 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
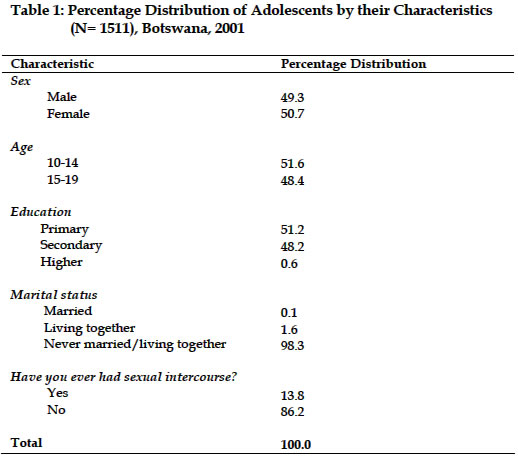
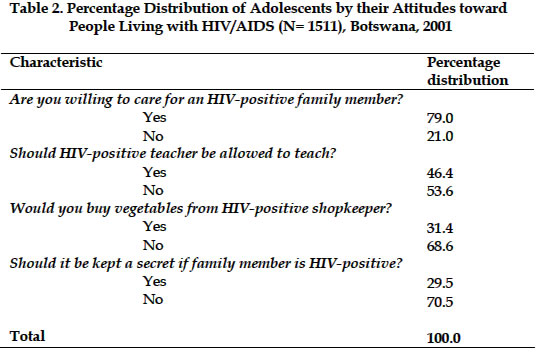
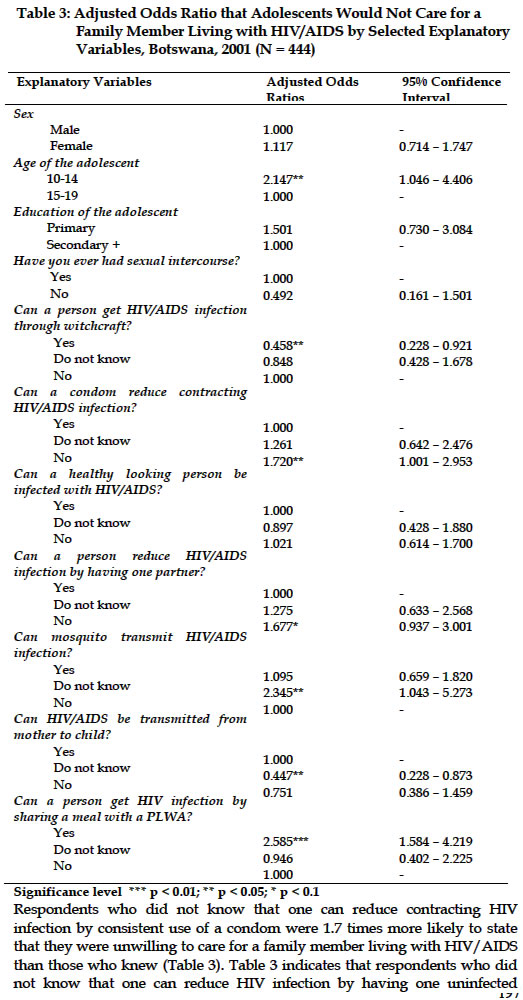
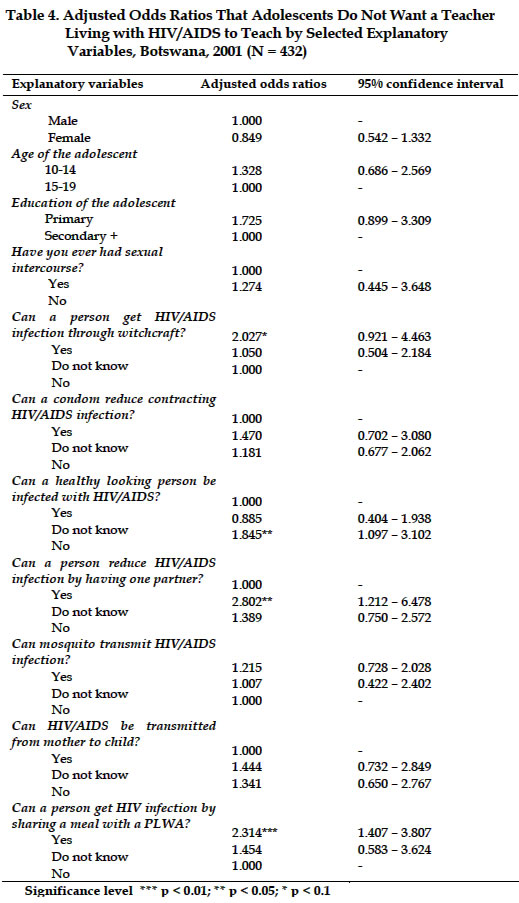
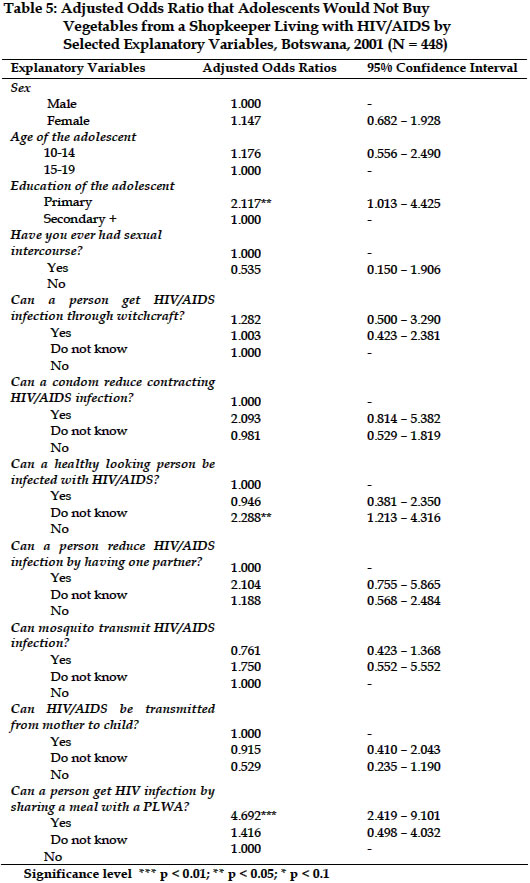
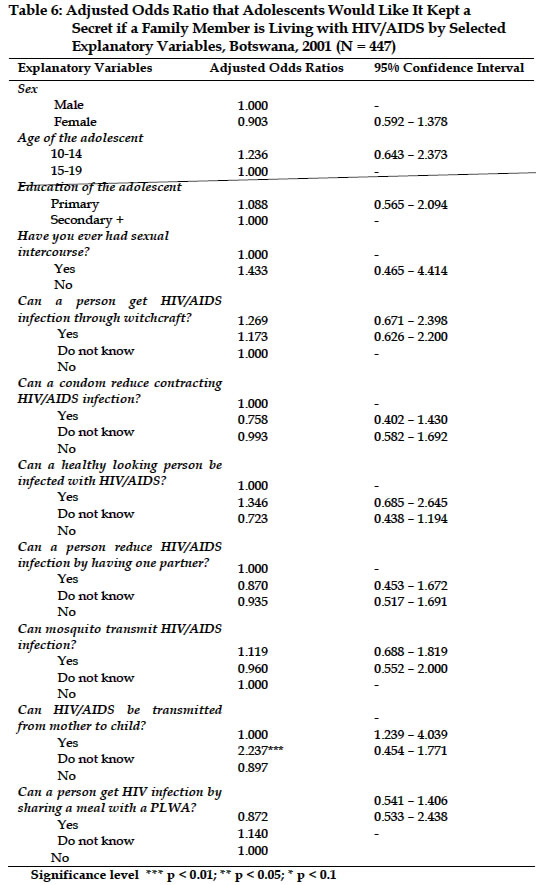
African Population Studies/Etude de la Population Africaine, Vol. 19, No. 2, August 2004, pp. 191-204 HIV/AIDS-Related Stigma and Discrimination among Adolescents in Botswana Gobopamang Letamo[1], PhD Department of Population Studies, University of Botswana, Gaborone, Botswana Code Number: ep04018 ABSTRACT The primary goal of this study is to examine and determine factors influencing stigmatisation and discrimination among adolescents towards people living with HIV/AIDS in Botswana. HIV/AIDS-related stigma and discrimination result from fear, ignorance, and denial. There exists little or no research in Botswana dealing with how people living with HIV/AIDS or suspected of having HIV/AIDS are perceived and treated. Data analysed in this paper are taken from the Botswana AIDS Impact Survey conducted in the year 2001. Both descriptive and multivariate logistic regression models are used to analyse the data. The results show that many of the adolescents expressed negative attitudes towards people living with HIV/AIDS. Logistic regression analysis shows that misconceptions about HIV transmission often encourage stigmatisation and discrimination of people living with HIV/AIDS. Interestingly, although the majority of the adolescents stigmatise and discriminate against PLWA, many of them are willing to care for a family member who has HIV/AIDS. There is need to address issues of stigma and discrimination as part of prevention of further spread of HIV/AIDS in Botswana. INTRODUCTION Right from the beginning, the HIV/AIDS epidemic has been accompanied by an epidemic of fear, ignorance, and denial, leading to stigmatisation of and discrimination against people with HIV/AIDS and their family members (International Center for Research on Women, 2002). HIV/AIDS-related stigma and the resulting discriminatory acts create circumstances that fuel the spread of HIV (Busza, 1999). The fear of being identified with HIV prevents people from learning their sero-status, changing unsafe behaviour, and caring for people living with HIV/AIDS. A study in Botswana and Zambia found that stigma against HIV-positive people and fear of mistreatment prevented people from participating in voluntary counselling and testing and programmes to prevent mother-to-child transmission (Nyblade and Field, 2000). The authors argued that stigma and its resulting discrimination also intensifies the pain and suffering of both the people living with HIV/AIDS and their families. There exists little or no research in Botswana dealing with how people living with HIV/AIDS (PLWA) or suspected of having HIV/AIDS are perceived and treated because of their illness. However, it is quite evident from studies done elsewhere that PLWA are unfairly treated and/or discriminated against because of their actual or suspected HIV/AIDS status (Aggleton, 2000; Busza, 1999; International Center for Research On Women, 2002; Gilmore and Somerville, 1994; Goldin, 1994). Discrimination against people living with or suspected of having HIV/AIDS, apart from denying them their basic rights, is also an ineffective public health measure. It should be noted that at the on-set of HIV/AIDS epidemic, the disease was mainly found among groups who are already socially marginalised and discriminated against. These groups included homosexuals, injection drug users, and commercial sex workers. To anybody belonging to these groups, HIV/AIDS means additional stigmatisation whether or not they are infected. People living with HIV/AIDS may become implicitly associated with stigmatised behaviours, regardless of how they actually became infected. The stigmatised find themselves ostracised, rejected, and shunned and may experience sanctions, harassment, and even violence based on their infection or association with HIV/AIDS. Discrimination may stem from fears due to lack of knowledge about how HIV/AIDS can or cannot be transmitted. Since discrimination often includes public restrictions and some forms of punishment, it can be more frequently identified (Busza, 1999). Stigma is often rooted in social attitudes. In this study, social attitudes’ variables are used to investigate HIV/AIDS-related stigma and discrimination among adolescents in Botswana. Individuals with HIV and AIDS are stigmatised because their illness is: (i) associated with deviant behaviour; (ii) viewed as the responsibility of the individual; (iii) tainted by a religious belief as to its immorality and/or thought to be contracted via a morally unsanctioned behaviour and, therefore, thought to represent a character blemish; (iv) perceived to be contagious and threatening to the community; (v) associated with an undesirable and an unaesthetic form of death; and (vi) not well understood by the lay community and viewed negatively by health care providers (Alonzo and Reynolds, 1995). The present paper adopts a similar framework in studying factors influencing stigmatisation and discrimination against PLWA among adolescents in Botswana. Variables that reflect knowledge and misconceptions about HIV transmission and those that show the socio-economic and demographic profile of individuals are used as predictors of stigma and discrimination. The primary goal of this study is to examine and determine the attitudes and perceptions of adolescents towards PLWA with a view to suggest how such stigma and discrimination can be mitigated. Specifically, the paper addresses two main objectives. First, it measures the attitudes of adolescents towards people living with HIV/AIDS. That is, whether or not adolescents are willing to care for a family member who is ill with HIV/AIDS; whether an HIV positive teacher should or should not be allowed to continue teaching; whether or not they would buy food or vegetables from an HIV positive shopkeeper; and whether or not it should remain a secret if a family member got infected with HIV/AIDS. Second, it examines the factors (social, economic and demographic) that are associated with negative attitudes toward people living with HIV/AIDS. The high prevalence of HIV/AIDS in Africa as reflected in the statistics makes this study particularly important. MATERIALS AND METHODS The data analysed in this paper are taken from the Botswana AIDS Impact Survey (BAIS) conducted in 2001. Sample selection was done in two stages. First, 98 enumeration areas were selected with probability proportional to measures of size, where measures of size are the number of households in the enumeration area. Second, the households were systematically selected from a fresh list of occupied households prepared at the beginning of the survey’s fieldwork, i.e. listing of households for the selected enumeration areas. Overall, 2000 valid households were drawn systematically. The questionnaires for the BAIS study were based on the UNAIDS Model Questionnaire with some modifications and additions. Some of the modifications include lowering the age limit of eligible persons to 10 years and increasing the upper limit to 64 years. Two questionnaires were administered in the survey: the household questionnaire and an individual questionnaire for men and women aged 10-64 years. Respondents who did not complete the questionnaire, and those who were not adolescents, were excluded from the present analysis. The data quality is believed to be high because of a number of reasons. First, the interviewers were thoroughly trained for 2 weeks. Second, there was close supervision of the interviewers during the data collection stage. Third, questionnaires were thoroughly edited to ensure that relevant questions have been responded to and coded according to the codes designed for the study. Fourth, the data were checked for consistency with the aid of the Computer Edit Specifications designed by the subject matter specialist. Finally, the household response rate was 88% (90.3% in rural areas and 85.8% in urban areas) whilst the individual response rate was 95.1% (Central Statistics Office, 2002). Definitions of Stigma and Discrimination Stigma generally refers to a negatively perceived defining characteristic, either tangible or intangible (Busza, 1999). Several authors had divided stigma into felt or perceived stigma and enacted stigma (Gilmore and Somerville, 1994). Felt stigma refers to real or imagined fear of societal attitudes and potential discrimination arising from a particular undesirable attribute, disease (such as AIDS) or association with a particular group. Enacted stigma, on the other hand, refers to the real experience of discrimination. Regarding HIV/AIDS, it may be actual infection or based on behaviours believed to lead to infection. Stigma is most frequently associated with diseases that have severe, disfiguring, incurable, and progressive outcomes, especially when modes of transmission are perceived to be under the control of individual behaviour (Gilmore and Somerville, 1994). It is also common in diseases that are perceived to result from the transgression of social norms, such as socially sanctioned sexual activity (Gilmore and Somerville, 1994). Stigmatisation often leads to discrimination, which refers to any form of distinction, exclusion, or restriction affecting a person by virtue of a personal characteristic (International Center for Research On Women, 2002). Ignorance and fear are said to underlie HIV-related stigma. Inadequate understanding of the modes of HIV transmission leads to fear of transmission from casual contact (International Center for Research On Women, 2002). Through stigma, society often blames infected people for being ill and justifies discriminatory acts against them while asserting innocence and health of those who stigmatise (UNAIDS, 1999). For the purpose of this study, stigma and discrimination are conceptualised as negative attitudes toward people living with HIV/AIDS. Measurement of Stigma and Discrimination One of the most difficult issues facing researchers working in the area of stigma and discrimination is that of measurement. Stigma and discrimination are measured here by assessing negative attitudes toward persons living with HIV/AIDS. For instance, respondents who report that they do not want an HIV-positive teacher to continue teaching even though he is not sick exhibit distinction, exclusion or restriction against persons with HIV/AIDS. The reason for not allowing the teacher to continue teaching is based on the teacher’s sero-status. Methods Both descriptive and multivariate analyses were conducted. Logistic regression analysis is used to evaluate the effect of a select group of predictor variables on the probability of expressing negative attitudes toward PLWA, while controlling for other variables in the model. Logistic regression method was used because it provides an interpretable linear model for a categorical dependent variable. It also allows for the testing of the significance of a given predictor whilst controlling for all other predictors in the model (Agresti and Finlay, 1986). Separate logistic regression models were used to evaluate the effects of individual factors on the probability of expressing negative attitudes toward PLWA. For the ith individual, the model could be expressed as: ln PI / (1-Pi) = ß0 + åß kxki where PI is the probability that the ith adolescent will express negative attitudes toward PLWA, 1-Pi is the probability that the ith adolescent will not express negative attitudes toward PLWA, ß0 is the baseline constant, xki is an array of (k) independent variables, and ß is the corresponding vector of unknown regression coefficients (Agresti and Finlay, 1986; Hosmer and Lemeshow, 1989). The SPSS-PC logistic programme was used to estimate regression coefficients through the maximum likelihood procedure, together with confidence intervals for the estimates. Results Sample Characteristics The interviewed adolescents’ ages ranged from 10 to 19 years, with a mean age of 16. The ratio of males to females was virtually similar, 50.7% compared to 49.3%. The population of the adolescents used for analysis was slightly skewed towards those aged 10-14 years (Table 1). By virtue of their age, the majority of adolescents had either primary or secondary education (99 percent) and were predominantly unmarried (98 percent). Another interesting observation is that 86 percent of adolescent reported that they have never had sexual intercourse. Descriptive Statistics The majority of adolescents (68.6%) indicated that they would not buy vegetables from an HIV/AIDS patient (Table 2). The next most popular HIV/AIDS-related stigma and discrimination among adolescents was towards a teacher who is HIV-positive but not sick with AIDS. About 54 percent of the adolescents argue that an HIV-positive teacher should not be allowed to teach even though he or she may not be sick. Almost four-fifths of adolescents stated that they would be willing to care for a family member sick with HIV/AIDS. A related but different observation is that about 30 percent of adolescents reported that it should be kept a secret if a family member is sick with HIV/AIDS. The next section examines factors influencing negative attitudes of adolescents toward people living with HIV/AIDS. Multivariate Analysis of Discriminatory Attitudes of Adolescents toward HIV/AIDS Patients The betas represent the change in the log odds due to the unit increments in the values of the predictors (DeMaris, 1992). eß is a summary statistic for the partial effect of a given predictor on the odds, controlling for other predictors in the model. Tables 3, 4, 5 and 6 show the results of multivariate analysis models predicting the relative odds of adolescents expressing discriminatory attitudes toward HIV/AIDS victims. In addition to the relative odds, 95% confidence intervals are also shown in the tables. Respondents who did not know that one can reduce contracting HIV infection by consistent use of a condom were 1.7 times more likely to state that they were unwilling to care for a family member living with HIV/AIDS than those who knew (Table 3). Table 3 indicates that respondents who did not know that one can reduce HIV infection by having one uninfected faithful sexual partner were 1.7 times more likely to state that they were willing to care for a family member living with HIV/AIDS than those who knew. All these relationships were statistically significant at 90% level. Respondents who believed that a person can get HIV infection by sharing a meal with a PLWA were almost three times more likely to say that they were unwilling to care for a family member living with HIV/AIDS than those who did not have this misconception. It is therefore evident that adolescents who lack understanding of modes of transmission were more likely to stigmatise and discriminate against people living with HIV/AIDS. Generally, respondents who had misconceptions about how HIV transmission were more likely than their counterparts to state that they were unwilling to care for a family member living with HIV/AIDS. Another noteworthy observation is that adolescents 10-14 years of age were 2 times more likely to state that they were unwilling to care for a family member living with HIV/AIDS than those who were 15-19 years. The sex and education of the respondent were not predictors of whether or not the adolescent was willing to care for a family member living with HIV/AIDS. Those who have misconceptions (those who believe that HIV/AIDS can be transmitted by sharing a meal with PLWA or can be contracted through witchcraft or mosquito) were more likely to express negative attitudes toward an HIV-positive teacher than those who had correct knowledge of HIV transmission. However, not all of the predictors are statistically significant. From Table 4, it can be observed that adolescents who believed that a person can get HIV infection by sharing a meal with a HIV/AIDS patient were 2.3 times more likely than their counterparts to stigmatise and discriminate against a teacher who has HIV/AIDS. This relationship was statistically significant at 99% level. Another observation is that adolescents who did not believe that a healthy looking person can be infected with HIV were almost 2 times more likely than their counterparts to have a negative attitude towards an HIV-positive teacher. It is also interesting to note that adolescents who believed that a person can get HIV/AIDS through witchcraft were twice more likely than their counterparts to have a negative attitudes toward a teacher who is HIV-positive. It appears again that lack of knowledge of how HIV/AIDS can be transmitted is an important predictor of discriminatory attitudes among adolescents towards people living with HIV/AIDS. Adolescents with primary education were 2 times more likely than those with secondary or above education to state that they would not buy vegetables from a shopkeeper living with HIV/AIDS (Table 5). Adolescents who believed that a healthy looking person can be infected with HIV/AIDS were twice more likely than their counterparts to discriminate against a shopkeeper living with HIV/AIDS. From Table 5, it can be observed that adolescents who believed that a person can get HIV infection by sharing a meal with a HIV/AIDS patient were 5 times more likely than their counterparts to indicate that they would not buy vegetables from a shopkeeper living with HIV/AIDS. This relationship was statistically significant at 99% level. As to whether or not adolescent would like it kept a secret if a family member became ill with HIV/AIDS, none of the independent variables was statistically significant (Table 6), reflecting, perhaps the hypothetical nature of the question. DISCUSSION HIV/AIDS-related stigma and discrimination are a serious public health problem not only in Botswana but also internationally. The purpose of this study was to examine the factors influencing stigma and discrimination related to HIV/AIDS among adolescents and to suggest ways of mitigating the impact created by such practices. The results clearly showed that HIV/AIDS-related stigma and discrimination are rampant in Botswana. One important finding is that although many of the respondents stigmatise and discriminate against HIV/AIDS patients (a teacher or shopkeeper who is sick with HIV/AIDS), a substantial proportion of them are willing to care for a family member sick with HIV/AIDS. This probably reflects that no matter how stigmatised the disease is, people are willing to make sacrifice in order to care for their close relatives. It is possible that the hypothetical teacher or shopkeeper who is sick with HIV/AIDS is not imagined to be a family member but a distant person. One may conclude that people are more likely to discriminate against HIV/AIDS patients who are not close relatives. Misconceptions about how HIV infection may be transmitted tend to promote negative attitudes towards PLWA. Consistently, respondents who believed that HIV infection can be transmitted through witchcraft or sharing a meal with a PLWA were significantly more likely to stigmatise and discriminate against PLWA than other people. This might be indicative of the fact that negative response and attitudes towards PLWA are strongly linked to general levels of knowledge about HIV and AIDS and, in particular, to the causes of AIDS and routes of HIV transmission (Bharat, Aggleton and Tyrer 2001). In other words, the perception of how HIV/AIDS was acquired is critically important on how people will treat a PLWA. The results also show that regardless of intensive public campaigns relating to various aspects of HIV/AIDS, including its transmission, the messages have not quite reached a large majority of people in the country. The Information, Education, and Communication campaigns on HIV/AIDS need to be intensified to dispel some of the prevailing misconceptions about HIV/AIDS transmission. There is clearly a need for a qualitative study on stigma, discrimination, and associated factors so that mitigating strategies that effectively deal with these issues are designed and implemented. REFERENCES
[1] Acknowledgement: The author wishes to express gratitude to the Central Statistics Office in the Ministry of Finance and Development Planning for allowing him permission to use the Botswana AIDS Impact Survey data. Copyright 2004 - Union for African Population Studies The following images related to this document are available:Photo images[ep04018t6.jpg] [ep04018t1.jpg] [ep04018t4.jpg] [ep04018t5.jpg] [ep04018t2.jpg] [ep04018t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}