 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 19, No. 2, Sup. B, 2004, pp. 139-164 Disability among the Children of Migrants in South Africa[1] Kevin J A Thomas University of Pennsylvania, Philadelphia
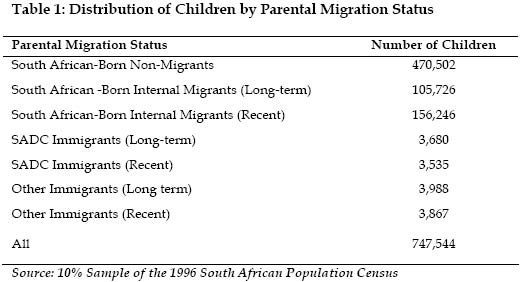
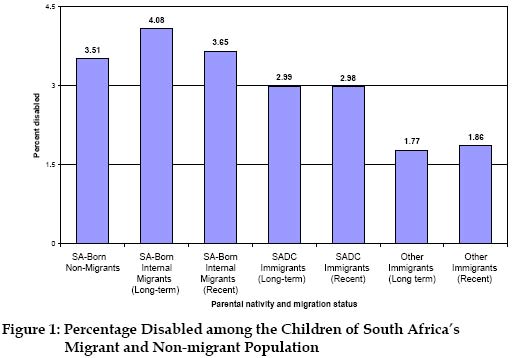
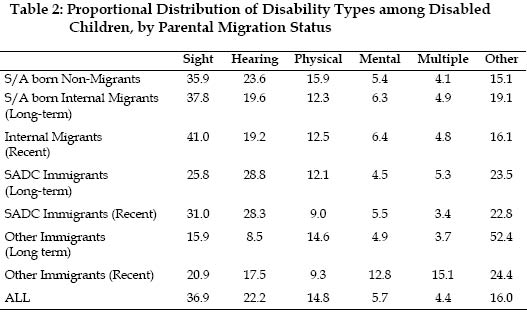
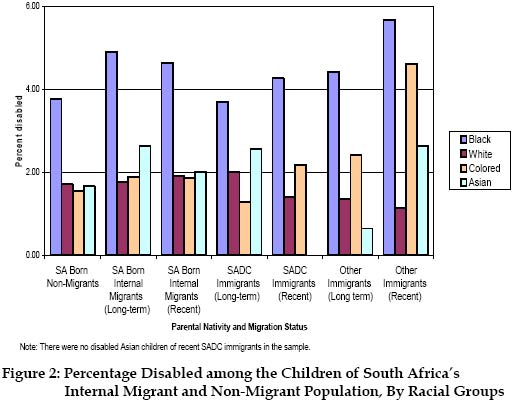
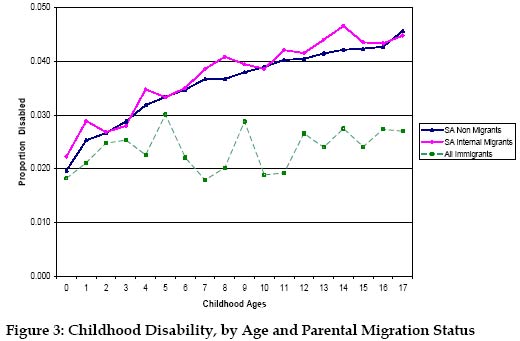
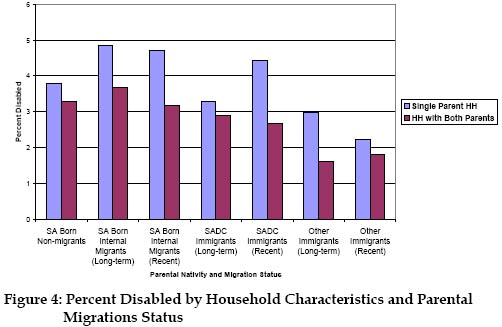
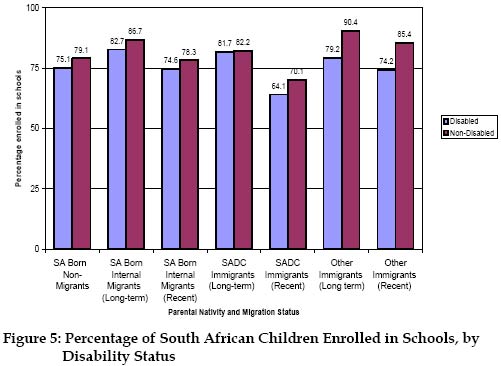
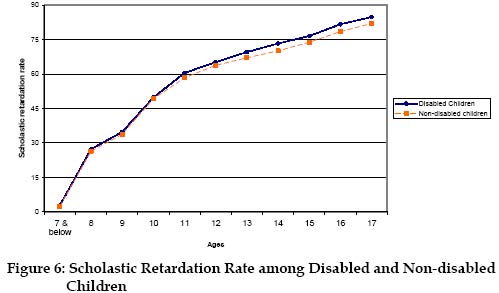
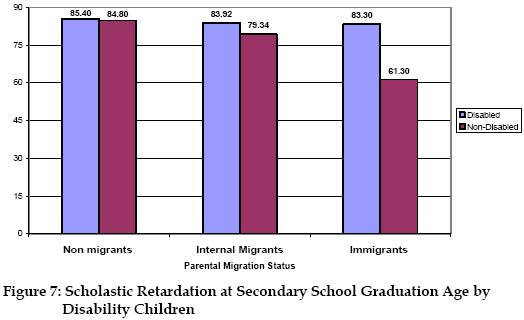
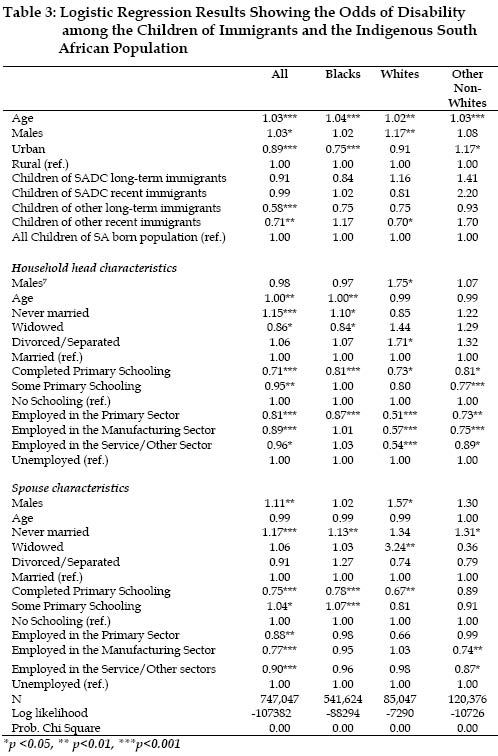
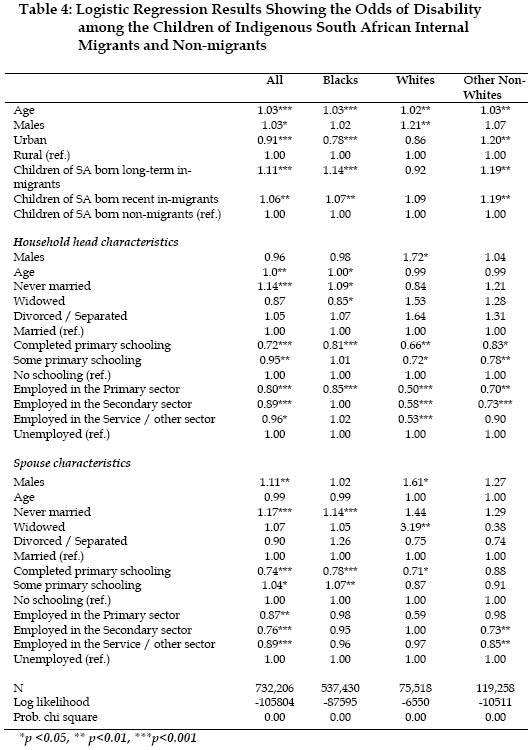
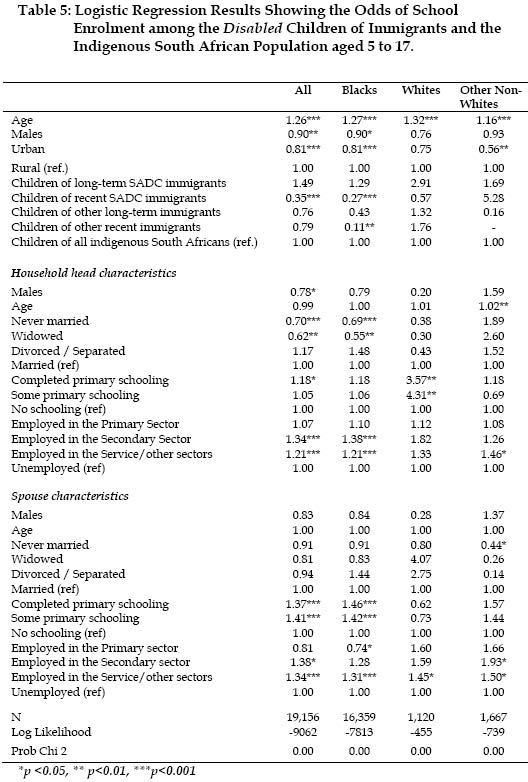
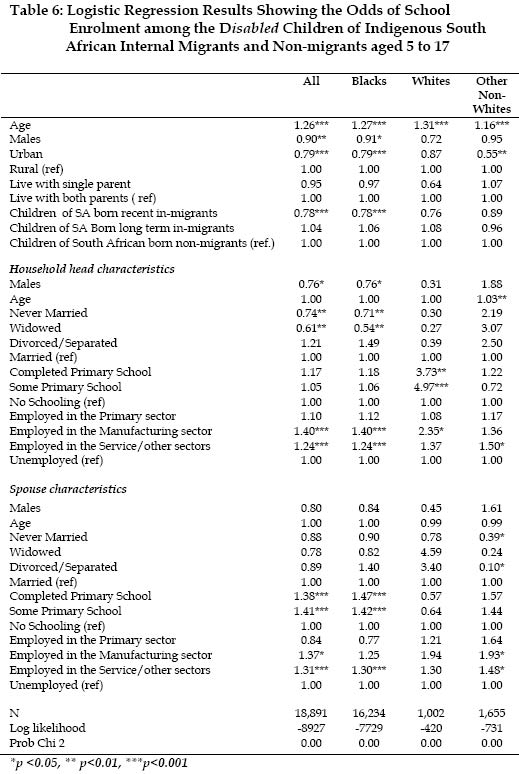
This study describes the relationship between child disability and parental migration status in South Africa. The results indicate that though the children of immigrants were generally less likely to be disabled than those of the native-born population, the immigrant advantage was significant only among the children of immigrants from countries that are not a part of the South African Development Community (SADC). Additionally, the children of South African-born internal migrants were more likely to be disabled than the children of South African-born non-migrants. The study also examines school enrolment among disabled children. Our results show that disabled children of immigrants were more likely to graduate from secondary school at younger ages than were the disabled children of internal migrants and non-migrants. However, the disabled children of recent SADC immigrants were less likely to be enrolled in schools than those of native-born South Africans. INTRODUCTIONMost studies on the health outcomes of children of migrants have compared the health status of the children of immigrants with that of the children of the native-born population. These studies have yielded ambiguous results. For example, Preston et al (1993) observed child mortality levels higher than the levels of the native-born US population among French-Canadian immigrants in the US. On the other hand they observe comparatively lower child mortality levels among Jews living in the US than among the native-born US population (Preston and Condran 1993). Generally, when immigrants have been found to have better health outcomes than the native-born population, immigrants’ superior health has mainly been attributed to selection or ‘healthy migrant’ effects, i.e. people in poorer health are less likely to migrate (Findley 1988). Health migrant effects are however stronger for adult than for child migrants. Children in poor health, like most other children, generally travel with adults during the migration process. As such, Preston et al (2001) maintain that migration rates in the childhood ages reflect the migration levels of parents. This study uses census data to examine disability among the children of non-migrants and different groups of migrants in South Africa. Census data are limited in their ability to explain why differences in disability levels exist among children of the different groups in this study. As a result, the study is mainly descriptive and focuses on identifying empirical patterns of disability among South Africa’s children. The study attempts to achieve several objectives. Firstly, it compares child disability among the children of immigrants with that among the children of the native-born population. Secondly, it describes child disability patterns by age, race, and parental migration status of the children in the study. Thirdly, the study examines the factors associated with child disability in South Africa by modelling disability among the children of the different groups, controlling variables that account for parental socioeconomic characteristics. Additionally, the study compares the likelihood of school enrolment of disabled children and their non-disabled counterparts and investigates the odds of school enrolment of the disabled children of the different migrant groups. Child disability is an important health status indicator that can provide insights into the morbidity levels of migrants in their host societies. The study of child disability among the children of migrants in South Africa is important for several reasons, one of which is the fact that it informs the debate on whether migrants make a major contribution to the health/disease burden in South Africa (Vletter 2000; Zinyama 2000). Child disability can alsonegatively affect the contribution to labour force activity of parents with disabled children (Breslau et al., 1982). This is of particularsignificance whenmigrantparents are perceived as economic migrants who are primarily in their host societies in search of work opportunities. High levels of disability among the children of migrants may thus reinforce negative local perceptions of migrants as being a burden to their host societies, because of migrants’ disability demands on the health system and their consequent sub-optimal contributions to labour force activity. Health and Disability in South Africa Disability, illness and other compromised states of well being constitute critical dimensions of health that are important in understanding morbidity patterns in a population (Murray and Chen, 1992). The disability profile of a population can thus be used to make inferences about its morbidity levels. Data from the 1996 South African Population Census indicate that 6.5% of the total population reported having at least one type of disability, a majority of which was sight/visual related (Statistics South Africa, 1999). According to the 1996 census most disabled people in South Africa were females (55%) and this is of particular significance because disabled women in South Africa are more likely to be poor, illiterate or malnourished than women who were non-disabled (South African Government 1997). In addition, a large proportion of South Africa’s disabled were Blacks (87%). Among the adult population of South Africa, observers have noted that disability may be associated with the consequences of structural violence during the apartheid era (Cock, 1989; South African Government, 1997) and the occupational demands on manual labour (Scott, 1999). Disability levels could also be indirectly associated with the use or adequacy of primary health care services. This association is particularly strong in rural areas in Africa where many severely disabled people die because of the lack of supportive services and resources or face additional complications that arise from the lack of medical supervision and treatment (Disabled People of South Africa, 2003; Cock, 1989). Very limited research has been done on child disability in South Africa, either among migrants or among the native-born population. Available evidence, however, indicates that 80% of Black children with disabilities in South Africa live in extreme poverty and in inhospitable environments (South African Government, 1997). South African children with disabilities are less likely than their non-disabled siblings to attend school, to have access to youth development programs as teenagers and to be employed when they become adults (South African Government, 1997). There is thus a strong association between the limited educational opportunities for children with disabilities and their limited access to employment opportunities when they become adults. Disability among children in South Africa also has implications for the welfare of their families, whose ability to cope with their child’s disability is very limited. For example, in South Africa, it is estimated that 98% of mothers of children with disabilities in rural areas are semi-literate or illiterate single women (South African Government, 1997). Disabled children more generally require more attention and resources and are especially vulnerable to poverty than non-disabled children. They need more assistance with activities of daily living, and such added assistance can disrupt family life and reduce time, energy and resources available for other activities (Mauldin, 1992; Green, 2002). In addition, chronic conditions in childhood have been found to be associated with divorce among married couples (Mauldin 1992).The effect of child disability on parental resources however varies with the age of the child, and becomes stronger as the disabled child grows older and as the permanency of the disability of the child becomes more apparent with age. Disabled children are also sometimes viewed as bearers of negatively valued traits and they and their families can experience emotional distress and social isolation (Green, 2002; Odom, 2002). For migrant families with disabled children these factors can in turn affect their adaptation in their host societies. An examination of the disability status of the children of migrants in South Africa presents us with an opportunity to examine the health of migrants in a very unique context. This is particularly true because of existing inequalities in health status and access to health care that occur between particular groups within the South African society. Differential access to health care in South Africa, a legacy of 40 years of apartheid, means that health status and the burden of disease are differentiated according to skin color and mostly in favour of Whites (Brown, 1987; Marks and Anderson, 1987; Cameroon,2003).Cameroon, for example, discovers that the physical growth of White children in South Africa is superior to that of their non-White peers (Cameroon, 2003). Marks and Anderson (1987) also note that the apartheid system in South Africa led to the decimation of the Black population by preventable diseases and negatively affected family life and human health under the migrant labour system. Existing health inequalities in South Africa have far reaching implications for the disability levels experienced by different migrant groups. As observed by Bollini and Siem (1995), different migrant and ethnic groups have different health entitlements and may experience different outcomes based on their position in society. Bollini and Siem argue that access to health care, particularly for migrants from seemingly disadvantaged groups, is normally limited by economic, linguistic, cultural and administrative barriers as well as racism and prejudice against the alien culture that is assumed to be inferior. Such issues have particular relevance for the complex nature of race relations in South Africa. Migrants could experience different health outcomes that may also reflect the social and economic context of the segment of the population into which they assimilate (Harris, 1999) and their duration of residence in the host country. This position draws from Portes and Zhou’s patterns of assimilation into segregated and unequal segments of US society that include an upward mobility to a White upper class and a downward mobility into the lower classes (Zhou, 1997). Zhou argues that racial status and duration of residence are among the factors that affect this process. This suggests that the health patterns, including disability levels, of long term immigrants from other African countries, for example, are more likely to be affected by the same social environment and structural inequalities that are associated with the poor health outcomes of the Black population in South Africa. DATA AND METHODS The data source for this study is a 10 percent probability sample of the 1996 South African Population Census. These data provide information on individual demographic variables such as age, sex, race, as well as variables such as completed years of schooling and occupation. In addition, these data provide migration related information, such as data on place of birth, duration of time since individuals migrated to their current places of residence and their country of citizenship. This study compares disability outcomes of children below 18 years of age among several migrants groups in South Africa identified by Zuberi and Sibanda (forthcoming). Firstly, it compares disability among children of indigenous South Africans with disability among the children of long-term and recent immigrants. All immigrants are divided into the two categories; immigrants from countries in the South African Development Community (SADC) [2] and immigrants from other countries[3]. Secondly, the study compares child disability among the children of South African born to internal migrants with child disability levels among the children of South African-born non-migrants. Individual and household level data from the 1996 South African Census data are linked in order to place all children within different migrant households. An immigrant household is defined as a household in which at least one of the parents is foreign-born (similar definition are used in Rumbaut, 1999; Hernandez and Darke, 1999). This procedure may misidentify some children such as those who have a native-born father but who now live with their native-born mother who currently lives with a foreign-born spouse. Such biases are however assumed to be unsystematic. Native-born households on the other hand are households in which both parents were born in South Africa. Native-born households are further divided into three different groups i.e. non-migrants, long-term internal migrants and recent internal migrants. Non-migrant South African households are those that have never changed their place of residence, long-term migrant households are those that changed their place of residence prior to the end of apartheid in South Africa in 1994 and recent migranthouseholds are those that changed their place of residence between 1994 and 1996 (Zuberi and Sibanda forthcoming). Distinguishing between long-term and recent migrants helps uscapture period effectsin child disability levels among the children of all migrants (immigrants and internal migrants) in South Africa[4]. The 1996 South African Population Census also had measures of different types of disability – sight, hearing, physical, multiple and mental. For purposes of this study, a child is coded as being disabled if s/he reports any type of disability[5]. The measurement of whether or not a person had a serious disability was based on subjective reports. The identification of a disability depended on the respondents’ interpretation of what constituted a serious disability. However, the interviewer was allowed to clarify that a serious disability was one that prevented the respondent from performing normal activities of daily living such as getting out of bed, dressing, bathing and the like. Even though these data contain only self-reported disability measures, it is not expected that these subjective measures would compromise the results of this study. Self-reported indicators have been found to be reliable measures of health status particularly with regard to the World Health Organization’s definition of health, as a state of well-being and not necessarily the absence of disease (Idler and Kast, 1991; Ross and Mirowsky, 1999). The study then models child disability using dichotomous logistic regressionmodels (i.e. disabled = 1; non-disabled = 0) that control child demographic characteristics such as their age, sex, place of birth, and their type of residence (i.e. urban or rural) as well as several variables that control the socioeconomic characteristics of their household heads and the spouses of their household heads which are used as proxy estimates of children’s household socioeconomic characteristics. These models also include controls that will facilitate the comparison of child disability among the children of the members of the different migrant groups. The study also compares school enrolment of disabled children aged 5 to 17 with that of non-disabled children in the same age range. Additionally, the odds of school enrolment among disabled children of the various migrant groups are estimated using other logistic regression models. RESULTS Descriptive Results As shown in Table 1, the majority of the children in the sample were born to South African-born non-migrant parent. They constituted 63% of the total sample. Disability levels varied among the children of the different migrant groups in South Africa. The highest levels of child disability were recorded among the children of the different groups of the South African born population i.e. the children of South African born non-migrants as well as those of long and short term internal migrants (see Figure 1). The children of long-term internal migrants were most likely to be disabled. Children of the different immigrants groups generally had lower levels of disability compared to the children of all groups of South Africans. This is consistent with the results of other studies (e.g. Guendelman, Hudes and Eskenazi 1980; Beiser et al., 2002) that have reported an immigrant health advantage. Among the children of immigrants, the proportions disabled were higher among the children of SADC immigrants compared to disability levels among the children of other immigrants. However, there was hardly any difference in the proportions disabled among the children of long-term and recent SADC immigrants. The lowest percentage of disabled children was found among the children of other long term immigrants. The distribution of the different types of disabilities among disabled children in South Africa is presented in Table 2. Except for multiple disabilities, each type of disability was recordedwhen itwasthe only type of disability a child had. Other types of disabilities refer to disability types that were not specified in the census questionnaire such as disabilities due to chronic health problems such as epilepsy and cerebral palsy, congenital anomalies such as cleft palates and disabilities due to conditions such as Down syndrome. As shown in Table 2, sight related disabilities were more prevalent among children of the South African-born population particularly among the children of recent internal migrants. Hearing disabilities ranked second in terms of prevalence and was particularly predominant among the children of SADC immigrants. Mental disabilities and multiple disabilities were the least prevalent among all children in South Africa. The highest percentages of children with other types of disabilities were recorded among the children of other immigrants particularly among the children of other long-term immigrants among whom other disabilities accounted for over half of the disabilities. Disability by Race, Age and Household Characteristics Disability among children in South Africa also varies among children of the different races. Figure 2 shows the percentages disabled among the children of South Africa’s migrant and non-migrant population, by racial group. It suggests that the high proportions of Black and Colored disabled children of other immigrants in South Africa who migrated after 1994 (i.e. among other recent immigrants) may be the reason for the higher proportion disabled among the children of other recent immigrants compared to those of other long-term immigrants shown in Figure 1. Similarly, Figure 2 suggests that the lower percentage disabled among the children of recent internal migrants compared to the children of long-term internal migrants shown in Figure 1, may in large part be due to lower proportions disabled among Black and Asian children of internal migrants who migrated after 1994 (i.e. recent internal migrants). Figure 2 also presents a conspicuous health or disability disadvantage among all Black children compared to the children of other races, in all the different groups. It also demonstrates an increasing likelihood of disability among Colored children of most immigrant groups (except for the children of long-term SADC immigrants) compared to Colored children of the South African born non-migrant and internal migrant population. The disability disadvantage of Black children can be attributed to two reasons. Firstly, it may reflect the effect of structural factors, such as racism, that continue to maintain differential access to health care and resources among different racial groups. The prevalence of such factors in South Africa is discussed by Cameroon (2003) and more generally discussed by Williams and Collins (1995). Additionally, differences in child disability by race could also reflect differences in the accumulation of health stocks over the life course of immigrants that could be traced to their different places of origin. Compared to White and Asian immigrants, a majority of Black immigrants in South Africa are from poorer countries in Africa. These include Black immigrants from SADC countries and those in the ‘other immigrants’ category who are mainly from other African countries. Socioeconomic conditions at the different places of origin may account for differential processes of wear and tear of the body that arise from exposure to high and repeated stress (Smith, 1999). The cumulative toll of such processes could have had a negative effect on the health outcomes of immigrants and their children. Further analysis of child disability, by age, revealed unique variations in the age patterns of child disability observed among children by the migration status of their parents. As Figure 3 illustrates, the levels of disability were generally highest among children in the older age groups compared to those in the younger ages particularly among the children of native-born internal migrants and non-migrants. Such a pattern suggests an accumulation of disabilities as exposure to health risks increases with age (Case, Lubotsky and Paxson, 2002). The exception to the positive relationship between age and the percentage disabled is seen among the children of immigrants. The age pattern of disability observed among thechildren of immigrants was distinct in two ways. Firstly, unlike thechildren ofSouth African born internal migrants and non-migrants the age pattern of disability among the children of immigrants showed a less distinct pattern of increasing disability with age. This pattern suggests that the children of immigrants were less likely to accumulate health risks as age increased. Secondly, the percentages of the children of immigrants disabled at each age were lower than those observed among the children of native-born internal migrants and native-born non-migrants in similar age groups. In fact, the differences in the proportion disabled between the children of immigrants and those of native-born South Africans increased as age increased. Disability also varied by the characteristics of the households in which the children lived. Previous studies e.g. Weitoft et al. (2003) discovered higher mortality and morbidity levels among children living in single headed households. This health disadvantage has been associated to the socioeconomic disadvantage of such households and their unique childcare arrangements that are necessitated by the absence of the spouse of the household head. Among South African children, a strong relationship emerged from the analysis of child disability by parental migration status and household characteristics. Figure 4 shows that child disability levels were higher among children living in single parent households than among those who lived in households with both parents. The percent disabled in single parent households were however lower among the children of the different groups of immigrants. School Enrolment among Disabled Children The age range of South African children in our sample enables us to examine school enrolment among the disabled child population of school going age (i.e. age 5 to 17). Though it has earlier been noted that disabled children in South Africa are generally less likely to be enrolled in school than their non-disabled counterparts, the association between schooling and later employment as adults suggests a further examination of the likelihood of school enrolment among the disabled children of the different migrant groups. The percentage enrolled in school among children in the sample was higher for non-disabled children (80.7%) than it was for disabled children (76.7%). However among disabled children, school enrolment was lowest for the children of the South African born population (76.8%), including non-migrants and internal migrants, than it was for the children of all immigrants (79.2%). Figure 5 shows the percentage of children age 5 to 17 of the migrant and non-migrant populations, who were enrolled in schools, by their disability status. Disabled children were less likely to be enrolled in schools than their non-disabled counterparts in all the groups shown in Figure 5. The differences the percentage enrolled in school among disabled and non-disabled children in South Africa were largest among the children of long-term and recent immigrants from other countries. Among disabled children, the percentages enrolled in schools were highest among the disabled children of all groups of long-term migrants (both internal migrants and immigrants). Disabled children of recent internal migrants and otherrecent immigrants had percentages enrolled that were comparable to that of the disabled children of South African born non-migrants. The lowest levels of school enrolment among disabled children were recorded among the children of recent SADC immigrants. Overall, the results presented in Figure 5 point to the fact that the disabled children of all migrants (i.e. internal migrants and immigrants) are more likely to be enrolled in school as duration of residence increased. Additional insight into schooling patterns among children of schooling age in South Africa can be derived from the analysis of their scholastic retardation rates. These are ratios that define the relationship between a child’s age and the grade in which he/she is enrolled. According to Shryock et al. (1975), a student is scholastically retarded if the grade in which he/she is enrolled is below thatwhich is normally expected for his/her age. They further define the scholastic retardation rate by the following formula: Where, Figure 6 illustrates the scholastic retardation rates for children by their age and disability status. It assumes that children in South Africa enter grade 1 at age 5 and complete their secondary education around age 17. Though the scholastic retardation rate generally increases with age among children in South Africa, disabled children are generally more likely to be scholastically retarded than non-disabled children in all the childhood ages. Furthermore, the differences in scholastic retardation among disabled and non-disabled children increase with age, being lowest among children aged 7 and below and highest among those in their late teens. When the scholastic retardation rates among children aged 17 (i.e. those at the end of their secondary schooling career) are examined by parental migration status, we still find higher scholastic retardation rates among the disabled children of non-migrants, internal migrants and immigrants compared to their non-disabled counterparts. As shown in Figure 7, the differences in scholastic retardation rates at age 17 among disabled and non-disabled children were highest among children with immigrant parents. Additionally, the lower scholastic retardation rates at age 17 among the children of immigrants, compared to the children of internal migrants and non-migrants points to the fact that the children of immigrants were least likely to lag behind as they moved from one class to another. This in turn suggests that they were more likely to complete their secondary education at an earlier age. Multivariate Analyses How do the odds of disability among children in South Africa vary by period of migration and parental migration status? Logistic regression models are used to answer this question from two different perspectives. Firstly, the odds of disability among the children of immigrants are compared to the odds of disability among all the children of the South African born population (Table 3). Secondly, we compare the odds of disability among the children of South African born internal migrants with the odds of disability among the children of the South African born non-migrants (Table 4). The regression models include controls that account for the age, sex, place of residence (i.e. rural or urban) of children and whether or not they lived in a single parent household. Additionally, the models try to capture the influence of household socioeconomic status on child disability by controlling socioeconomic attributes of household heads and their spouses which are considered here as proxies for household socioeconomic status. Such proxies include marital status, level of schooling, and the sector of employment of household heads and their spouses. Sector of employment is further divided into several nominal categories; the primary sector i.e. forestry, agriculture, fishing etc, the secondary sector that consists mainly of manufacturing jobs and the service/other sectors i.e. financial and business services, social services, diplomatic service and the like. Unemployed household heads and unemployed spouses are used as reference categories for the sector of employment variable. a. Differences between the Children of Immigrants and Native-born South Africans Do the children of immigrants have higher odds of being disabled than the children of the native-born population of South Africa? As shown in Table 3, the children of both groups of non-SADCimmigrants (i.e. long-term and recent from other countries) have significantly lower odds of disability than the children of indigenous South Africans. Compared to the children of indigenous South Africans the children of other long-term immigrants had the lowest odds of disability followed by those of other recent immigrants. However, even though children of both groups of SADC immigrants had lower odds of disability than the children of the South African-born population, these odds were not significant. Results from Table 3 indicate that all South African children were significantly more likely to be disabled as age increased.. Male children had higher odds of disability than children who were females. Furthermore, the likelihood of disability among all children in South African was greater if household heads and their spouses were never married rather than married. Child disability was also significantly higher when spouses of household heads had some schooling compared to when they had no schooling. Table 3 also shows several factors associated with decreasing odds of disability. Children living in urban areas in South Africa were less likely to be disabled than those living in rural areas. Some primary or completed primary schooling among household heads significantly decreased the odds of child disability. Additionally, child disability was significantly lower when household heads and spouses of household heads were employed, regardless of sector of employment, than when they were unemployed. The odds of child disability were also significantly lower when spouses of household heads had complete primary education. Among the different races there was a slight variation in the factors associated with child disability. For example, parental immigration status was significantly associated with child disability only for Whites, among whom the children of other recent immigrants were less likely to be disabled than those of the indigenous White population. Living in an urban area was significantly associated with lower odds of child disability among Black children and higher odds of disability among other non-White children (i.e. Colored and Asian children). The disability advantage of Black children living in urban areas is particularly instructive. Rural people in South Africa, particularly Black rural children, are more likely to suffer from preventable and treatable diseases and have limited access to health care (Marks and Anderson, 1987; Cameroon, 2003). Among Whites, there was no significant association between child disability and place of residence. White children, however, faced very high odds of disability when household heads were males and when household heads were widowed while among Blacks the odds of child disability were higher when household heads were never married, compared to when they were married. Sex of spouses of household heads was associated with child disability only among Whites. Additionally, even though there were significantly lower odds of child disability when household heads were employed in any sector among children in the other races, among Blacks this was not so. Black children were less likely to be disabled only when household heads were employed in the primary sector. b. Differences between the Children of Internal Migrants and Non-migrants Is there an association between child disability and parental internal migration status among the children the South African born population? Table 4, which excludes all children of immigrants, provides interesting answers to this question. This analysis concentrates only on the children of South African-born internal migrants and non-migrants. Compared to the children of non-migrant South Africans, all the children of both groups of internal migrants had significantly higher odds of disability. However, Table 4 suggests a positive association between period of migration (i.e. long-term or recent) and the magnitude of the differences in the odds of child disability. The difference in the odds of child disability between the children of long-term migrants and the children of non-migrants was greater than the difference in the odds of disability between the children of recent internal migrants and the children of non-migrants. The factors significantly associated with the odds of disability among children of the South African born population are basically the same as the factors affecting child disability among all children in South Africa, reported in Table 3. There were no significant differences in the odds of disability between the children of long-term and recent internal migrants compared to the odds of disability among children of non-migrants among Whites. Among Black children and other non-White children, the odds of child disability were higher among the children of internal migrants, regardless of duration, than it was among the children of non-migrants. However, the difference in the odds of disability between the children of long-term migrants and the children of non-migrants was the same as that between the children of recent internal migrants and non-migrants for other non-White children. Among Blacks, the odds of disability were significantly higher among the children of long-term internal migrants compared to the odds among the children of non-migrants. c. Odds of School Enrolment among Disabled Children We now turn our attention to school enrolment among disabled children. Investigating school enrolment among disabled children is important for several reasons. Firstly, the child care responsibilities of mothers with disabled children may be negatively associated with mothers’ participation in the labour force (Breslau et al., 1982). This association may become stronger if disabled children are not enrolled in school. School enrolment of disabled children however keeps them away from home and is thus likely to increase parental labour force participation. Additionally, school enrolment of disabled children may be an important factor determining the employment of disabled children when they become adults. The analysis presented here tries to answer the question of whether the disabled children of migrants are more likely to be enrolled in school than the disabled children of non-migrants and concentrates on children between the ages of 5 and 17. It should be noted that school enrolment of disabled children is also determined by the extent to which schools can cater to the specialized needs of such children. This analysis is however restricted to association between the odds of school enrolment of disabled children and the characteristics of children, household heads and spouses of household heads, presented in Tables 5and 6. According to the results presented in Table 5, there are significantly lower odds of school enrolment among all disabled children of recent SADC immigrants compared to the odds of school enrolment among the disabled children of the native-born population. Table 5 also shows that among Blacks, both the disabled children of recent SADC immigrants and those of other recent immigrants had lower odds of school enrolment compared to the Black children of non-migrants. The results show no significant association in the differences in the odds of school enrolment of the disabled children of the other groups of immigrants and the disabled children of the native-born population. Generally, school enrolment among all disabled children in South Africa had a significantly strong association with the employment of household heads and spouses of household heads in the manufacturing sector and the service/other sectors. Disabled children also had significantly lower odds of attending school if they were males, lived in urban areas, and had a male household head that was either never married or divorced. The odds of school enrolment among disabled children of South African born internal migrants and non- migrants are presented in Table 6. Compared to the disabled children of non-migrants all disabled children of recent internal migrants had significantly lower odds of school enrolment. Among the races, this relationship was found only among Black disabled children and this may be due to the fact that a majority of all disabled children in South Africa were Black. Black disabled children were also significantly less likely to be enrolled in school when their household heads were either never married or widowed, unlike disabled children of the South African born population in the other races. White disabled children were significantly more likely to be enrolled in school when household heads had at least some primary schooling compared to when they had no schooling. However, among White children alone, none of the characteristics of spouses of household heads were significantly associated with school enrolment. The age of household headswas a significant factor associated with school enrolment among other non-White disabled children alone. Other non-White disabled children were more likely to be enrolled in school whenhousehold heads were employed in the service/other sectors and when spouses of household heads were employedin themanufacturing sector or the service/other sectors. The results presented in table 6 generally show that there were no significant differences in the odds of school enrolment of the disabled children of internal migrants and non-migrants among Whites and other non-Whites. DISCUSSION AND CONCLUSIONS This study has examined disability among the children of immigrants and the native-born born population in South Africa and among the children of indigenous South African internal migrants and non-migrants. It has also analyzed school enrolment among disabled children of the different migrant groups in South Africa. Generally, the children of native-born South Africans were more likely to be disabled than the children of international migrants, implying that the children of immigrants in South Africa make a lesser contribution to aggregate child disability levels than the children of native-born South Africans. Specifically, however, the comparison of immigrants and native-born South Africans revealed a significant health advantage, in terms of disability status, only among the children of long-term and recent immigrants from non-SADC countries. Among the races, lower odds of disability were observed only among White children of recent immigrants compared to White children of the native-born population. Conversely, the study observed a greater likelihood of child disability among the children of indigenous internal migrants than among the children of indigenous non-migrants. Specifically, even though the children of recent internal migrants were more likely to be disabled than the children of non-migrants, the children of long-term internal migrants had much higher odds of disability than the children of non-migrants. Ironically, unlike children from the other races, there were no significant relationships between the odds of disability among White children of internal migrants and non-migrants. The study has made no attempt to determine why immigrants are less likely to have disabled children than the native-born South African population. Rather, it has identified and described the differences in disability among the children of different migrants groups and has discussed the factors generally associated with child disability and the factors associated with school enrolment among disabled children. The results, however, suggest that the higher odds of disability among the children of internal migrants may have reflected the greater likelihood of disability among all non-White children of internal migrants, the majority of whom were Blacks. These results also show that the disabled children of immigrants were more likely to graduate from secondary school at younger ages compared to the disabled children of internal migrants and non-migrants. However, the fact that disabled children were found to have lower percentages enrolled in schools than their non-disabled counterparts was not surprising. The study’s observation of lower odds of school enrolment among disabled children of recent SADC immigrants compared to the disabled children of the native-born population and the lower odds of school enrolment among disabled children of recent internal migrants compared to those of the non-migrant population is cause for concern. This is because the study’s results point to a strong association between the employment of household heads and their spouses and the enrolment of disabled children. Even though this relationship could potentially be endogenous, it is clear that disabled children are generally more likely to be enrolled in school when their household heads and their spouses were employed. These results thus suggest that attempts to increase school enrolment among disabled children may not only improve economic conditions in the households of disabled children but may also increase the potential contributions that disabled children can make to economic activity when they become adults. REFERENCES
[1] “The African Census Analysis Project (ACAP) in collaboration with Statistics South Africa (STATS SA) Pretoria, provided the data for this analysis” [2] SADC countries include South Africa, Botswana, Lesotho, Mozambique, Malawi, Swaziland, Tanzania, Zambia, Zimbabwe, Namibia, Democratic Republic of Congo, Mauritius, Seychelles and Angola. [3] Immigrants from SADC countries are differentiated from immigrants from other countries because SADC countries are closest to South Africa in terms of distance. SADC countries also seek to promote free movement of nationals among member states. [4] The division of migrant households into ‘long-term’ and ‘recent’ migrant categories may have implications for the examination of disability among the children of migrants. Recent migrant households are more likely to be composed of first generation children than long-term migrant households. This was the case mainly among the children of immigrants from other countries. [5] It is assumed that the parents of infants correctly reported the disability status of their children. [6] Additionally, the scholastic retardation rate allows for the fact that the age at which children enter school varies because of the relationship between their birth dates and the ages permitted by law. For example, among six year olds, children aged 6.1 years could still be in grade 1, while some aged 6.9 years would be in grade two. The “normal” grade for each age is thus a two-year grade span that accommodates such variations. [7] The reference group, female
household heads, is a unique feature of South African households. Female headed
households are mainly found in polygamous families, where “…a mother and her
children stand out definitely as a group…inhabiting its own home” (Hoernle, in
Sibanda 2001). Households could also have female heads because of other reasons
such as divorce, separation, widowhood etc. Additionally, de facto female
headed households may be due the absence of husbands who are migrant workers
Sibanda (2001). The following images related to this document are available:Photo images[ep04039t2.jpg] [ep04039t5.jpg] [ep04039f3.jpg] [ep04039f2.jpg] [ep04039f1.jpg] [ep04039t1.jpg] [ep04039t4.jpg] [ep04039f4.jpg] [ep04039t3.jpg] [ep04039f5.jpg] [ep04039f7.jpg] [ep04039t6.jpg] [ep04039f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}