asked if there were any contraceptive methods they would never recommend under any circumstances, followed by a question on which methods they would never recommend. However, the different methods, which they said they would not recommend under any circumstances, were not significant. Women who live in communities where providers said they consider client’s health before recommending any method have a high probability of using the injectables. This may possibly be because providers may be avoiding the risks of estrogen-related complications contained in combined pills. In addition, providers may prefer injectables as there is little client involvement and they are therefore regarded as very effective. The latter reason also explains the high use of the injectables for women living in communities where providers mentioned some methods of family planning that would never be recommended under any circumstance. About 14% of all providers said they would never recommend natural family planning since they regarded it as ineffective. In summary, contraceptive method choice in Lesotho is affected by both individual and community factors. Similar to the analysis of contraceptive use, individual factors explain the variation in method choice within communities while community factors mainly explain the variation in method choice between communities. SUMMARY AND CONCLUSIONSThis study has shown that the decision to use and to choose a particular method of contraception is a function of both individual and community characteristics. Only 29% of women exposed to the risk of conception use contraception. This low use of contraception may have serious implications for the fertility rate of Lesotho that has been kept low by the effect of migrant labor; Mpiti and Kalule-Sabiti (1985) asserted that if a substantial drop in labor migration occurs, there might be an increase in fertility if this is not accompanied by greater use of contraception. At the individual level, young women who are sexually active (representing 17% of the teenagers) are observed to have particularly low contraceptive usage in Lesotho and this may suggest a high risk of teenage pregnancies. This has serious implications for the increase in the growth rate, which the government wishes to lower. Early childbearing directly influences population momentum, a key factor in high growth rates. Therefore, there is need to reach young people with information about responsible sexuality and the potential consequences of sexual activity. This can be achieved by interventions that provide negotiation skills, for example, skills for resisting peer pressure to engage in unwanted sexual activity. In addition, a relationship has been observed between contraceptive use and education. Women with primary or no education, who form the great majority of the women (63%), are about 50% less likely to use contraception as those with secondary education. This group of women need special attention for the promotion of family planning services. The partner’s education and work status is also important; where the husband or partner is not or less educated and where the husband or partner is not working contraceptive use is less. Reaching people with information about family planning through communication campaigns can create awareness of family planning and promote information about modern contraceptive methods. Both mass media and interpersonal communication can inform people about the choices they have. The World Bank (1994) has identified intrinsic strengths that Lesotho possesses which should make it possible to organize educational campaigns. These include the homogeneity of the population and the wide access to the radio. This paper has also shown clearly that the delivery of family planning services is also important for the adoption or continuation of contraception. Women who live in communities served by LPPA have higher contraceptive use. The World Bank (1994) regarded LPPA as having comparatively greater experience with counseling of clients that improves quality and reduces dropout. It suggested that the MOHSW should co-ordinate more closely with LPPA because LPPA is able to draw on the more extensive experience of the International Planned Parenthood Federation and generally follows its procedures, which have proven to be effective. This may also suggest that LPPA should establish clinics in the rural areas as well as in the other two districts in the mountainous region. In addition, family planning in facilities that offer family planning as an integral part of the MCH/FP should be given enough attention to attract and maintain its contraceptive clientele. Finally, the effect of the family planning providers has been identified as an important element in influencing contraceptive use and method choice, together with the services they offer. The bias of providers is important in both use and choice of methods and explain largely the difference observed between communities. It is important to recognize that, as Kwan (1994) indicated, the degree of satisfaction and the acceptance of services by the clients depend very much on the attitude and the competence of service providers. REFERENCES
Copyright 2003 - Union for African Population Studies The following images related to this document are available:Photo images[ep03013f1.jpg] [ep03013t6.jpg] [ep03013t2.jpg] [ep03013f2.jpg] [ep03013t5.jpg] [ep03013t4.jpg] [ep03013t3.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}