 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 19, No. 2, Sup. B, 2004, pp. 31-59 The Social and Economic Implications of HIV/AIDS[1] Victor Gaigbe-Togbe and Mary Beth Weinberger[2] Population Division, Department of Economic and Social Affairs, United Nations - New York, USA Code Number: ep04034 ABSTRACT The paper reviews the state of knowledge on the
demographic and socio-economic impacts of AIDS. It shows that HIV/AIDS has
been taking a devastating toll on human lives. Life expectancy has already
fallen by more than 10 years in the most affected countries. Households are
feeling the impact of AIDS in terms of loss of earnings and increased
expenditure for medical care. As a result of HIV/AIDS, food consumption is
decreasing in many AIDS-affected households, leading to malnutrition,
especially among young children. The HIV/AIDS epidemic is also imposing serious
costs on the private sector in the most affected countries. AIDS deaths reduce
the number of available workers, since the deaths occur predominantly among
workers in their most productive years. The available evidence points to an
impact of the epidemic on the labour costs and productivity of most firms
depending on the skills of those who are affected and whether they are
replaceable or not. HIV/AIDS is also having a dramatic impact on the
agricultural sector, partly because the great majority of the infected
population in the most affected countries lives in rural areas. The health and
education sectors are also feeling the impact of HIV/AIDS. Children in
AIDS-affected households are often taken out of school. Deaths and illnesses
have also affected education-sector administrators and teachers resulting in a
reduction in the supply of educational services and an increase of educational
system costs. The health sector in the most affected countries is also
witnessing a shortage of health professionals and an increase in the demand for
health care. Finally, while there seems to be less agreement among economists
about the impact of HIV/AIDS on the growth of GDP per capita at the present
time, the impact of HIV/AIDS on the economy and development is likely to
intensify in the near future. The longer-term economic effects resulting from
lower investment in human capital – especially the education, health and
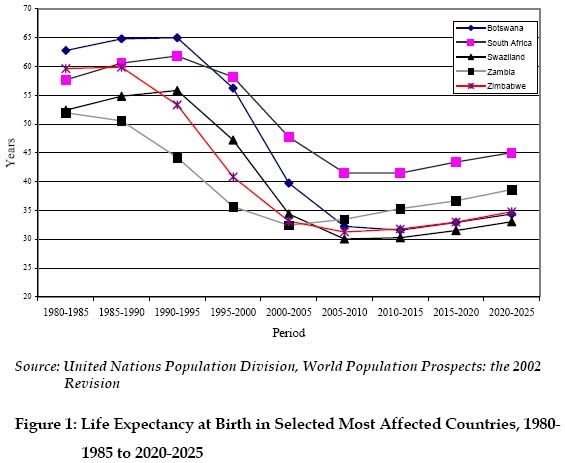
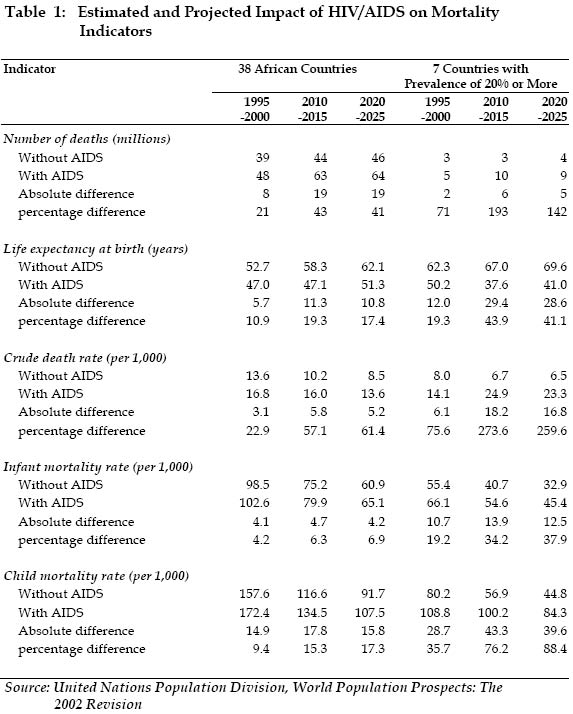
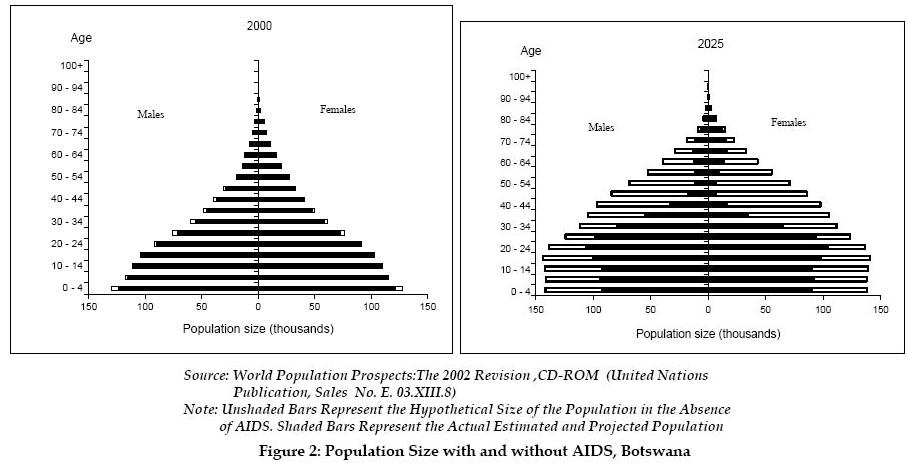
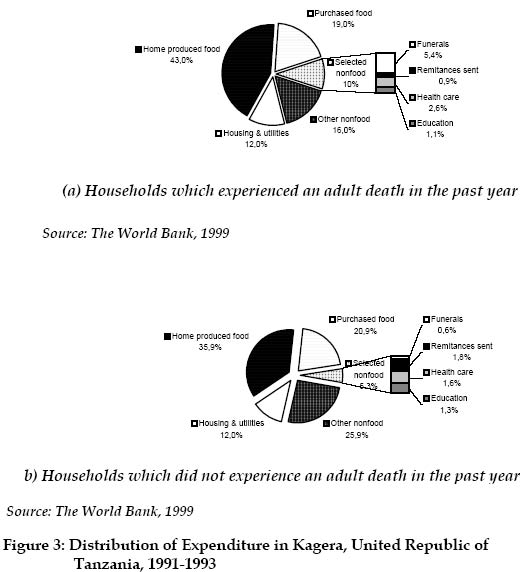
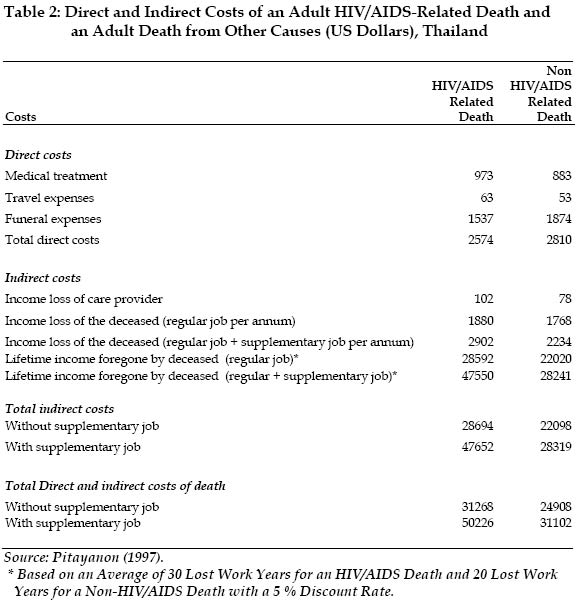
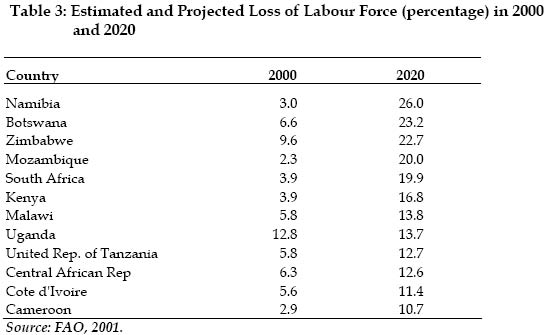
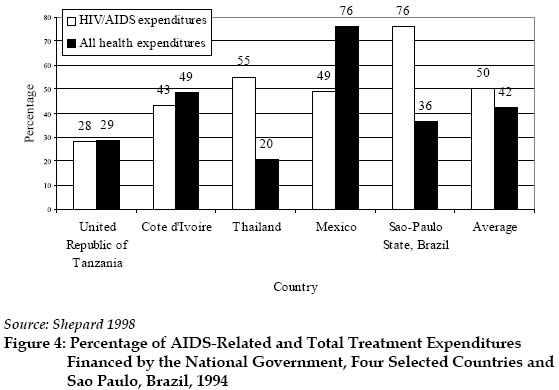
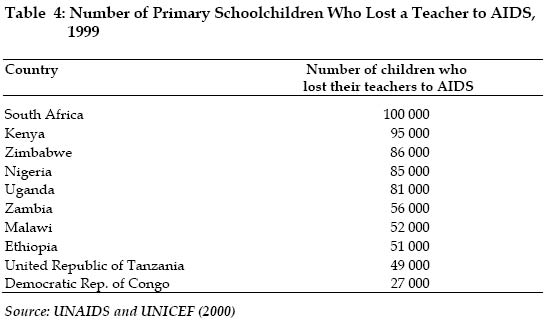
nutrition of future workers – may be severe. Since its onset in 1981, when the first AIDS cases were reported, the human immunodeficiency virus (HIV) epidemic has become not only the deadliest epidemic in contemporary history but also a major demographic, humanitarian and development crisis. As of end-2002, 42 million people were infected with the HIV and 25 million had already lost their lives to the disease. More than 13 million AIDS orphans are currently living in sub-Saharan Africa. The HIV/AIDS epidemic is leading to a reversal of hard-won gains in life expectancy of the previous decades. Moreover, the HIV/AIDS epidemic has been threatening the social fabric of societies in the most affected countries and eroding the social and economic safety net. This paper reviews the state of knowledge on the social and economic impact of AIDS. The first section discusses the demographic impact of the epidemic. Life expectancy at birth is estimated to have dropped by more than 20 years for some countries, while a few are expected to experience a decline in their population in the near future. The second section examines the impact of AIDS on households, the first units affected by the epidemic. The third section presents the impact of AIDS on the private sector (firms and companies). The fourth section investigates the impact on the agricultural sector. The fifth and sixth sections give an assessment of the impact of the AIDS epidemic on health and education elements of human capital. Lastly, the impact on macro-economy is examined, followed by a summary of the lessons learned and the proposition of new avenues of research to further investigate the impact of the HIV/AIDS epidemic. The Demographic Impact of AIDS The AIDS epidemic is taking and will continue to take a devastating toll on human lives. According to the 2002 Revision of the United Nations World Population Prospects (United Nations, 2003), life expectancy at birth has already fallen by more than 10 years in the most affected countries, those with an adult HIV prevalence of 20 % or more. In most of the countries that are severely affected by the epidemic, HIV/AIDS is responsible for stopping or even reversing the long-term decline in mortality that had been registered until recently. The impact on population size is most marked in Africa. In 38 African countries[3] for which the United Nations Population Division explicitlyincorporates the impact of AIDS into its 2002 Revision of estimates and projections, the population is estimated at 603 million in 1995, 16 million fewer than it would have been in the absence of AIDS. By 2025, the population of these 38 African countries will reach 983 million, 14 % fewer than in the absence of AIDS. In the 7 countries with an adult prevalence of 20 % or more, all in Africa, the impact is more striking. By 2025, the population of these countries is projected to be 35 % lower than it would have been in the absence of AIDS. Life expectancy at birth, a measure indicating the average number of years that a newborn child would live if mortality remained constant throughout his lifetime, is estimated at 47 years in 1995-2000, 6 years lower than it would have been in the absence of AIDS in the 38 African countries. It is projected to reach only 52 years by 2020-2025, 10 years lower than it would have been in the absence of AIDS. In the seven countries with an adult HIV prevalence of 20 percent or more, life expectancy at birth is estimated at 49 years in 1995-2000, 13 years lower than in the absence of AIDS. By 2020-2025, the difference between the life expectancy with AIDS and the life expectancy without AIDS will reach 29 years, a 41 % difference. Figure 1 shows the estimated and projected life expectancy at birth for specific countries of this group. Table 1 presents the estimated and projected impact of HIV/AIDS on mortality indicators for the 38 African countries with moderate to high adult HIV prevalence for which the demographic impact of AIDS has been incorporated into the estimates and projections. The same table presents also these indicators for the seven countries with prevalence over 20 %, namely: Botswana, Lesotho, Namibia, South Africa, Swaziland, Zambia and Zimbabwe. The additional number of deaths due to AIDS in the 38 African countries is estimated at 8 million in 1995-2000. By 2020-2015, it is projected to reach 19 million. In the seven most affected countries, HIV/AIDS will cause an additional 6 million deaths in 2010-2015. In the 38 African countries, life expectancy at birth is estimated at 47 years in 1995-2000, 5.7 years lower than it would have been in the absence of AIDS. Life expectancy is expected to decline in 2000-2005 before resuming an upward trend, but reaching only 51.3 years by 2020-2025. In the absence of AIDS, life expectancy at birth would have reached 62.1 years in 2020-2025, that is, 10.8 years higher without AIDS (table I). The effect of AIDS is more marked in the seven countries with adult HIV prevalence above 20 %. Life expectancy in those countries is estimated at 50.2 years in 1995-2000, about 12 years lower than it would have been in the absence of AIDS. By 2020-2025, the difference in life expectancy with and without AIDS is projected to reach 28.6 years. HIV/AIDS is having effects on the crude death rate (the annual number of deaths per thousand populations) similar to those on the life expectancy at birth (table 1). In some cases, death rates that were projected to decline in the absence of HIV/AIDS will instead rise. For instance, in the absence of AIDS, the crude death rate for the 38 African countries considered was expected to decline from 13.6 deaths per 1,000 persons in 1995-2000 to 8.5 deaths per 1,000 in 2020-2025. AIDS will cause the crude death rate to increase from 16.8 deaths per 1,000 in 1995-2000 to 17.5 deaths per 1,000 in 2000-2005 before declining to 13.6 deaths per 1,000 in 2020-2025. Infant mortality in the 38 African countries considered is estimated to decline from 103 deaths per 1,000 live births in 1995-2000 to 65 deaths per 1,000 live births in 2020-2025, whereas under-five mortality is estimated to decline from 172 deaths per 1,000 live births to 108 deaths per 1,000 live births during the same period. In the absence of AIDS, the decline in both infant and under-five mortality rates would have been much steeper, from 99 deaths to 61 deaths per 1,000 live births and from 158 deaths to 92 deaths per 1,000 live births, respectively. In the seven African countries with the highest adult HIV prevalence, infant and under five-mortality are estimated at 66 deaths and 109 deaths, respectively, in the presence of AIDS in 1995-2000, but only 55 and 80 deaths per 1,000 in the absence of AIDS. The age-differentiating characteristic of the AIDS epidemic makes its impact especially devastating for the affected populations. Figure 2 above presents the age pyramid of Botswana in 2000 and 2025 with AIDS and in the absence of AIDS. Whereas the impact of AIDS is not apparent on the age structure in 2000, by 2025, a serious deficit is projected in the population of working age, especially those aged 30 to 50 years. As AIDS kills predominantly the younger adults, Botswana and the other worst-affected countries will witness in the future a hollowing out of an entire generation. The Impact of HIV/AIDS on Households The impact on households and families begins as soon as a member of a household starts suffering from HIV-related diseases. In this regard, three kinds of impacts can be distinguished. The first one is the loss of the income and household production of the family member, in particular if he/she is the breadwinner. The second impact is the increase in household expenditures to cover the medical costs. The third impact is the indirect cost resulting from the absenteeism of the members of the family from school or work to take care of the patient. When the person dies, the temporary loss of income becomes a permanent loss; funeral and mourning costs are incurred; and the family may compensate by reducing investments in productive activities (e.g., removing children from school to save on expenses and increase household labour). Households may lose most of their savings in order to pay for the high costs of HIV/AIDS-related health care and funeral expenses. Furthermore, community attitudes towards helping needy households may contribute to the impact of the disease. For example, households in the more urbanized areas may suffer the worst impact because of the lack of community support. In societies where stigmatization of the HIV-affected individuals and households is common, the impact of the HIV/AIDS epidemic may be even more severe. The change in the composition and structure of households caused by the HIV/AIDS epidemic may be not only quantitative but also qualitative. Thus, the number of impoverished female-headed households will increase when the male breadwinner of the household dies of AIDS. Where the AIDS patient in the household is female, the impact of the HIV/AIDS epidemic on the household can take a form that is different and of even greater magnitude. Indeed, the (often culturally determined) position of women can affect the household impact of an illness such as AIDS in males. One of the striking features of the economic impact of AIDS on affected households and families in Zambia, for example, is the rapid transition from relative wealth to relative poverty. Haworth’s (1991) survey of AIDS-affected families found that the shift into poverty was most visible in families in which the deceased father was both the breadwinner and tenant of a house provided through his job. Many such families were forced to move after the death of the father, with a majority of those families reporting economic difficulties. In the early 1990s, the International Children’s Centre in Paris launched a multi-country field study of the socio-economic evolution of children and families affected by HIV/AIDS in three countries: Burundi, Côte d’Ivoire and Haiti. In each of these countries, about 100 households affected by HIV/AIDS were followed longitudinally for a year. In Côte d’Ivoire, the study showed that marked differences occurred in the economic activities of households, with a steady decline in the number of economically active household members throughout the course of the study (Béchu, 1997). In this study that tracked 107 households with at least one adult AIDS patient, it was found that per capita consumption dropped in households where the AIDS patient either died or moved away. In households in which the AIDS patient remained relatively free of symptoms, per capita consumption remained stable over time. In a longitudinal study carried out in Kagera, United Republic of Tanzania in 1991-1993, households that experienced an AIDS adult death in the year prior to the first wave of the survey spent, in relative terms, more on funerals and health expenditures than did households which did not experience an adult death (figure 3), although households without an adult death had higher total expenditure on all goods and services than those with an AIDS adult death. A more recent study in Zimbabwe showed that heavy expenditures, substantial loss of income and erosion of capital assets associated with terminal illnesses are seriously undermining the economic viability of households (Mushati et al., 2003). In another longitudinal study conducted in the Free State of South Africa, it was found that affected households allocated more of their resources to food, health and rent and less to education and clothing than non-affected households (Booysen, 2003). Outside of sub-Saharan Africa, the AIDS epidemic is also having its toll on affected households. In a study carried out in Thailand, Pitayanon et al. (1997) compared the direct and indirect costs of an adult HIV-related death with those of an adult death from other causes. The impact of an AIDS-related death on the household was substantial and much greater than the impact of a death from other causes (table 2). While the direct costs of an adult non AIDS-related death are slightly higher than those of an AIDS-related adult death, the indirect costs associated with an AIDS-related adult death are on average 30 % higher than those of a non-AIDS adult death. This is because AIDS deaths occur mainly at the prime working-age years, resulting in a higher number of years lost than deaths due to other causes. Other socio-economic impacts of a HIV/AIDS-related death included the loss of the family labour production. The production loss in the households was almost 50 % leading to about a 47 per loss in the household income. The loss of a breadwinner tends to reduce the economic viability of the household that remains, and some households faced with this situation may disband, with the members dispersed to the homes of relatives. However, little is known about how frequently this occurs, since most studies are not designed to follow up households or household members who move out of the study area. In one study of rural South Africa, Hosegood and others (2003) found that households experiencing at least one AIDS death during a one-year period were nearly three times as likely to dissolve as other households. A study in Uganda (Ntozi, 1997) inquired retrospectively about migration of the spouses of former household members who had died. In total, 37 % of widows and 17 % of widowers had migrated from their original homes. For both sexes, migration was more common for younger spouses, and results suggested that those who were in worse health (possibly because of AIDS) were more likely to leave. Remarriage is potentially another way of coping with the economic as well as the emotional and social losses resulting from the death of a spouse. In some societies there are strong traditional expectations that widows will remarry, and widows’ and children’s access to property and other resources may depend on remarriage. If the death was due to AIDS, however, the surviving spouse may be infected, and remarriage poses a grave risk of spreading the disease. Little is known, however, about how marriage practices are actually changing in the face of this risk. In Malawi, divorced or widowed women were less likely to remarry if their husband had been HIV-positive, but the partner’s HIV status did not affect the likelihood that men would remarry (Floyd and others, 2003). Studies from Uganda in the early 1990s indicated that the practice of widow inheritance was in decline. But results also suggested that many people were basing their decisions about risks of remarriage on the appearance of health, and many of those who appeared healthy are likely in fact to have been infected by HIV (Ntozi, 1997; Muzika-Gapere and Ntozi, 1995). Households may also try to adjust to the loss of an adult by sending some members, particularly children, to live with other relatives, or by taking in working-age relatives. The feasibility of doing this probably varies greatly between societies, depending on long-standing social customs, and, for individual households, depending on the availability of suitable kin. A review of changes in household structure in three areas heavily affected by HIV/AIDS found that, in the cases of Tanzania and Uganda, many households added a member after a death occurred, with the result that the average household size following an adult death declined by less than one member, and the dependency ratio in affected households rose by only a modest amount. By contrast, in Thailand, where households were smaller to begin with than in the African cases, the households where an adult died remained one person smaller even two years after the death, and their dependency ratio nearly doubled (World Bank, 1999). The HIV/AIDS pandemic has led to increased attention to the fate of the growing number of orphans. At the end of 2001, an estimated 14 million children aged under 15 years had lost one or both parents to HIV/AIDS, 11 million of whom lived in sub-Saharan Africa (UNAIDS, 2002a); the number is forecast to nearly double by 2010. Several recent studies have examined the relative welfare of orphans by comparing them to non-orphans in the same society with respect to levels of school enrolment, household economic status and, less frequently, nutritional and health status. The studies have shown that orphans are at a substantial disadvantage. The amount of educational disadvantage is greatest for orphans who have lost both parents. In recent surveys of sub-Saharan countries, only 60 % of children aged 10-14 who lost both parents attended school on average, compared to 71 % of those with both parents still alive and living with at least one biological parent (UNICEF, 2003). Although many orphans live in households that are relatively well-off economically, in many countries orphans are disproportionately found in poor households. Orphans' lower school enrolment is not entirely explained by the greater poverty of households where orphans live, although poverty itself confers a large disadvantage on orphans and non-orphans alike (Ainsworth and Filmer, 2002; Case, Paxson and Ableidinger, 2003). Even though grandparent-headed households tend to be female-headed and poor, living with a grandparent is, on average, associated with higher educational enrolment for orphans than is living with other relatives, particularly more distant relatives. Orphans who live with a non-relative, though they are a small minority, are at an enormous educational disadvantage (Case, Paxson and Ableidinger, 2003). Girl children have much lower enrolment ratios than boys in many of the countries impacted by HIV/AIDS; however, orphanhood by itself generally disadvantages boys and girls equally with respect to schooling. Available evidence also points to nutritional disadvantage for orphans (Ainsworth and Semali, 2000; Subbarao, Angel and Plangemann, 2001). Taking in orphans represents a substantial economic burden for many of the receiving households, as well (Deininger, Garcia and Subbarao, 2001). Studies conducted in Zimbabwe (WHO, 2002) and Thailand (Knodel and Im-em, 2002) showed that older caregivers in particular are under serious financial, physical and emotional stress due to their care-giving responsibilities. The AIDS epidemic not only puts more stress on older persons, but it also impoverishes them at the very time they themselves may need support. The empirical evidence, although sketchy, points to a tremendous impact of AIDS on households. Indeed, households and families bear most of the burden since they are the primary units in which individuals cope with the disease. Few studies have documented how the impact varies according to the characteristics of the household. Moreover, the impact on orphans has only started receiving attention. Similarly, the effects of the AIDS deaths of children have only begun to be studied. The Impact of HIV/AIDS on Firms and the Private Sector The HIV/AIDS epidemic is imposing serious costs on the private sector in the most affected countries. AIDS deaths may lead directly to a reduction in the number of available workers, since the deaths occur predominantly among workers in their most productive years. As younger, less experienced workers replace experienced workers, worker productivity may be reduced. The impact of AIDS will also depend on the skills of affected workers. If skilled workers who occupy important positions in the firm become sick or die from AIDS, the company may lose its institutional memory—that is, the “know-how” accumulated through many years of experience. The absence of workers in the company may also have an impact on the morale of the remaining workers, which could lead to declining productivity. HIV-infected workers also are likely to become less productive as infection progresses to AIDS. In Namibia, NamWater, the largest water purification company, announced in 2000 that HIV/AIDS was “crippling” its operations (Angula, 2000). They reported a high staff turnover due to HIV-related deaths, increasing absenteeism and a general loss of productive hours. A recent study in Kenya (Fox et al., 2003) showed that tea pluckers who died of AIDS-related causes produced a quantity of tea roughly one-third less in their last two years of life than other healthy workers. The AIDS patients who died had also suffered an earning loss of 18 % in the year before their death. Firms that have a health programme to help workers who become sick may find themselves responsible for substantial medical costs. The insurance scheme of the firm may become more expensive as insurance companies increase the costs of coverage as a response to high HIV prevalence rates in firms. This could impede any saving for investment by the firms. A study on Lonrho companies in Malawi found that deaths-in-service benefits increased by more than 100 % between 1991 and 1996 (Ntirunda and Zinda, 1998). The study also found that AIDS-related costs were 1.1 % of the total costs and 3.4 % of gross profits of these companies in 1992. Another study of five firms in Botswana found that the impact of HIV/AIDS depended on the type of business, the skill level of employees, the type of benefits provided, and the amount of savings (Stover and Bollinger, 1999). Many businesses will also suffer a shrinking market for their goods when HIV/AIDS epidemic in the community leads to the impoverishment of households which can no longer afford to purchase goods. Businesses that produce “luxury goods” are more likely to experience a decline in the demand of these goods. A South Africa furniture manufacturer (JD Group) projected an 18 % reduction in its customer base as a result of HIV/AIDS (Whiteside, 1996). The impact of HIV/AIDS on firms depends partly on the age structure of the workers in the firm. For example, a study conducted in Zambia in Barclays Bank showed that mortality peaked in the 30-39-year age group. The death rate rose from 0.4 % to 2.2 % between 1987 and 1991,and the bank paid more than ZK 10 million (US$ 58,140) in the form of ex-gratia payments to the families of employees who died from HIV/AIDS (Smith and Whiteside, 1995). The study also showed that medical expenses and training costs were on the increase whereas man-hours were reduced. Not only does the absence of infected workers contribute to revenue losses at the firm level, but absence of healthy workers taking care of infected family members or attending funerals of co-workers can also be detrimental for companies. It has been estimated that extension workers in north central Namibia spent at least 10 % of their time attending funerals (Engh and others, 2000). In summary, the few available studies of the impact of HIV/AIDS on firms point to an impact of the epidemic on the labour force, costs and productivity of most firms depending on the skills of those who are affected and whether they are replaceable or not. The evidence available also points to a greater impact of the HIV/AIDS epidemic on small firms, those with less than 10 employees. The loss of a few employees in key positions in these firms can lead to their disappearance. Although more studies have been conducted recently, the results of many such studies are still not in the public domain. Their publication would aid in assessing the economic impacts of the epidemic, and in devising sound public policies in response. The Impact of HIV/AIDS on Agriculture HIV/AIDS is also having a dramatic impact on the agricultural sector, partly because the great majority of the infected population in the most affected countries lives in rural areas. In many African countries, farming and other rural occupations provide a livelihood for more than 70 % of the population. A number of studies have been conducted to assess the impact of HIV/AIDS on agriculture. Most of these studies were conducted under the auspices of FAO. Indeed, of the AIDS impact studies conducted so far, the majority have dealt with the rural world. A study conducted in Burkina Faso in 1997 found that the HIV/AIDS epidemic had led to shifting work patterns and an overall reduction in food production. Revenues from agricultural production had decreased by 25 to 50 % in HIV/AIDS-affected households (FAO, 1997). A study among agricultural workers in the United Republic of Tanzania showed that a woman whose husband was sick was likely to spend 45 % less time working than if the husband were healthy. In Kagera, a survey showed that, on average, adults in households that experienced a death spent five hours less in farming during the previous week than those without a death (Mutungadura, 2000). In Kenya, a study found that the commercial agricultural sector is facing a severe social and economic crisis due to the impact of HIV/AIDS (Rugalema, 1999). The loss of skilled and experienced labour to the epidemic is a serious concern. But it is difficult to quantify the impact of the epidemic in terms of increasing costs. The impact of HIV/AIDS on agriculture may also depend on the level of prevalence in the country or area. For example, production loss in AIDS-affected households was reflected in a survey conducted in Zimbabwe, a country with an adult HIV prevalence of more than 25 %. According to this survey, conducted in 1997 by the Zimbabwe Farmers’ Union, agricultural output in communal areas declined by nearly 50 % among households affected by AIDS (Kwaramba, 1997). Maize production by smallholder farmers and commercial farms declined by 61 % because of illness and deaths from AIDS. These production losses could result from a number of factors including shifting production patterns. But according to the same author, so far Zimbabwe data do not indicate a dramatic switch from cash to subsistence crops. The impact of AIDS is expected to increase in the future. FAO has estimated that in the 27 most affected countries in Africa, 7 million agricultural workers have died from AIDS between 1985 and 2000 and that 16 million more deaths are likely to occur in the next two decades. In the ten most affected African countries, labour force decreases ranging from 11 to 26 % are anticipated (table 3). In summary, the studies available show that HIV/AIDS is having a detrimental impact on the agricultural sector. Since, in many of the most affected countries, this sector occupies most of the population, this impact will be far-reaching and in the long run threatens the food security of areas or entire countries. However, the future impact will depend partly on the possibility of mechanizing agricultural production and reducing reliance on labour-intensive means of production. It is therefore important to review periodically the impact on this sector. It is also important to point out that the agriculture sector in the most affected countries is already facing a number of other crises, such as desertification and the neglect of the traditional farming sector by governments. FAO observed that the HIV/AIDS epidemic was intensifying labour bottlenecks in agriculture; increasing malnutrition; and adding to the burden of rural women, especially those who head farm households. The Impact of HIV/AIDS on Health The HIV/AIDS epidemic has been posing tremendous challenges to the healthcare systems of the developing countries and in particular to those of the most severely affected countries. HIV/AIDS increases the overall health expenditures at the same time it is claiming the lives of doctors and nurses in the developing countries. The impact of HIV/AIDS on the health sector may operate in many ways. First, there may be an increase in the number of health workers affected with the HIV virus. The World Bank estimated that a country with a stable 5 % adult HIV-prevalence rate can expect that each year between 0.5 and 1 % of its health care providers will die from AIDS. In contrast, a country with 30 % prevalence would lose 3-7 % of its health workers to the HIV/AIDS epidemic (World Bank, 1999). Occupational exposure may also affect the supply of health care, as more health workers may contract the disease in the workplace through injuries with HIV-positive patients. The increasing mortality of health professionals in some countries poses a serious threat to the replacement of those who are deceased. Training of new professionals is certainly going to cost more money, while the accumulated experience of those who die is lost forever. The morale of health professionals may also be affected. Indeed, staff taking care of HIV-infected patients may suffer greater stress than other health workers. This may lead to greater staff absenteeism and staff refusing to be transferred to high-prevalence regions within countries. A shortage of nurses and doctors has been observed in the high-HIV-prevalence countries. This shortage is particularly pronounced in rural areas. The AIDS epidemic is also responsible for diverting expenditure towards higher levels of care needed for the AIDS patients. Highly active antiretroviral treatment for AIDS has hardly been available in low-income countries, but this is beginning to change with the establishment of differential pricing schemes for the drugs. In early 2000, the annual cost of the drugs for treating one person was US$10,000-12,000 nearly everywhere, but by the end of 2001 prices as low as US$350 were being offered in some cases (UNAIDS, 2002a). Such prices will mean that many more people can be treated. However, low-income countries with high HIV prevalence cannot be expected to meet, out of their own resources, the cost of extending treatment to all who need it. A study conducted in Rwanda showed that 350 HIV-positive outpatients visited the hospital 10.9 times on average as opposed to only 0.3 times for the general population. The study also revealed that the increased demand for out-patient services was characterized by a considerable inequality—reflecting differential access and command over income (Nandakumar and others, 2000). In summary, the studies conducted on the impact of HIV/AIDS on the health sector show that the magnitude of the impact is high. Absenteeism and deaths of health workers pose a serious threat to the health system of the most affected countries. Moreover, because the treatment of AIDS is expensive, few public health sectors in the developing world can afford it with the meagre budget devoted to health. Figure 4 shows that the part of the health expenses covered by the public sector is as low as 28 % in the United Republic of Tanzania. Thus, rising costs will fall mainly on the private sector and households. Overall, the studies conducted have shown hat the health sector in the most affected countries is stretched beyond its limit with the increasing demand due to the HIV/AIDS epidemic. Coping strategies need to be devised by Governments to avoid the collapse of the health system in these countries. The Impact of HIV/AIDS on Education HIV/AIDS affects the education sector through three main routes: the supply of education through the availability of experienced teachers, the demand for education (number of children enrolled in school) and the quality of education. The absenteeism of teachers from school and ultimately their death affects the supply of education. Teachers who are infected with the HIV virus may try to transfer to another area or, once visibly ill, disappear (Katahoire, 1993). Other teachers may also want to transfer out of heavily affected areas or refuse to be posted to them, thus decreasing the supply of education available in the region. The deaths of children or parents may affect the demand for schooling, as a smaller number of children will be entering the school system and more children will be dropping out of school to take care of sick parents or siblings after the death of their parents. The number of children entering the school system is expected to diminish if AIDS orphans do not enroll, delay enrolling, or leave school in large numbers. Equally important is the possible decrease in education quality as teachers may be absent from school and may not be able to provide the same quality of schooling they were providing before becoming sick. Many studies have been conducted to estimate and predict the impact of AIDS on education. A number of studies undertaken under the auspices of UNICEF reached the conclusion that because of AIDS, many countries will be facing a shortage of teachers in the near future. For instance, a study conducted in Zambia using a model developed by UNICEF showed that of around 1.7 million primary school students, 56,000 would have lost a teacher to AIDS in 1999. The study also found that the number of teachers’ deaths in 1998 was equivalent to the loss of about two thirds of the annual output of newly trained teachers (UNICEF, 2000). The same UNICEF study estimated that 860,000 children have lost a teacher to AIDS in sub-Saharan Africa (table 4). Among them, children from South Africa, Kenya, Zimbabwe and Nigeria are the most affected. In Malawi, 10 % of education personnel in urban areas are estimated to have died of AIDS by 1997, and by 2005, it is projected that this figure will increase to 40 % (World Bank, 1998). HIV/AIDS is also affecting the demand for education. For example, focus group discussions with AIDS-affected households found that these households were unable to meet the costs of children’s education as a result of AIDS. Furthermore, an analysis of 49 case studies of families affected by AIDS throughout Zambia found that 56 of 215 children had been forced to leave school (Haworth and others, 1991). In most countries affected by the HIV/AIDS epidemic, the school-age population is projected to continue to grow in spite of HIV/AIDS. But in a few countries, recent projections of the United Nations Population Division suggest that some of the countries most severely affected by HIV/AIDS will show a reduction in the school-age population. In Zambia, projections yield a population under age 15 at 5.8 million by 2010, 1.4 million less than it would have been in the absence of AIDS (Hunter and Fall, 1998). Despite the limitations in the availability of reliable data, the currently available evidence points nonetheless to a tremendous impact of the HIV/AIDS epidemic on the demand for education, on the education supply and, to a lesser extent, on the quality of education. Many questions remain unanswered, though. For example, is there any difference in the school attendance of children whose parents have AIDS but are still alive and children who are AIDS orphans? Does the situation of AIDS orphans regarding schooling change over time? What are the mitigating factors? Follow-up studies need to be conducted to document these changes over time. Because most of the studies conducted so far have used small samples, their results may be hard to generalize. It is therefore important to undertake studies using large samples so as to allow in-depth examination of factors affecting the supply, demand and quality of education. Although some studies have mentioned that teachers are dying of AIDS at a higher rate than the general population, the evidence on this is weak. More needs to be done to investigate this claim. The Impact of AIDS on the Economy The impact of the HIV/AIDS epidemic on the economy as a whole is an issue that has been addressed since the beginning of the pandemic. There have been claims that the HIV/AIDS epidemic is responsible for slowing the rate of growth of the gross national product (GNP) of many heavily affected countries and that in some cases, GNP could decrease by more than 1 % for every 10 % HIV prevalence (Cuddington, 1993, Haacker, 2002). Others have found no evidence of an impact on the macro-economy so far (Bloom and Mahal, 1995). It is difficult to estimate the effect of HIV/AIDS on a country’s macro economy because so many factors other than the HIV/AIDS pandemic affect the long-term economic growth. The most affected countries in the world are also faced with drought, war and other problems. There are a number of ways in which the HIV/AIDS epidemic could affect the economy: (i) First, the AIDS epidemic may reduce the labour supply, leading to reduced output. This may be particularly true in the labour-intensive sectors where replacement of workers is not easy to achieve. (ii) Savings of families will be reduced due to the increase of HIV/AIDS-related health expenditures (drugs and hospitalisation), leaving less income to invest in the economy, and the children’s education. (iii) The AIDS epidemic may divert business and governmental investment funds from other vital sectors to health expenditures, leading to a slower growth of the gross domestic product (GDP). (iv) The HIV/AIDS epidemic may deepen the poverty of the most affected countries by decreasing the growth rate of per capita income and by selectively impoverishing the individuals and families that are affected. A variety of economic modeling approaches have been employed to estimate the macro-economic effects of the HIV/AIDS epidemic. In most cases the focus is on estimating effects on growth of GDP or GDP per capita. Sometimes effects on intermediate outcomes, such as saving and investment, are also estimated. In interpreting the estimates of the epidemic’s effects on the macro-economy, it should be borne in mind that economic forecasting is not an exact science. “It cannot be said that econometric modelling has a good track record. Also, it should be readily admitted that we know relatively little about those structural relationships which are important for estimating the impact of HIV on development “ (Cohen, 1992). Despite the controversies and uncertainties that surround such estimates, there remains a need for policymakers to try to understand the impacts that HIV/AIDS may have on overall performance of their economies and their budgets. Results of estimation and modelling exercise vary, depending on the modelling approach as well as on the national context. Dixon, McDonald and Roberts (2002) reviewed 11 studies that attempted to quantify the effect of HIV/AIDS on GDP per capita in Africa. Some of the studies employed a neoclassical growth model fitted to the data of a particular country, and others used cross-national data and regression analysis. “The consensus from these studies is that the net effect on growth of GDP per capita will be negative and substantial. The more recent studies show greater effects; and the most recent estimates indicate that the pandemic has reduced average national growth rates by 2-4 % a year across Africa” (Dixon, McDonald and Roberts, 2002). How large are these effects in comparison to other factors affecting economic growth? Some analysts note that other factors can produce effects on economic growth that are at least as large as those estimated to result from the spread of HIV/AIDS. For instance, Greener (2002) notes that a reduction in the rate of growth of GDP by between 0.5 and 2.6 percentage points, which encompasses the size of the effect indicated by most studies, “is within the range of variation that could be caused by poor economic management or fiscal policy. This implies that the macroeconomic impacts of HIV/AIDS, in themselves, can be substantially reduced by appropriate policy interventions (Greener, 2002). However, the longer-term effects on the economic may be more serious than most macro-economic estimates suggest. Estimates of AIDS’ effects on macro-economic performance usually take no account of the loss of “social capital” or of the long-term damage that is accruing to human capital, as children’s education, nutritional and health suffer directly and indirectly as a consequence of HIV/AIDS. The effects of lowered investment in the human capital of the younger generation will affect economic performance over future decades, well beyond the timeframe of most economic analyses (MacPherson, 2003; Bell, Devarajan and Gersbach, 2003). While many of the studies discussed here deal with quantifiable economic effects of the HIV/AIDS epidemic, the concept of “development” implies more than material advancement. A nation’s achievement of a long and healthy life for its population is itself one of the main defining features of successful development, as is highlighted, for example, by UNDP’s Human Development Index (HDI), which is a combined measure of mortality, education and per capita income. Cohen (1997) and Gaigbe-Togbe (2001) show that HIV/AIDS affects the HDI through its impact on life expectancy at birth. Based on empirical evidence of societies’ economic valuation of a death, the epidemic’s effect on mortality itself represents a loss of welfare that dwarfs the estimated effects of HIV/AIDS on GDP (Jamison, Sachs and Wang, 2001; Crafts and Haacker, 2003). CONCLUSIONS The HIV/AIDS epidemic has already had a devastating demographic impact, especially in sub-Saharan Africa. Recent United Nations population projections show even more drastic losses over the coming decades. Households are the first units affected by the HIV/AIDS epidemic. The death of a breadwinner may lead to the impoverishment of the household. Children are being taken out of school to care for ill parents or for financial reasons whereas grandparents are acting as surrogate parents to care for their grandchildren. HIV/AIDS is also having a sizeable impact on the labour force, costs and productivity of business firms in the areas with high HIV prevalence. The impact of HIV/AIDS on agriculture is also considerable in the most affected countries. Indeed, the impact in this sector will be far-reaching and threatens the future food security of areas or entire countries. The health sector is often heavily impacted by HIV/AIDS. The increase in the number of persons seeking medical services and the higher costs of health care for AIDS patients are crippling the already inadequate health systems of the most affected countries in the developing regions. The sector is losing its personnel because of the disease, higher costs and AIDS related stress of the medical staff. In the education sector, the pool of qualified teachers is also shrinking in countries or areas with high HIV prevalence. So far, the studies on the impact on macro-economy points to at least to a difficulty in estimating the real impact of AIDS on the economy. However, the impact of HIV/AIDS on economy and development is likely to intensify in the near future. Many countries are still experiencing a rapidly rising prevalence of the HIV and the effects will play out over many years. Most of the available studies on the impact of AIDS on the economy covered the southern part of Africa. Few studies are available on West Africa or on Asia. This may be explained by the relatively low prevalence of HIV/AIDS in these regions. Thus, the organization of studies in these regions should provide insight on the ways in which the HIV/AIDS epidemic affects development under diverse socio-economic and cultural conditions. In the most affected countries, the HIV/AIDS epidemic exacerbates existing problems and dysfunctions of the socio-economic system of a region or a country. Indeed, these countries are already faced with many obstacles on their road to development, including famine, war, inefficient governance and illiteracy to name a few. Poverty, illiteracy and other health programs are also crying out for attention whilst the HIV/AIDS epidemic is causing unforeseen ravages. Mitigating policies and programmes need to be devised and implemented in order to ease the suffering of entire population and future generations. Only prevention, treatment and increased support will allow the countries affected and the international community to reverse or at least reduce the dire-predictions of the implications of the HIV/AIDS epidemic. REFERENCES
Notes [1] The views expressed are those of the authors and are not necessarily those of the united nations 2 The authors are with the United Nations Population Division. This paper is based on the United Nations publications The Impact of AIDS (United Nations, 2003a) and The HIV/AIDS Epidemic: Its Social and Economic Implications (United Nations, 2003b). The contributions of Joseph Chamie, Larry Heligman and Elizabeth Gould of the United Nations Population Division are gratefully acknowledged. [3] List of the 38 African
countries for which the demographic impact of AIDS was explicitly factored in
the estimates and projections for the 2002 Revision of World Population
prospects: Angola, Benin, Botswana, Burundi, Burkina Faso, Cameroon, Central
African Republic, Chad, Congo, Côte d'Ivoire, Democratic Republic of the Congo,
Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Gambia, Ghana, Guinea,
Guinea-Bissau, Kenya, Lesotho, Liberia, Malawi, Mali, Mozambique, Namibia,
Nigeria, Rwanda, Sierra Leone, South Africa, Sudan, Swaziland, Togo, Uganda,
United Republic of Tanzania, Zambia, Zimbabwe. Copyright 2004 - Union for African Population Studies The following images related to this document are available:Photo images[ep04034t3.jpg] [ep04034t1.jpg] [ep04034f4.jpg] [ep04034f1.jpg] [ep04034f3.jpg] [ep04034t2.jpg] [ep04034f2.jpg] [ep04034t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}