 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude
de la Population Africaine, Vol. 19, No. 2, Sup. B, 2004, pp.165-177 Chuks J. Mba University of Ghana, Accra - Ghana Code Number: ep04040 ABSTRACTThe paper examines the deleterious effect of external causes, especially road accidents and suicidal behaviour, on South Africa’s expectation of life for possible policy interventions. Employing the multiple and associated single decrement life table techniques, the study estimates the total number of South Africans who would eventually die from external causes by the time they reach age 75 from a hypothetical cohort of 100,000 live births, on the assumption that the mortality conditions of 1996 prevailed. The results of the analysis show that if the prevailing mortality conditions continued throughout their life span, about 9.1 % of the population might eventually die from external causes by the time they attain age 75. This is very high, as demonstrated also by a tremendous gain in life expectancy to the tune of about 17 years that would result in the absence of external causes. Disabilities result from some of these external causes, especially injuries sustained during road accidents, which in turn impact adversely on the economic condition of the victims. This is because the disabled person is unable to work and earn a living, and therefore cannot take care of himself and his dependents. The end result is the perpetuation and worsening of poverty. It is suggested that both the people and government of South Africa should work together to bring about a substantial reduction in external causes of death with a view to ultimately raising the expectation of life of the citizens. INTRODUCTION One vital event that characterizes all societies is death. While every human being will one day succumb to this vital event, people in the developed countries generally live longer than their counterparts in the developing world (United Nations, 2001a; 2001b; World Health Organization, 2001). At the same time, certain deaths, occurring in either a developed or developing country, are not the product of natural causes, and therefore can be avoided. South Africa is one of the leading economies of Africa, although it is still a developing country (World Bank, 2000). The country’s expectation of life is one of the highest in Africa (United Nations, 2001a). However, there are certain deaths, not due to natural causes, which if drastically reduced, will undoubtedly raise the longevity of the citizens. These deaths constitute part of what is called external causes (World Health Organization, 2001). According to the World Health Organization (2001), external causes relate to the sum of the following causes: transport accidents (code E47); accidental poisoning (code E48); accidental falls (code E50); accidents caused by fire and flames (code E51); misadventures during medical care/abnormal reactions (code E49); other accidents (code B52); drugs and medicaments causing adverse effects (code B53); suicide and self-inflicted injury (code B54); homicide and injury purposely inflicted by other persons (code B55); and other violence (code B56). It is conceded that it is impossible to eliminate all these various components of external causes of death in real life. However, the empirical evidence point to the fact that transport (road) accidents account for an overwhelming majority of external causes, followed by homicide and injury purposely inflicted by other persons, though to a much lesser extent. These two aspects of external causes can be drastically reduced. In South Africa and other developing countries, road accidents are rising, and the number of those with fatalities and serious injuries is also increasing considerably. It has been found that while North American and Western European countries have succeeded in checking and even reversing the road accident trend, road accident fatalities rose to more than 350 % between 1968 to 1990 in Africa (Dhliwayo, 1997). Also, in 1990 road accidents ranked number 12 as a cause of death, but it has been projected that by 2020, road accidents are expected to be the number 2 cause of lost disability-adjusted life years in developing countries (Murray and Lopez, 1996). South Africa’s road accident statistics, in particular, bear further horrifying evidence of the large contribution to road fatalities, as well as damage to life and property. In a study by the Council for Scientific and Industrial Research (1995), it was found that one out of every four buses and minibuses in the country was involved in a road accident every year. Also, vehicular accidents cost the country the 12.8 billion rand (the equivalent of US$2.1 billion) a year (Stoppard, 2000). As a result of the high accident rates in South Africa and elsewhere in Africa, and the concomitant loss of life and property, there is the urgent need to raise awareness with a view to combating the deteriorating road safety situation in the country. South Africa’s murder rate is about 1,000 times higher than the world average. The country has the worst record of rape in the world (Nevin, 1998). Also, in the country, as in many other countries, suicide is one of the leading causes of death. In fact, suicidal behaviour constitutes a major public and mental health problem, as well as a considerable drain on resources in both primary and secondary health care settings (Gulbinat, 1996; Leenaars, 1995). Consequently, in the present study, attention will be focused primarily on these two components with a view to raising awareness and expanding knowledge about their deleterious effect on South Africa’s expectation of life for possible policy interventions. In an attempt to achieve this objective, a stochastic procedure will be adopted whereby the life expectancy of the South African society will be simulated in the absence of external causes. Thus, the thrust of this study is to attempt to answer three basic questions. First, what is the contribution of external causes mortality to the overall mortality of South Africa? Secondly, to what extent will life expectancy be enhanced if external causes were absent in the mortality experience of the country? What are the economic implications of the external causes, with particular reference to the dependents of the affected persons and those disabled as a result of the external causes, especially from road accidents? DATA AND METHODS The data for the present study emanate from two sources: The 1996 Census data file of South Africa and the World Health Organization (2001) database. The census data set of South Africa is part of the collection of census micro-data presently archived by the African Census Analysis Project of the Population Studies Center of the University of Pennsylvania, which are used for demographic research and training (Zuberi, 2001). In an attempt to determine the effect of death due to external causes on the overall mortality experience of South Africa, the present study employs the multiple decrement life table techniques (Preston et al., 2000; Namboodiri and Suchindran, 1987; Keyfitz, 1985; Chiang, 1968). The multiple decrement procedures are based on the principle of competing risk; that is, as human beings are exposed to the risk of dying, death could result from various causes. The basic assumption underlying this principle is that the various causes of death are mutually exclusive and exhaustive (Preston et al., 2000; Namboodiri, 1991; Chiang, 1984). The assumption of independence implies that the force of the mortality function from different causes is additive. In South Africa’s specific context, the state of interest is being alive and decrements from that state are attributable to external causes and all other causes of death. Drawing from the conventional life table technique, the force of decrement from all causes combined is the sum of the force of decrement from external causes and the force of decrement from all other causes. That is:
Thus, the force of decrement from cause i at age x is simply the rate at which persons are leaving the defined state from cause i. Because it is not possible in real life situations to observe directly associated single decrement processes, that is, processes in which one decrement alone is operating, certain functions defined for the basic life table can be extended to the associated single decrement life table. Associated with each decrement i in a multiple decrement process is a force of decrement function, μi (χ). In general, the rate of decrement from μi (χ) if i were the only decrement differs from what it would be if i were working in the presence of other decrements. The interest here is to determine the resultant life table, called the associated single decrement life table, if only the external causes (i) of decrement were operating to reduce South Africa’s population. The decrement of interest is simply all decrements other than i (that is, - i). Thus, the task is to construct a table based on μ-i (χ) in which cause i will be arbitrarily deleted from the set of multiple decrements. It should be stated that in the ensuing analysis the estimation of life table functions, such as nax , nqx , ndx , nLx , and so on, follows the usual conventional approach. However, the calculation of the mean number of person-years lived in the interval by those dying in the interval, nax, is based on Chiang’s (1968) approach for ages above age 4, while for children below age 5, the procedure suggested by Coale and Demeny (1983) is adopted. The probability of dying from the external causes, nqix , is computed by applying the proportion of deaths that are due to the external causes to the overall probability of dying between ages x and x+n, nqx ,as indicated hereunder:
where nDix is the observed total number of deaths from external causes between ages x and x+n, and nDx is the observed total number of deaths from all causes between ages x and x+n. In constructing the associated single decrement life table, the constant of proportionality for decrement other than external causes in the interval x to x+n, R-1 is computed using the formula:
Also, the probability of surviving from age x to age x+n in the absence of external causes, nPx -1, is estimated using the following formula proposed by Chiang (1968):
while the average person-years lived between ages x and x+n in the absence of external causes, nax-1, is calculated using the formula:
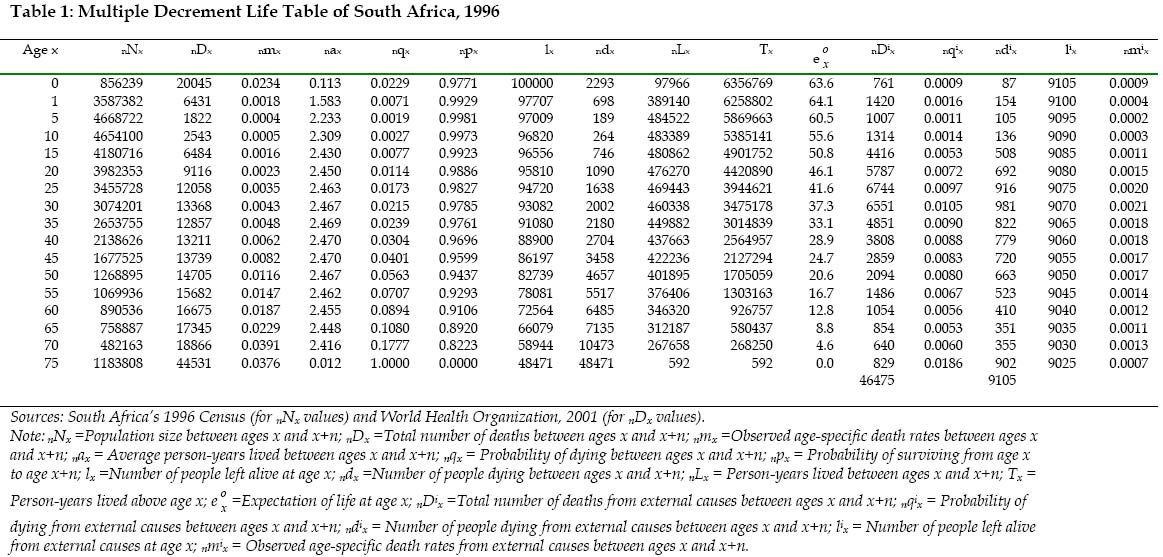
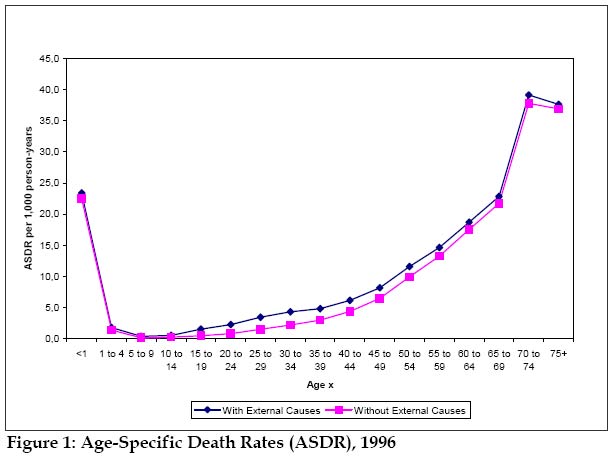
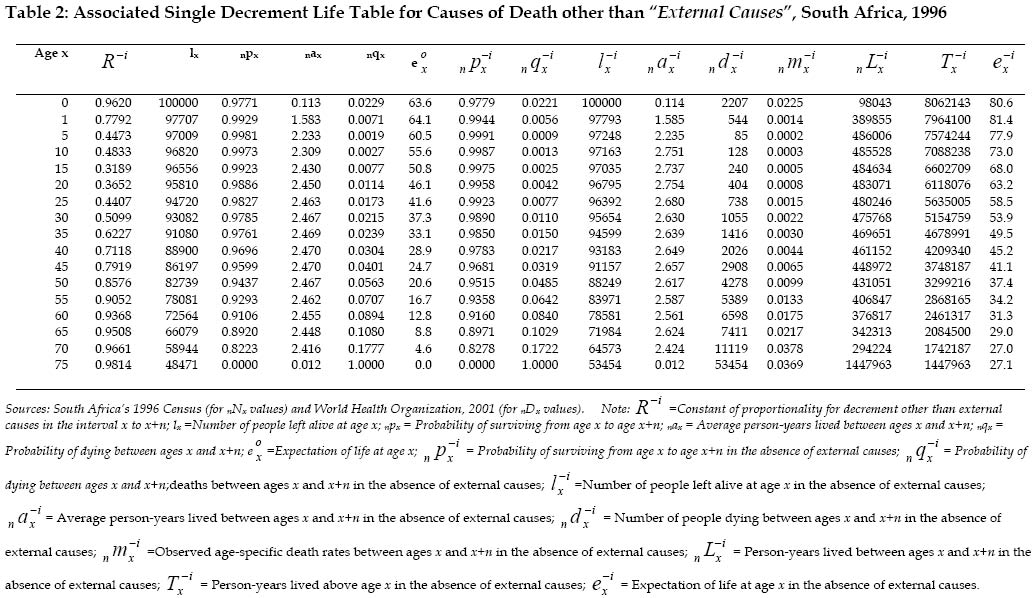
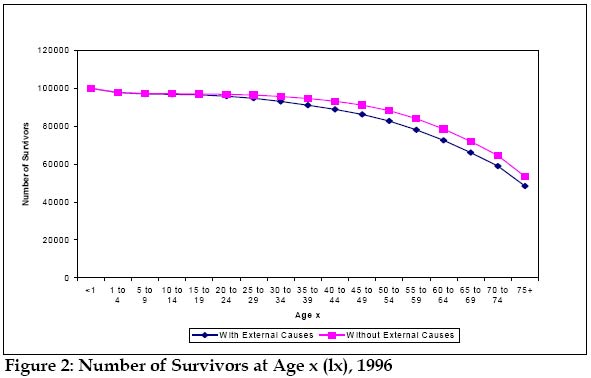
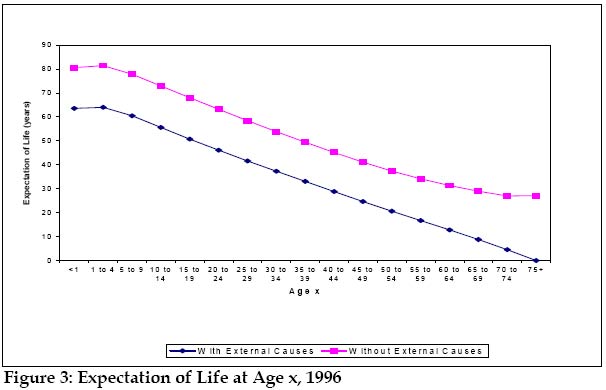
for x=0, 1, 5 (ages under 10 years) and 70 (70-74 age group); but for the intervening age groups, (x=10 to 65), this formula is employed: . RESULTS Table 1 shows the multiple decrement life table of South Africa in 1996 constructed with a view to finding out the contribution of external causes to the overall mortality experience of the country. The findings reveal that the infant mortality rate and under five mortality rate are respectively about 23 deaths per 1,000 live births, and 25 deaths per 1,000 live births. The graphical representation of the age-specific death rates, presented in Figure 1, indicates that mortality is high at very young ages, but declines to very low levels before age 25, and rises gradually up to age 65, and then much more rapidly thereafter. The mortality estimates translate into expectation of life at birth of 63.6 years. This finding is consistent with estimates of life expectancy at birth for the country from other sources (United Nations, 2001a; Udjo, 2001; Republic of South Africa, 1997; Kinsella and Ferreira, 1997). Table 1 further shows that the proportion of new born babies that will eventually die from external causes under the South Africa’s age-cause-specific death rates of 1996 is 9105/100,000=9.1 %. Similarly, under the prevailing age-specific mortality conditions, the proportion of the elderly persons who survive to age 70 that will die from external causes is 9030/58944=15.3 %. A striking feature of Figure 1 is that there is a noticeable improvement in age-specific death rates at all ages, especially after age 15, when external causes is eliminated. Table 2 indicates the associated single decrement life table for South Africa under a hypothetical scenario whereby external causes is deleted to determine the extent of the resultant gain in expectation of life in the country. The findings show that the probability of surviving to age 75 in the absence of external causes is 0.53 (53454/100000), which is higher than 0.48 (48471/100000), the probability of surviving to age 75 for all causes combined. This translates into a gain in life expectancy at birth of 17 years, from 63.6 years for all causes combined to 80.6 years in the absence of external causes. This tremendous gain in both the number of persons surviving to each age and expectation of life is better illustrated pictorially in Figures 2 and 3. Figure 2 shows that the number of survivors increased consistently from age 20 in the absence of external causes. More remarkable are the results displayed in Figure 3. The graph reveals that there is a pronounced gain in life expectancy at every age with the deletion of external causes. DISCUSSIONS AND CONCLUSIONS
Employing the multiple and associated single decrement life table techniques, the present study has attempted to estimate the total number of South Africans who would eventually die from external causes by the time they reach age 75 from a hypothetical cohort of 100,000 live births, on the assumption that the mortality conditions of 1996 prevailed. The results of the analysis revealed that if the prevailing mortality conditions continued throughout their life span, about 9.1 % of the population might eventually die from external causes by the time they attain age 75. This is very high, as demonstrated also by a tremendous gain in life expectancy to the tune of about 17 years that would result in the absence of external causes. It is factual that the number of people killed and injured in road accidents relative to the population in South Africa and elsewhere in Africa has not yet reached the same level as in North America and Europe. Nevertheless, the rate of those killed and injured relative to the number of motor vehicles is extremely high in South Africa and most countries of Africa. It should be stated that death resulting from road accidents has serious consequences for the bereaved, especially if the victim was the breadwinner. The surviving dependent relatives are left without any means of livelihood and are forced to fend for themselves. If these relatives are young, their educational advancement is curtailed; if older, they are abandoned without any financial support. All this heightens poverty and perpetuates social ills such as armed robbery, theft, fraud, and other crimes. These adverse consequences are also the inevitable results in cases where persons in the working age group sustain severe injuries. In most of these cases disability results, preventing participation (or active participation, at best) in labour force. The disabled individual is no longer in a position to adequately provide for himself and/or his dependents financially. And the worst case scenario is that the one-time remunerative worker or person whose earnings support his family is now absolutely dependent on others for means of livelihood due to disability. Worse still, the sustenance of the family members is in limbo. The positive correlation between disability and poverty is not in doubt. Poverty creates challenges for families that may be particularly difficult to manage with only one available disabled parent. These road accidents and the resultant deaths and/or disabilities may lead to changes in family structure such as loss of one or both parents, divorce or separation due to disability. This condition not only places individuals at greater risk of poverty but also may increase their vulnerability to the challenges associated with poverty. Thus preventing road accidents and disability is preventing poverty. What South Africa (and indeed all African countries) needs is poverty reduction and not poverty acceleration (Wilson et al., 2001). The causes of road accidents usually pertain to road, vehicle, and human factors. Given that road users are supposed to adjust their behaviour to the road conditions, yet it is important to observe that improved road safety standards often reduce the risk of road accidents. In this respect, road construction and maintenance should be a top government priority. The government should improve the mechanism for ensuring the roadworthiness of motor vehicles, with particular reference to the maintenance of brakes, steering and tyres, as well as control of maximum speed and protection of passengers in case of an accident. In fact, in an empirical analysis of minibus-taxi road accident cases, the Council for Scientific and Industrial Research (1995) concluded, among other things, that speed, overloading and defective tyres represented the significant elements in collisions, both as individual contributory factors and in combination. The need for developing and improving measures aimed at reducing accidents cannot be overemphasized. It is thus recommended that a South African Road Safety Initiative should be put in place by the South Africa’s autonomous main roads agency. The objective will be to improve the road safety situation in the country by increasing awareness among the decision-makers, politicians, and the public, as well as developing better information systems and increased action by international organizations. In particular, modern sophisticated equipment should be used to vigorously enforce speed limits, as well as drinking and driving restrictions. Also mandatory installation and use of seat belts is important as the number of vehicles increases. This is because seat belts have been effective in protecting drivers and passengers against death and serious injuries (Jacobs and Baguley, 1995). It is clear that human factors are often the most important accident cause. Driving too fast, driving under the influence of drugs or alcohol, other reckless driving, inattention to other road users, overloading vehicles with goods and people, and driving for too many hours undoubtedly contribute significantly to road accidents. All these issues should be effectively addressed with the unparalleled co-operation and strong support of the people. Critical to the reduction of transport accidents in South Africa is increased political commitment. This is because if the political concern is low, funding for road safety measures will likely be low and unorganized, and implementation will be erratic. The result will be that accidents will continue to increase as road traffic increases, and the politicians will continue to blame the road accidents on irresponsible road-user behaviour alone. It is recognized that the government has made some consistent efforts to address the safety problems in the areas of education and awareness. Unfortunately, progress has been curtailed by a highly fragmented enforcement system. About 485 separate governmental entities hold some responsibility for enforcement on the roads, but use different standards for fines, speed limits, or heavy vehicle checking (Department of Transport, 2001). This patchwork system creates an overall misalignment of risk and does not augur well for effective monitoring and enforcement of road safety measures. Available information points to a dramatic rise in violent crime in South Africa. There are at least eight armed thefts of cars in each day in Johannesburg, while armed robbery and car hijackings are increasing in Pretoria (Telegraph, 2001). Also, the country’s murder rate is about 1,000 times higher than the world average, and has the worst record of rape in the world (Nevin, 1998). Against this dismal background, the government should do more to curb crime and violent behaviour. In particular, the police service should employ and improve on its crime intelligence network. In South Africa, as in many other countries, suicide is one of the leading causes of death. In fact, suicidal behaviour constitutes a major public and mental health problem, as well as a considerable drain on resources in both primary and secondary health care settings (Gulbinat, 1996; Leenaars, 1995). Granted that there are a plethora of reasons why people end their lives and sometimes those of other members of their family, however, paramount among these is poverty (May, 1998). The inability to provide for the family because one cannot get a job is a monumental problem. The latest available census figures shows that while unemployment rate is 33.8 % for the whole country, the African population which constitute about 76.7 % of the entire population, has the highest unemployment rate of 42.5 % (Statistics South Africa, 1998). As people become increasingly powerless economically, they continuously lose their means of survival and they tend to resort to suicide. The government should create more employment opportunities for its citizens. Additionally it should expand welfare benefits to cover not only all women aged 60 or more and men aged 65 or more who are entitled to a social pension of about $100 per month (May, 1998; Ministry for Welfare, 1997; Kinsella and Ferreira, 1997), but all economically active unemployed persons. One other emerging reason that is rapidly gaining currency behind the escalating suicide rate in South Africa is the prevalence of the human immunodeficiency virus (HIV), the virus that causes the acquired immune deficiency syndrome (AIDS). With the prevalence rate of 19.9 %, South Africa is one of the African countries with the highest HIV/AIDS prevalence rates (United Nations, 2001b; World Health Organization, 2001; UNAIDS, 2000). Many people cannot take the fact that they are HIV-positive, as a result they prefer to kill themselves (Mail & Guardian, 2001). There is the urgent need for the development of more relevant information, education and communication (IEC) programmes to build knowledge, motivation and skills. The IEC programmes need to be developed based on a full understanding of the individual and the broader socio-economic factors that influence individual, institutional and group behaviour. They should focus on fostering health and responsible behaviour. IEC could also be used to promote ideas of equitable and mutually respectful and responsible gender relations, to increase male responsibility in pregnancy and the prevention of STDs and HIV, and to promote informed reproductive health choices, especially for young women. This is because biological and social factors make women and girls more vulnerable to HIV/AIDS than men and boys. Moreover, there is empirical evidence to support the fact that HIV infection rates in young women can be 3-5 times higher than among young men (World Health Organization, 1994). As stated from the outset, it is impossible to completely eliminate external causes from the mortality experience of the South African society. But it is unarguably true that external causes can be substantially reduced. It is the contention of this paper that both the people and government of South Africa should work in tandem to bring this about, in order to eventually raise the expectation of life of the citizens. REFERENCES
The following images related to this document are available:Photo images[ep04040f3.jpg] [ep04040f2.jpg] [ep04040t1.jpg] [ep04040f1.jpg] [ep04040t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}