 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
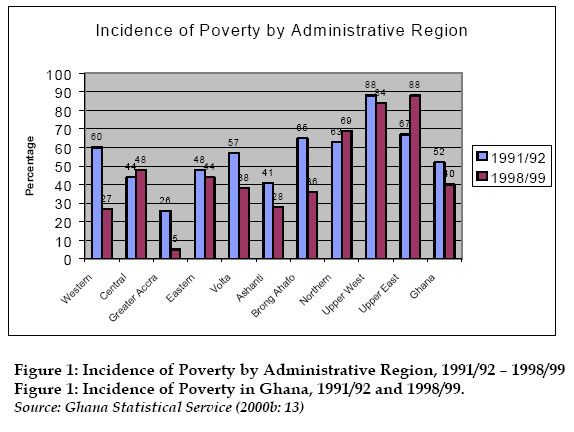
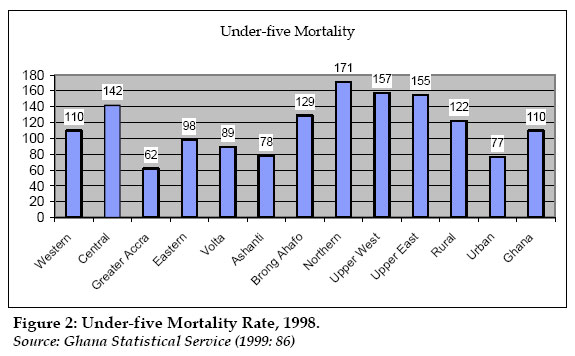
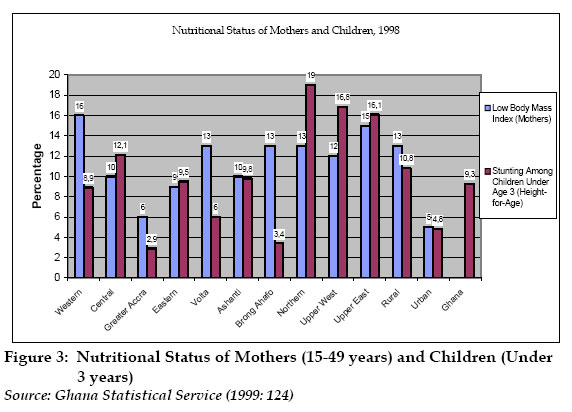
African Population Studies/Etude de la Population Africaine, Vol. 19, No. 2, Sup. A, 2004, pp.285-302 Implementation of Ghana’s Health User Fee Policy and the Exemption of the Poor: Problems and Prospects Delali Margaret Badasu Institute of African Studies University of Ghana[1] Code Number: ep04031 Abstract Like many other African countries, Ghana has been implementing a cost-sharing policy in its health sector since the 1990s. The adoption of this policy and the consequent charging of user fees for health services was due to stagnating economies and associated budgetary constraints and increasing gaps between supply and demand for basic social services that have been characteristic of African countries since the 1970s. The main objectives for the adoption of cost-sharing policies have been to improve both quality and access to health services. Studies focusing on the experience of African countries with the implementation of user fees indicate varying findings on the impact of user fees on their health delivery systems. The access of the poor, in particular, has been adversely affected, according to the findings of a number of studies. Policies, such as targeting the poor, have not been effectively implemented to mitigate the impacts of the user fee policy on their access. This paper examines the problems associated with granting exemption to the poor in Ghana. It also discusses the prospects of considering the poor in alternative policies that may be adopted in future. Its main findings indicate that a number of shortcomings of policy adoption, particularly the lack of specification of criteria by which the poor can be identified, make it difficult for health workers to grant exemptions. Further findings show that declining government budget allocations and supplies might have made it imperative for the facility manager to be more concerned about collecting revenue than attending to financial access of the poor. The study, however, suggests that despite the shortcomings of the targeting policy and its implementation, it should continue to be an important component of health policy, considering the vast inequalities in income in the population. Introduction Stagnating economies and associated budgetary constraints and increasing gaps between supply and demand for basic social services have been characteristic of African countries since the 1970s. In the 1980s, many of these countries adopted macroeconomic programmes, commonly referred to as Structural Adjustment Programmes (SAPs) as a response to the shattered economies (Audibert and Mathonnat, 2000:66). Some common features of the SAPs are liberalization of the economies and “gradual shift from direct state controls and regulation to greater reliance on market forces” and introduction of cost-sharing policies that require citizens to pay for social services such as education and health services (Botchwey, 1993:4). International sources of and/or support for the policies have also been recognized. For example, the 37th WHO Regional Committee held in BamakoMali in 1987, recognizing the financial inability of many African States to guarantee a minimum level of health care for their populations endorsed jointly with UNICEF a resolution, known as the Bamako Initiative, on a number of health issues for the African states. Some of the major objectives of the initiative were: to strengthen community participation and financing of health care services with decentralized management of community resources, to improve the availability of essential drugs and their rational use and to integrate all primary health care services, with special emphasis on maternal and child health services. Behind the initiative were the promising results of pilot programmes that were running in Benin and Guinea (Audibert and Mathonnat, 2000:66). The debate that ensued from the Bamako Initiative centred on the achievement of two of its major objectives: obtaining drugs and at lower cost at the health facilities and secondly, the ability of the population to pay for the drugs that would be available. There were also concerns about whether the pilot programmes in Benin and Guinea could be operated on national scale. However, some African states decided to adopt cost-sharing policies soon afterwards. Audibert and Mathonnat (2000:66) have observed that the Bamako Initiative inspired the introduction of user fees in the health sector of Mauritania in 1993. In Kenya, actions taken to implement user fee and targeted exemptions in 1989 were part of the IMF/World Bank programme (Wa Mbugua, 1993:13). In Ghana and Zimbabwe, the governments had to succumb to multilateral donors’ suggestion to effect a sudden implementation of user fees across all facilities and abandon a gradual phased implementation that was already underway (Russell, 1999:772). Some other international efforts that have influenced health policy in the developing world, including the African sub-region, must also be mentioned: the 1978 Alma-Ata Declaration of Health for All by the Year 2000 and the 1992 Dakar Consensus. The latter adopted a set of 13 Mid –Decade Goals (from the 1990-2000 Decade Goals set at the 1990 World Summit on Children) to meet the challenges of improving the lives of women and children. The Alma-Ata Declaration encouraged the promotion of basic health care and implementation of expanded immunization programmes in many developing countries, including Ghana since the 1970s. The Darkar Consensus has also served as a guiding principle for African governments in their devoting of more resources to maternal and child health. Studies focusing on the experience of African countries with implementing user fees policy indicate varying findings. Some show that availability of drugs has improved at some public health facilities (Audibert and Mathonnat (2000) on Mali, Chawla and Pellis (2000) on Niger). Others indicate that the financial access of the poor to health services has rather been adversely affected even though revenue generated has been considerable (Mackintosh and Tibandebage (2001) on Tanzania; Nyonator and Kutzin (1999), Waddington and Enyimayew (1989, 1990) on Ghana; Gilson and Mills (1995) several countries; Dlodlo (1995) on Zimbabwe). Thus the dual goal of maximizing quality gains through revenue collection and minimizing equity losses have not been realized in many countries which have implemented the health user fee policy. Recognizing the realities of the worsening economic conditions of their citizens, a number of African states, including Ghana, adopted policies to exempt the poor and other categories from paying user fees. Such policies aim at minimizing equity losses or reduced access of the poor to health facilities resulting from fee payments (Nyonator and Kuntzin, 1999:329-330; Dlodlo, 1995:1; Wa Mbugua, 1993:12). These and other safety net provisions, known as social dimensions of adjustment (SDA), have been implemented alongside the SAPs for specific groups of people who tended to be adversely affected by adjustment programmes. A typical group has been the “new poor” – people who lost their jobs as a consequence of cutbacks in public expenditure or layoffs in public enterprises to make the latter more efficient (Boer, 1993:10). Beneficiaries of SDAs have not always been the most absolute poor, those who were poor before and after introduction of SAPs and their related SDAs, as pointed out by Boer (1993:10 citing Green 1991: 16-17). Questioning the relevance of targeting of social expenditure to poverty alleviation in African states, Boer points out that the extent of this absolute poverty in the region suggests that targeting is not an important instrument for poverty alleviation. She notes again that SDAs seem to have been designed to sustain adjustment programmes by reducing their burden on government officials, the middle class and other politically influential people rather in many cases. (Boer 1993:10 citing Morrison 1992:36). Boer warns that donor inspired and supported targeted programmes are in danger of backfiring in future if domestic political support and financial commitment do not come forth as poverty among vulnerable categories may increase considerably in future. Notwithstanding such evidence and apprehension, the need to consider safety net provisions in health delivery in African countries such as Ghana cannot be overemphasized. The disproportionate burdens of disease among the poor and disparities in socioeconomic development among the countries and the current market-oriented policies being implemented lend support to this view. The argument by others who advocate adoption of comprehensive or integrated health policies in place of “crisis-led” measures (Boer, 1993; Wa Mbugua, 1993) is also important. Focusing on the Ghanaian situation, this paper examines the problems and prospects of exempting the poor under the health user fee policy. Specifically, it examines how the clause on exemption of the poor from paying user fees has been implemented and the problems associated with granting exemption to the poor. It suggests a number of long-term more effective policies for health delivery in the country. It also shows that targeting as a component of health policy is necessary, at least in the short term and recommends alternative more efficient and effective long-term policies for health delivery in Ghana. A number of secondary sources of data and information have been used. Three major studies on the implementation of the user fee have been examined. The studies were carried out between 1989 to 1999. Information on current user fee practices was collected from three hospitals in Accra, the capital of Ghana. The study has also cited some works on health reform and implementation of the user fee policy in other African countries. Conceptual Issues Targeting Targeting is a welfare concept and a strategy for identifying any group(s) of persons in a population who are eligible for an intervention or assistance. This usually arises from resource constraints or some distributive objectives that demand exclusion of some individuals from a programme/intervention so that it can have intended impact (Vos 2003, Grosh 1996:146-147). Resource constraints and efficiency objectives may require that those who have greatest need or can least afford access to the service in question be identified and provided for. Two errors often arise in targeting: 1. Error of exclusion: excluding those intended to benefit from a programme and 2. Error of inclusion: including those not intended to benefit from a programme. In programmes reaching the poor, for example, errors of exclusion arise from undercoverage of the poor for whom a programme is intended and errors of inclusion or leakage result when unintended nonpoor benefit from programmes or interventions that target only the poor (Cornia and Stewart 1993). Both errors render a programme/policy ineffective and must be minimised to achieve desired impacts. Several reasons account for the occurrence of both errors including lack of adequate/reliable data and administrative and political infeasibility at both policy adoption and implementation stages. Grosh (1996: 146-147) has noted that often governments and policy-makers rarely do full fledged policy modelling such as cost effectiveness and cost benefit analysis, sometimes due to lack of data. But Grosh (1996 citing Gill et al. 1990:10, 24-28) observes also that requirements for good analysis to determine policy/programme outcomes can be formidable, and some intangibles such as work culture, stigma and power relations are hard to convert into monetary measures for analysis. So, governments make choices after exploring options for only a few weeks, using scanty data and rudimentary analysis. Grosh (1996) suggests five criteria for choosing among poverty programmes: administrative feasibility, political feasibility, collateral effects, targeting and tailoring the solution to the problem. When data are available, a full cost effectiveness simulation can be done to predict outcomes. In its absence, Grosh (1996: 181) suggests a clear pass/fail test on each of the five criteria to eliminate options that are unlikely to be effective. She stresses that though some programmes may be well designed with high expectations they should be eliminated if administratively and politically they are not feasible. Grosh suggests that a minimum level of administrative feasibilty is required and beyond it the way the programme is projected to the public, the relative power of beneficiaries, resources available to bolster administrative capacity, etc. affect programme outcomes. In this regard, the ability of the poor to avail themselves for exemption from the health user fee charges and the administrative feasibility of the health facilities to identify and grant exemptions are crucial, among other factors, to the achievement of the objectives of the policy. Policy Implementation Also relevant are the issues of the institutional capacity of the health workers to implement the policy as distinct from the policy itself. New approaches to understanding of policy implementation have received the attention of the discipline of development administration. More recent views such as Bjorkman’s (1995:374) emphasize that implementation cannot be guaranteed as a matter of course and “must therefore be taken into account when policy is formulated”. He suggests “multiple goals and small steps” rather than goals spanning over long periods that cannot be easily monitored. Corkery et al. (1995) advocate design of effective implementation strategies, while Grindle et al. (1991) suggest that governments must consider policies as long-term process that need assessment of different actors’ behaviour and allocation of resources to meet the challenges. The issues raised by Grosh have relevance for the implementation of user fees and the workability of the exemptions as examined in this paper. Attempts at tackling the adverse effects of the user fee policy on the poor by introducing exemptions for them can be examined within the context of administrative and political feasibilty as well as the culture and power relations of the poor and the health workers. Health Policy Reform and Implementation of the User Fee Policy Health Sector ReformsGhana’s health sector has had many reforms (Agyepong, 1999: 59-60). The most recent reform that has been in process since the early 1990s has been finally documented in what is popularly known as “Medium Term Health Strategy, 1996-2000”. It aims at improving access to health services, quality of care and efficiency, strengthening links with other sectors such as the Ministry of Agriculture and Education which also have health components in their activities or impact on the health of people (Ministry of Health, 1996). Its main achievement or focus has been the introduction of user fees (Nyonator and Kuntzin, 1999; Russell et al., 1999). The introduction of user fees in Ghana and other African states has also been a component of a range of strategies that are part of an international health reform agenda. They are linked to a broad set of public sector reform ideas and initiatives collectively known as the ‘new public management’ (NPM). The NPM in the health sector has other policies apart from the user fees - decentralization of the health sector with changes in organizational management and culture, and autonomous hospital boards and deregulation, enablement and regulation of the private sector. The main objectives of these policies are achievement of sustainable financing of health services, quality improvement, and equity with respect to access (Russell, 1996:767 and citing Mills, 1999 and Ferli et al., 1996). Institution of User Fees and Exemption of the PoorFees for health services in public facilities, first introduced in 1971, were very low and aimed at reducing unnecessary use of services rather than to generate revenue. The fees were raised slightly in July 1983 and increased substantially in July 1985 when a new hospital act was passed under the military regime of the Provisional National Defence Council (PNDC), aimed at recovering at least 15% of operational costs. Initially, the act allowed health centres and clinics to retain only 25% of the revenue from fees collected while hospitals were allowed to retain 50%. In 1990, this provision was amended and some public health institutions were selected for a pilot programme and allowed to keep all revenue generated from user fees. In 1992, the new fees were implemented nation-wide as government, influenced by multilateral donors (Russell et al., 1999), abandoned a phased implementation procedure started in 1990. Since then, a decentralized system of charging fees has been operating in the public health facilities and all revenue has been retained for operational or non-salary budget. Budget surpluses that are not invested in improving care quality are sent to the Ministry of Health (Agyepong, 1999: 60). A revolving fund for drugs known as “cash-and-carry” was initiated in 1992 by which all health institutions were to recover the full cost of drugs and keep this revenue to purchase drugs only. An overhead cost of 10-15% is added and the full cost is revised in line with inflation. The public health facilities also charge other fees for the following: Out Patient Department (OPD) cards and initial registration, consultation, admissions, gloves gauze, needles and syringes. Informal fees with various shades of legality and unauthorized fees are also collected from users (Agyepong 1999:60) The 1992 law, however, has a clause providing for exemption for the poor and treatment of emergencies whether patients are in a position to pay immediately or not. It does not indicate the criteria by which the poor can be identified though – whether income, geographical area, occupation, etc. Health workers are just instructed to use their discretion to grant exemption to anyone who says he/she cannot afford fees. They later apply for refund from government the exemptions that they grant. The implementation of the new user fee has been described by some as successful with respect to revenue generation despite some registered abuses. Revenue raising dominate other concerns and is at the expense of health care needs to the extent that the exemption clause has been either ignored or just labeled as difficult to implement, even in clear-cut cases where exemption could be granted. Evidence from the interviews conducted for this paper and secondary sources also show that the Ministry of Health has not been monitoring the fee collection system (Agyepong, 1999; Nyonator and Kuntzin, 1999: 329; Russell et al., 1999). Implementation of the User Fee and the Exemption Clause: Some OutcomesThe findings of three major studies covering the period 1989-1999 have been examined. Agyepong’s (1999) study examined patterns of utilization of health services in the Dangme West District of the Greater Accra Region. The findings showed that there was a fall in antenatal attendance, supervised delivery and outpatient attendance. The associated factors could be grouped into financial costs, problems of physical access and quality of services. Since physical access and quality of service have been long-term problems, financial costs emerged as a new component of the problems of health service utilization in the district. Regarding revenue generation, she reported that budget surpluses were recorded sometimes but were sent to the Ministry of Health instead of being utilized to improve quality of care or indication to grant more exemptions. Further investigations show that facility managers found the procedure for accounting for such expenditure cumbersome. Some functions were still highly centralized in the reforming health sector. The study also reported respondents’ suspicion about the lack of drugs in the health facilities while they were found in private pharmacies. They suspected alliance between the health workers and the pharmacies whereby the former promoted the business of the later by not having supplies and referring clients to the pharmacies to buy drugs at higher prices. Similar problems were observed in Zambia by Van der Geest et al. (2000:64) where unreliable drug supply persisted, making clients to consider fee payments which comprised a drug component unacceptable. The researchers suggested more humane charging practices whereby tangible products like drugs, rather than registration and consultation, can be exchanged for money. Waddington and Enyimayew (1989; 1990 cited by Agyepong, 1999:60; Nyonator, 1999 and Wa Mbugua, 1993:12) carried out two surveys, one in an administrative region (Volta Region) and the other in a district (Ashanti-Akim District). They indicate that following substantial increase in user fees in 1989, there was fall in utilization at both rural and urban clinics but larger falls in the former, despite their lower fees. They questioned the effectiveness of exemption or targeting of the poor under the user fee policy as level of attendance during pre-fee era was higher than after the fees were introduced. They noted that the trends in attendance suggest that people in rural areas who are mostly the poor are more vulnerable to the negative impact of user fees than the urban dwellers and large differences in physical access to modern health facilities among rural communities. Nyonator and Kuntzin’s (1999) work was based on a 1996 study on user fees in the Volta Region which used a variety of data collection methods including interviews with patients and facility managers, community-based focus group discussions, analysis of facility records and previous household survey data. The study found that official exemptions were largely non-functional and benefited health workers mainly. Their examination of facility records showed that less than one in 1,000 patient contacts were granted exemptions in 1995, and some were health workers themselves. Meanwhile, the level of revenue from user fees accounted for between two-thirds and four-fifths of the non-salary-operating budget of the government health institutions and virtually all of the resources for non-salary operating expenses in mission hospitals. Furthermore, though management skills for effective use of revenue has improved in the public facilities, the managers were having difficulty in using it to improve quality of care because they found the mechanism involved to be complex. When interviewed, facility managers complained that, administratively, it is not feasible to identify the poor or verify claims and that no clear criteria are provided them to identify and grant exemption. They use their discretion to grant exemptions and have been denying even genuinely poor clients. The researchers, however, observed that declining government budget allocations and supplies might have made it imperative for the facility managers to be more concerned about collecting revenue than attending to financial access of the poor. Similar problems have been reported in Zimbabwe where patients have to prove that their monthly income is less than Z$400 which must be verified by presentation of pay slips or an exemption card from social workers (Dlodlo, 1995:9). Commenting on the inappropriateness of this system, Dlodlo deplores the ignorance of the policy about the situation of some women who do not live with their husbands, have no idea about how much they earn and find it too much to ask them for their pay slip. Interviews with patients reported uncertainty about the cost of a visit among the poor and prevented some from going for treatment. The findings indicate that the poor were resentful about the user fee policy and complained that it has not resulted in improvement in care quality, not even a change in attitude of health workers while the non-poor were reaping the benefit of increased drug availability. Nyonator and Kuntzin (1999: 337) wondered how far down the income scale the benefits have reached and concluded that “health facilities in the Volta Region have achieved a kind of ‘sustainable inequality’, with fees enabling service provision to continue, while concurrently preventing part of the population from using these services”. All the three studies reveal that problems arising from implementing the user fee policy and exemption clause are major obstacles to the financial access of the poor to health services. The problems of undercoverage and leakage render the exemption clause ineffective in meeting the financial access needs of the poor. The main reasons are not only lack of specification of criteria for identification of the poor and for granting exemptions but also the following: · attitude of the facility managers to the needs of the poor, · the large number of potential beneficiaries (the absolute poor, health workers themselves and the non-poor who have been made worse off by worsening economic conditions), · the benefits of charging fees to meet operational budget needs as government allocations decline, and · lack of monitoring of the policy by government. Despite other achievements of the user policy, the fall in facility utilization due mainly to the implementation problems of the exemption clause shows that more effective and equitable health policies must be adopted for the health sector. Adopting More Effective and Equitable Health Policy Targeting: Short-term StrategyAn obvious policy response to these findings should be outright elimination of targeting in Ghana’s health delivery system. However, this paper recommends strengthening of targeting as a short-term strategy for effective and equitable health delivery in Ghana. A 1996 evaluation report on Tanzania’s experience of user fee policy has also indicated that both providers and users asked for “strengthening of exemptions and waivers”, among other strategies to improve health delivery in that country (Mmbuji 1996 et al. 1996). Ghana’s health delivery system may also become more equitable by adopting such an approach. Vast regional disparities in socioeconomic development and marked differences in the socioeconomic distribution of the burden of disease give support to such an approach towards effective and equitable health delivery. Inequitable socioeconomic development policies explain rural-urban differences in human development and levels of burden of disease. Generally, the southern regions (Western, Central, Greater Accra, Eastern, Volta, Ashanti and Brong Ahafo) have been favoured more by government urban-biased socioeconomic development policies that have been implemented over the years than the northern regions (Northern, Upper East and Upper West). The Central and Western regions in the south show some degree of departure with respect to some indicators though. The regional disparities with respect to incidence of poverty in the population can be observed in Figures 1. Incidence of poverty ranges from 5% in the Greater Accra Region to 88% in the Upper East and Upper West Regions in 1998/99. The southern regions generally have lower and declining poverty rates from 1991/92 to 1998/99 while the rates in the northern regions are higher and even increasing in two of the regions in this part of the country. Further details of the results of the survey from which the data come from show regional differences are higher than the rural-urban disparities. Differences in the levels of under-five mortality reflect the same pattern as observed for incidence of poverty (Figure 2). This suggests an association of poverty with disease and mortality rate. Indeed major causes of death in Ghana are malaria and communicable diseases caused by poor environmental sanitation. The poor are, therefore, more prone to illness and carry greater burden of disease in the country. Figure 3 also shows the variations in malnutrition among women and children by region and residential background. Though there is considerable chronic malnutrition among all categories the pattern here follows the previous ones. The percentage of who are stunted ranges from 11% in the Greater Accra Region the south to 40% in the Northern Region. The rates for the urban and rural areas are 14% and 30% respectively. The analyses of these health and anthropometric data suggest an association of poverty with mortality rate and health status. The poor, by their living conditions, are more prone to the diseases and therefore carry greater burden of disease in the country. A major implication of user fees for the poor is lack of access to health services and consequent higher mortality rate. The higher rates of morbidity and mortality already existing among the poor suggest that a health policy that denies them access to health services will worsen their health status. It is because of such disparities that Ghana’s poverty reduction programme, 2000-2004 has laid emphasis on equity of health outcomes with special focus on reducing geographical disparities and addressing diseases (such as malaria and guinea worm) and health conditions (particularly malnutrition) which affect the poor most (Republic of Ghana 2002:97). Statistics on ten-leading diseases reported at outpatient department shows that health delivery needs to focus on the poor who have the greatest burden of such diseases (Table 1). The four poorest administrative regions (out of ten) with the poorest health conditions have therefore been selected to receive special attention – Northern, Upper East, Upper West and Central regions. This paper recommends such an approach because it devotes more resources to high risk categories of health. The paper also recommends a combination of a range of reduced and graded fees and waivers for all mothers and under-fives and the aged (75+years) among the various regions based on the levels of poverty and burden of disease. This shall serve three purposes. This will avoid reduced access of mothers and children to services so that the prioritization of maternal and child health in health policy in Ghana (and as recommended by WHO and UNICEF) may not be compromised by user fee policy. Secondly, the new criteria are more administratively feasible for the health institutions because identification of the beneficiaries of this safety net provision may be easier. Thirdly, it can guarantee political consensus for the user fee as all regions and social categories have mothers, children and the aged who can benefit from such a concession. Moreover, government has been following the Dakar Consensus by laying emphasis on maternal and child health in health delivery at all levels. Ensuring the access of mothers and children to health services is just another appropriate step toward the realization of the goal to provide primary health care for all. The paper also recommends that government allocates exemption funds to facilities under annual budgetary allocations instead of maintaining the practice whereby health facilities apply for exemptions/waivers refund after granting them. This will motivate facility managers to attend to cases seeking exemption and make them not to see the granting of exemptions as loss of revenue. But government must effectively monitor this and the whole user fee policy to prevent the misallocation of the funds allocated for the purpose. It may, however, be difficult for government to cater for all categories of persons who may be considered for exemption – children, women and the aged. Some of these people may even be able to afford payment for health services. In this regard, government can adopt a policy that encourages those who can afford payment for services to refrain from requesting for exemption. Indeed, the patronizing of private health services that have been offered for fees over the years is an indication that health user fees can be afforded by some. What is needed is a policy that enhances the confidence of the genuinely poor members of the population to avail themselves for exemption while discouraging those who seek to abuse the provision from doing so. A good policy can reduce the error of inclusion (including those not intended to benefit from exemption) and error of exclusion (excluding those intended to benefit from exemption). The success of such approaches will depend on the attitude of health facility managers and health workers. Based on available information on poverty and health indicators, certain geographical areas may also be granted certain concessions such receiving free treatment for some identified diseases or health conditions. The Central and northern regions, for example, may be considered for some packages for maternal and child health services because of their extremely higher infant and child and maternal mortality rates. Treatment of water-borne and water related diseases in communities where such diseases are endemic and safe drinking water is unavailable. All these initiatives demand the development of a reliable health data base and other socioeconomic information that are required for planning and budgeting for an efficient health delivery system. The policies recommended above are affordable and feasible for government and providers. They are also more beneficial for users and will make health services more available for all. But long-term sustainable and more comprehensive policies are also needed to deliver health services more effectively. More Comprehensive Long-term Health PolicyGhana’s health delivery can become more effective and equitable in the long-term when distortions in the delivery system (such as allocating a disproportionate share of the health budget to curative services that serve high income groups) are removed and more equitable socioeconomic policies are adopted and implemented. In this regard, the ongoing discussion and trial of a health insurance policy can be introduced gradually for the non-poor who can afford it so that their contribution can become a source of subsidy for the poor. Ghana adopted the status of Highly Indebted Poor Country (HIPC), a World Bank classification of countries with an associated macroeconomic framework, in the year 2001 after almost two decades of Structural Adjustment. The main policy document on the HIPC initiative recognizes that “ill health is both a consequence and cause of poverty – through lack of funds and knowledge to prevent illness” (Republic of Ghana 2002: 96). In this regard, provision of basic social services and basic education for the poor and more emphasis on preventive health care must be at the centre of socioeconomic policy. These are major factors that made success stories such as Sri Lanka’s transformed health delivery system (Bjorkman 1994). Health policy in Ghana is comprehensive on paper. Its implementation also needs to become so. Government and health practitioners must also consider more seriously the negative socio-cultural factors that have determined the health behaviour of a large proportion of the population. There is a need to tackle this in health educational programmes that aim at encouraging best health behaviour practices among all age groups, and mothers in particular. The National Health Insurance Policy and the PoorSince it came into power in January 2003, the present government of the National Patriotic Party (NPP) has made efforts to introduce a new health policy in the country that can make health services more available to all citizens. In 2002, the Minister of Finance mentioned the intention of the government to introduce a national health insurance policy in the 2002 budget. After much debate on the bill introducing the policy and amendments thereof, parliament passed the National Health Insurance Bill on August 26, 2006 (Unik FM 6pm News August 27, 2003). The National Health Insurance Scheme which was launched on March 18, 2004 (Unik FM Radio Station, 6pm News, March 18, 2004, 7.30am). The National Health Insurance Scheme requires all persons aged 18 years and over to contribute C6,000.00 per month when enrolled under the scheme. Children aged 0 –17years will be covered if their parents are registered under the scheme. The scheme will also provide exemption for the poor and some other categories. Furthermore, there will be pre-determination of the poor at the District Level under this new policy. District Health Committees will determine their poor persons and have their names sent to the national level for funds to be sent to them so that they can cover these poor in their districts. The poor will then be provided insurance cards which they will use to access health services. It has been thought that identification of the poor at the district level will be easier since the district health committees are more likely to identify their poor more easily than health facility workers and managers. Thus the new procedure may eliminate the problem of identification of the poor. Since personnel at the district level are expected to be familiar with their subjects, their ability to identify the poor may be greater than health providers at any level under the cash-and-carry system. The consideration of exemption of the poor under the new health policy is a demonstration of the recognized need to have the poor granted a guaranteed access to health services. If problems of under-coverage and leakage can be minimized, this new strategy may prove to be a solution to the problem of identification of the poor and their inability to enjoy the benefit of exemption from fee payment. On the other hand, monitoring of the programme by the health authourities at the national level to ensure that it is successful will be necessary. Moreover, the district health committees should be prepared to face the challenge of developing a number of procedures to eliminate those members of their districts who are not poor but may just want to enjoy the provision. In this regard, they may have to consider using criteria other than income levels to eliminate such categories, for example, possession of assets. The task will also require the developing of statistics or database at all levels (district, regional and national) that can enable health financing and delivery to be performed more easily than it is being done presently. Conclusion The general objective of this paper was to examine the problems associated with the exemption of the poor under the implementation of the user fee in Ghana and make policy recommendations based on the findings of the study. Its specific objectives were to find out how the clause on exemption has been implemented alongside the charging of user fees and to examine the associated problems and outcomes. It also sought to establish whether Ghana needs targeting as a component of health policy, at least in the short term and to recommend alternative more effective policies for the country’s health delivery system. The findings of the study reveal that problems arising from implementing the user fee policy and exemption clause are major obstacles to the financial access of the poor. Both under-coverage and leakage render the exemption clause ineffective. In one of the studies, as low as one in every 1,000 patient contacts had exemption granted. The absence of criteria for identifying the poor is not the only problem making the provision unavailable to them. Other factors include attitude of the facility managers and their fear of the potential large number of beneficiaries that can lead to loss of revenue while government allocations have been declining and lack of monitoring of the policy by government. Despite other achievements of the user policy such as more availability of drugs, the fall in facility utilization due mainly to the implementation problems of the exemption clause shows that more effective and equitable health policies must be adopted for the health sector. The paper, examining the socioeconomic context of health delivery in the country, recommends strengthening of targeting as a short-term health policy while long-term policies consider satisfaction of basic needs and preventive care as well as adoption of human development approaches and more equitable socioeconomic development policy. The granting of exemption to the poor under the National Health Insurance Scheme that has just been introduced, is a step in the right direction. Governments in Africa, such as Ghana, also need to begin to consider seriously those social and cultural factors that are determinants of health among their citizens. References
[1] The author is indebted to Prof. J.W. Bjökman of the Institute of Social Studies, The Hague for supervising the project work from which this paper has been derived. Copyright 2004 - Union for African Population Studies |

{kind=link}
{kind=link}
{kind=link}