 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 19, No. 2, Sup. B, 2004, pp.179-198 Maternal and Child Health among the Urban Poor in Nairobi, Kenya Monica Magadi Centre for Research in Social
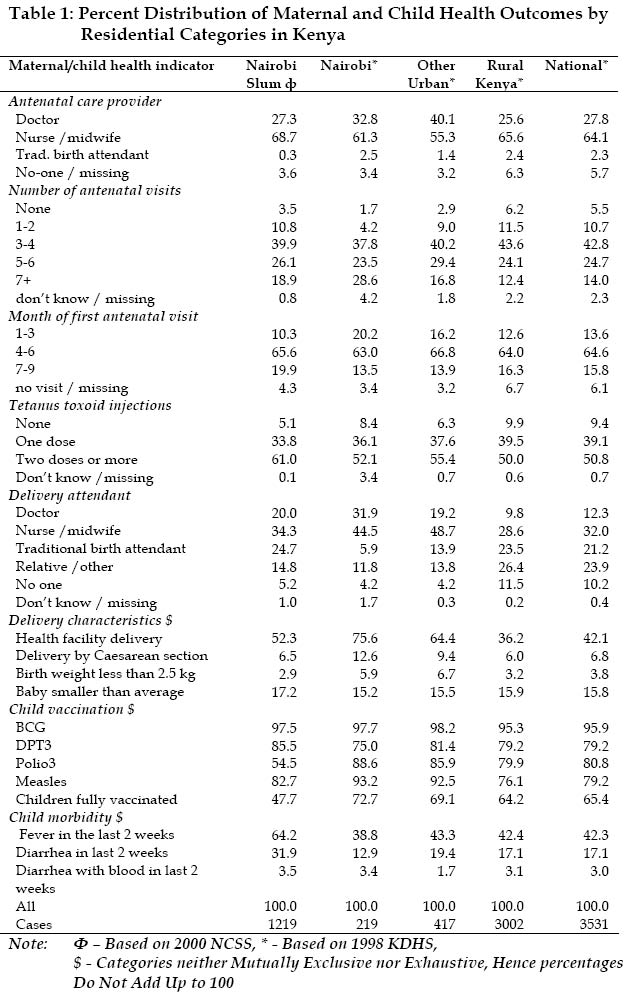
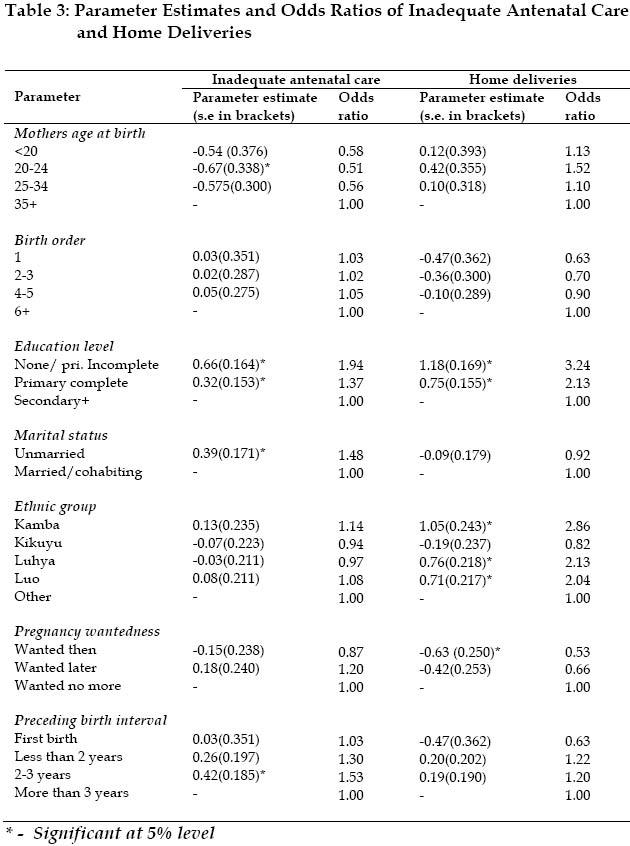
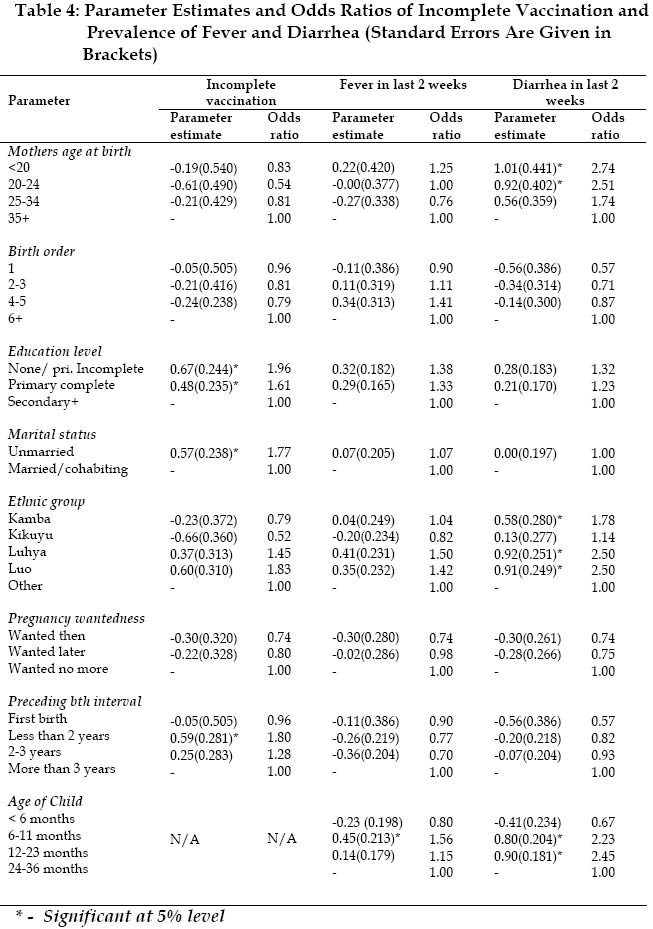
Policy (CRSP), Department of Social Sciences, LoughboroughUniversity ABSTRACT This paper examines maternal and child health in the Nairobi slums using information on 1219 births which occurred in the past three years before the Nairobi Cross-sectional Slum Survey (NCSS) of 2000. The specific objectives are to compare maternal and child health indicators in the Nairobi slums with the rest of the Kenyan population, and to identify socio-economic and demographic factors associated with poor maternal and child health in the Nairobi slums. The results show that overall, the quality of antenatal care in the slums is comparable to the rest of the Kenyan population. With respect to professional delivery care, the Nairobi slums are worse off than the rest of Nairobi or other urban areas in Kenya, but seem better off compared to the rural communities. It is with respect to child health indicators that the slum residents in Nairobi show the greatest disadvantage, in comparison with the rest of the Kenyan population. Children in the slums are considerably less likely to be fully immunized and more likely to experience fever and diarrhea than their counterparts living elsewhere in Kenya. In general, lower educational attainment and belonging to the Luo ethnic group are consistently associated with poorer maternal and child health outcomes in the Nairobi slums. INTRODUCTION Indicators of Maternal and Child Health with Particular Reference to Kenya Maternal health care, birth outcomes, child vaccination and morbidity conditions are all important indicators of maternal and child health. Poor antenatal care is a risk factor for adverse pregnancy outcomes for both the mother and the baby, including maternal mortality, perinatal mortality, premature delivery, low birth weight, pre-eclampsia and anemia, in many settings of the developing world. Apart from mere attendance of antenatal care, the quality of care received (in terms of the timing and frequency of visits and the content of antenatal care), does play a key role. Antenatal care is important for the identification and management of maternal complications, as well as for providing essential services such as tetanus immunization, iron and/or vitamin supplementation, and nutrition education. The frequency and timing of antenatal care are both important for timely identification and mitigation of potential pregnancy complications. It is important that antenatal care visits are started early in pregnancy and continue at regular intervals throughout the pregnancy. Some pregnancy complications, if not identified and treated early in pregnancy, would be detrimental to the health of the mother and the baby. It is generally recommended that antenatal care visits be made monthly during the first seven months, fortnightly during the 8th month, and then weekly until birth. Assuming the first visit is made during the 3rd month, this schedule translates to a total of 12-13 visits during pregnancy (NCPD, CBS and MI, 1999). Apart from frequency and timing of antenatal care, the quality and content of antenatal care are just as important. Tetanus vaccination is an important component of antenatal care to protect the baby against neonatal tetanus, which is one of the main causes of infant mortality. Two doses of the toxoid is usually given during a pregnancy, but sometimes only one dose or none may be required, depending on the number of doses already received during previous pregnancies. A total of five doses is considered adequate for lifetime protection (NCPD, CBS & MI, 1999). Appropriate care during delivery is important for the health of the mother and the newborn, especially in cases where childbirth complications develop. Although the majority of deliveries have no complications, sometimes sudden and unpredictable complications may arise, requiring urgent medical attention. It is estimated that 40% of pregnancies world-wide develop complications, 15% as life-threatening emergencies (Graham and Murray, 1997). The birth outcomes under such circumstances are greatly improved if the complications occur in the presence of a qualified attendant and in a medical facility with necessary equipment and supplies to adequately manage the complications. The particular concern in the delivery care component of maternal health care in Kenya arises from a number of factors. First, despite almost universal professional antenatal care in Kenya, less than half of all deliveries in the country take place in a health facility (NCPD, CBS & MI, 1999). Secondly, the KDHS data sets show that the significant improvement in antenatal care attendance over the years has not been matched with similar improvements in delivery care. The differences in utilization of antenatal and delivery services is probably a factor of accessibility of services, in combination with a range of cultural issues which influence acceptability of specific services. Service access, relating to affordability, is perhaps of greatest relevance to the slum communities. The introduction of cost-sharing for specific health services (excluding promotive and preventive services such as antenatal care) by the government of Kenya since 1989 is a clear deterrent for poor women seeking delivery care. Delivery characteristics such as Caesarean section deliveries and birth weight or birth size can provide useful indicators of maternal and child health. Birth weight or size is a strong predictor of infant mortality, with low birth weight being associated with a high risk of infant mortality, especially during the first few weeks of life. Low birth weight often results from premature delivery or intrauterine growth retardation or both. Caesarean section deliveries represent difficult deliveries that would result in a maternal and perinatal morbidity or mortality if appropriate care is not provided during childbirth. Caesarean section is normally viewed as an unfavorable delivery characteristic due to the increased risk of maternal death often due to sepsis, anesthetic accidents or technical problems during surgery. On the other hand, very low rates of Caesarean section deliveries may indicate lack of essential obstetric care since it is estimated that at least 5% of deliveries in a population would require a Caesarean section to avert morbidity or even death to the mother and the newborn (UNICEF/ WHO/ UNFPA, 1997). Important indicators of child health include child vaccination and morbidity conditions. The key strategy for controlling vaccine preventable diseases among children in Kenya is carried out through the Kenya Expanded Program on Immunization (KEPI). The program aims to reduce morbidity and mortality caused by measles, polio, tuberculosis, tetanus, diphtheria, and pertussis. According to the WHO guidelines, children should be fully immunized before they attain age 12 months. The complete immunization schedule consists of one dose of BCG (to protect against tuberculosis), usually given at birth, or first clinic visit; three doses of polio and DPT (to protect against diphtheria, tetanus and pertussis) given at approximately 6, 10 and 14 weeks of age; and one dose of measles given soon after 9 months of age. Finally, cough, fever and diarrhea are among the most common symptoms for the major killer diseases among children in Kenya. A serious cough may be a symptom of ARI while malaria and other common infections among children are usually accompanied by fever. Study Rationale and Objectives The underlying causes of maternal and child deaths in Kenya are factors that can be addressed with significant results for overall health of women and children. Maternal and child deaths are the direct result of disease and malnutrition, which in turn result from inadequate access to food, shelter, health care, safe water, sanitation and education (UNICEF, 1992). The access to these basic services is largely determined by the availability and distribution of resources. The immediate causes of maternal deaths include hemorrhage, sepsis, ruptured uterus and anemia, which frequently result from factors such as unsafe abortions, nutritional deficiency disorders, poor health or nutritional status, and inadequate care before, during or after delivery. In particular, sepsis, hemorrhage and ruptured uterus are often a result of poor care during and after delivery. Although low socio-economic status has been linked to poor pregnancy outcomes for the mother, it is likely that the influence is through lack of appropriate maternal health care and poor nutritional status (Magadi et al., 2004). These same factors (i.e. nutritional deficiencies and poor quality of care during delivery) have been linked to high rates of infant deaths during or slightly after birth. Over the years, the major causes of child deaths in Kenya, as in other African countries, have included malaria, acute respiratory infections, diarrhea disease, and several vaccine preventable diseases such as measles, polio, tuberculosis and neonatal tetanus (UNICEF, 1992). An examination of causes of under-five deaths (based on verbal autopsies) in different locations in Kenya identified pneumonia as a key factor in a rural community (Milza, et al., 1986), while diarrhea and measles have been identified as the predominant causes of under-five mortality in Kibera (NCB/CSD, 1992), which is the biggest slum in Nairobi Measles deaths are often localized to areas with low immunization coverage and high population density, while diarrhea results mainly from using unsafe water, poor personal hygiene, and unsanitary waste disposal. These conditions are typical of slum communities, making children in these areas highly susceptible to these diseases. More recently, the HIV epidemic, rising poverty levels and general deterioration in health care systems have all contributed to worsening child health conditions, resulting in an upsurge of infant and child mortality in many parts of sub-Saharan Africa. In Kenya, both infant mortality and under-five mortality increased by 30% between 1989 and 2003 (CBS, et al., 2003). The urban poor have been among the hardest hit, recording higher child mortality than their counterparts living elsewhere in the country (APHRC, 2002). This paper examines maternal and child health using information on births occurring in the past three years before the Nairobi Cross-sectional Slum Survey (NCSS). The specific objectives include (i) to compare maternal and child health outcomes in the Nairobi slums with the rest of the Kenyan population; and (ii) to determine socio-economic and demographic factors associated with poor maternal and child health outcomes in Nairobi slums. DATA AND METHODS The data analyzed in this paper is from the Nairobi Cross-sectional Slums Survey (NCSS) conducted by the African Population and Health Research Center (APHRC) based in Nairobi. The survey covered a representative sample of all the slum settlements in Nairobi and successfully interviewed a total of 3256 women aged 12-49 years from 4564 Nairobi slum households. Information on maternal health care and delivery characteristics analyzed in this paper relates to 1219 last births reported by the women interviewed, while information on child immunization and prevalence of common diseases among children was obtained for 1182 children born during the past three years before the survey. Specific outcomes of interest include antenatal care (type of provider, frequency of visits, timing of first visit and tetanus toxoid vaccination), delivery care (place of delivery and delivery attendant), delivery characteristics (Caesarean section, birth weight and size of baby at birth), child vaccination and recent child morbidity (prevalence of cough fever and diarrhea). The analysis is carried out in two stages. The first involves a comparison of maternal and child health indicators in the Nairobi slums with those of the other residential categories of the Kenya population: Nairobi, other urban Kenya, rural Kenya and overall national figures for Kenya. The comparison data is from the 1998 Kenya Demographic and Health Survey. The second stage involves a bivariate and multivariate analysis of demographic and socio-economic factors associated with poor maternal and child health outcomes in the slums of Nairobi. The outcomes included in this part of the analysis, namely: adequacy of antenatal care, place of delivery, vaccination coverage, and experience of fever and diarrhea were all dichotomized. Inadequate antenatal care is defined as less than four antenatal care visits during pregnancy, with then first visit taking place late, during the last trimester. The factors included in the analysis were maternal age at birth of child, birth order of child, maternal educational attainment, marital status, ethnicity, desirability of index pregnancy, and preceding birth interval. The bivariate analyses included Chi-square tests to assess significant differences in proportions experiencing outcomes by various socio-economic and demographic sub-groups. The multivariate analyses are all based on logistic regression to establish differences in odds of experiencing the outcomes of interest between various subgroups, when the other important factors are controlled for. For the multivariate analysis of child morbidity (incidence of fever and diarrhea), other important factors known to influence morbidity, namely age and sex of child, are included as covariates so that their effects are controlled for. RESULTS Comparison of Maternal and Child Health in Nairobi Slums with other Kenyan Population The distribution of maternal and child health outcomes by various residential categories in Kenya are presented in Table 1. The first important question on the quality of antenatal care relates to who provides antenatal care, in order to determine the extent of professional antenatal care. Overall, nurses or trained midwives are the predominant antenatal care providers in the Nairobi slums, accounting for about 69% of the cases, while doctors provide antenatal care in about 28% of the cases. It is, however, important to note that respondents may not be able to precisely distinguish between nurses or midwives and doctors, since sometimes male midwives or nurses are often mistaken for doctors by the general public. It is clear from the distributions that very rarely do traditional birth attendants provide antenatal care in this urban setting. The pattern of antenatal care provider in the slums is consistent with antenatal care in the rest of Kenya, although the slums seem to have the lowest proportion of TBA care, and the highest nurses/midwife care compared to the other communities in Kenya. Less than half of the births in the slums received more than four antenatal care visits during pregnancy. The median number of antenatal care visits of 3.9 is far lower than the recommended, but comparable to the national median of 3.7 visits. On average, the frequency of antenatal care visits in the slums of Nairobi is comparable to the other communities in Kenya, though notably worse off compared to Nairobi as a whole. For the majority of births in the Nairobi slums (66%), antenatal care starts during the second trimester and for another significant proportion (20%) it starts very late in pregnancy, during the last trimester. This pattern is consistent with the rest of the Kenyan population, though women in the slums tend to initiate antenatal care later. The median gestation period at first visit of 5.9 months is comparable to the national average of 5.7. In general, almost all women in the slums who had a birth in the three years preceding the survey had received at least one tetanus injection in the five years preceding the survey. Only 5% had not received any tetanus vaccination over the last five years. Tetanus vaccination coverage in the slums compares quite favorably with the rest of the Kenyan population. The proportion of births in the slums that take place in a health facility is higher than the proportion in rural areas or Kenya as a whole, but considerably lower than the proportion in Nairobi, or other urban areas in Kenya. While about half of the deliveries in the slums take place in a health facility, about three-quarters of all deliveries in Nairobi as a whole occur in a health facility. Births that are delivered in a health facility are likely to be attended to by a doctor, nurse or midwife while those delivered at home are likely to be attended to by a traditional birth attendant, a relative or other unskilled persons. Overall, 54% of births were delivered by a medical personnel (doctor, nurse or midwife), 25% by a traditional birth attendant (TBA), 15% by a relative or other unskilled persons, while 5% were delivered without any assistance. Medical delivery assistance is higher in the slums compared to the rural areas or Kenya as a whole, but substantially lower compared to Nairobi or other urban areas. Delivery assistance by a TBA is particularly high in the slums, compared to other urban settings. Only 6% of births in Nairobi as a whole are assisted by a TBA, yet one in four births in the slums is delivered by a TBA. Overall, the proportion of births delivered through Caesarean section in the slums (7%), is lower than that the in Nairobi (13%) or other urban areas (9%), but comparable to the rates in rural areas or Kenya as a whole. In general, the proportion of births reported to be smaller than average in the slums (17%) is comparable to the proportions reported in other settings in Kenya (15-16%). Information on child vaccination was obtained from child health cards, or mothers’ verbal report, if no child card was available. Overall, vaccination coverage for BCG, the three doses of DPT in the slums is comparable to coverage in the other settings in Kenya. However, coverage of the third polio vaccines is particularly low in the slums, compared to other settings. Measles vaccination in the slums is also lower than the coverage in Nairobi and other urban areas, but slightly higher than the rural areas or Kenya as a whole. Consequently, full immunization coverage in the slums compares rather unfavorably with the rest of Kenya. On prevalence of childhood diseases, the Nairobi slums seem to fare rather unfavourably compared to the rest of Kenya. Overall, 64% of children under three years of age were ill with fever in the two weeks period before the survey. This prevalence is considerably higher than the other settings in Kenya, all of which have prevalence rates below 44%. Nairobi is one of the regions in the country with relatively high prevalence of diarrhea. This has been explained mainly in terms of poor sanitation in the large and densely populated low-income areas. Slum areas are generally characterized by poor access to appropriate means of excreta disposal and lack of safe drinking water. A survey of basic facilities in Kenya revealed that more than half of the slum population in Nairobi have no access to appropriate means of excreta disposal. In addition, the survey observed that while 92% of urban residents in planned high density areas in Kenya have access to safe drinking water, only 53% of slum dwellers did (CBS/GOK, 1990). Data from three major slums in Nairobi (Kibera, Mathere and Kawangware) indicate that most slum dwellers do not have water supply to their houses, but purchase water from informal traders (more than 80% in Kibera and Mathare) or draw it from communal water points (AMREF, 1992). All these issues suggest that diarrhea is likely to be a major problem in the Nairobi slums. The results show that 32% of the children in the slums under three years of age had diarrhea in the two weeks period prior to the survey. This rate is more than double that of Nairobi as a whole (13%), and considerably higher than the rates for other urban areas, the rural areas, and Kenya as a whole. About 4% of the children in the slums had diarrhea with blood, which is a sign of serious systemic infection. Socio-economic and Demographic Factors Associated with Poor Maternal and Child Health in the Nairobi Slums This section of the paper examines the association between various socio-economic and demographic factors and maternal /child health in the slums of Nairobi. The analysis focuses on selected key maternal and child health outcomes, namely, timing and frequency of antenatal care, place of delivery, child vaccination, and prevalence of fever and diarrhea. Descriptive Analysis Table 2 presents the descriptive analysis, based on the percent distribution of these outcomes by given socio-economic and demographic characteristics. The distribution of adequate antenatal care in the Nairobi slums varies significantly according to most background characteristics (except ethnicity). The proportion receiving inadequate antenatal care rises steadily with increasing maternal age and parity. It is possible that greater anxiety about pregnancy among teenage mothers and first births would lead to adequate antenatal care (i.e. early start and more frequent visits). Older mothers (35 years and above) and births of order 6+ are the least likely to receive inadequate antenatal care. The pattern of antenatal care by marital status is not consistent with the observed pattern by age. Although single mothers are likely to be young, and young maternal age is associated with adequate antenatal care, single mothers are observed to have the lowest tendency of receiving adequate antenatal care, compared to ever married women. A plausible explanation for this is that births to single women are more likely to be unplanned, and antenatal care is likely to be inadequate due to mothers’ ambivalent attitudes towards such pregnancies (see, for example, Weller et al., 1987; Magadi et al, 2000). The distribution of antenatal care by pregnancy wantedness confirms that unintended pregnancies are associated with inadequate antenatal care in the Nairobi slums. The results also show some evidence of long preceding birth interval (3 years or more) being associated with more adequate antenatal care. As would be expected, higher educational attainment is consistently associated with more adequate antenatal care. While half of mothers with no formal education or incomplete primary education received inadequate antenatal care, less than one third of those with at least secondary education did so. The distribution of timing of antenatal care by division show least adequate antenatal care in Kasarani, Makadara and Kibera divisions, while Westlands Division has the most adequate antenatal care. More or less similar patterns are observed with respect to delivery care as antenatal care. There was considerable variation by division, with the highest proportion of health facility deliveries being reported in Westlands (74%), while the lowest proportion was in Embakasi division (41%). The Kikuyu have the highest proportion of health facility deliveries (70%), while the Kamba have the lowest (42%). With respect to education, women with secondary level education or higher have the highest proportion of health facility deliveries (70%), while those with no education or primary incomplete education had the lowest ((40%) as would be expected. The distribution of place of delivery by demographic characteristics show that births to women aged 35 years and above, and higher order births, are the least likely to be delivered in a health facility. The variation by birth order is particularly strong, showing a consistent negative relationship. About 60% of first order births are delivered in a health facility, compared to only 37% of births of order six and above. Unintended pregnancies and preceding birth interval less than 3 years are also associated with non-facility deliveries. Overall, about half (52%) of the children aged 12-23 months are fully vaccinated, and there is little variation in proportion of children fully vaccinated by most demographic factors such as mother’s age, marital status birth order and preceding birth interval all of which show no evidence of significant associations at 5% level. However, unintended pregnancies are significantly associated with lower vaccination coverage. Most of the socio-economic factors show significant associations. As would be expected, the proportion of children fully vaccinated rises steadily with increasing educational attainment. Also, Westlands Division and Kikuyu ethnicity are associated with relatively higher immunization coverage. With respect to child morbidity, a fairly large proportion (66%) of the children were ill with a fever in the two weeks’ period before the survey. Again there is little variation in fever morbidity by demographic factors, including maternal age, marital status, birth order and preceding birth interval. The most important demographic factor is child’s age (not shown in Table). Fever was most prevalent (75%) among the 6-11 month olds, and least prevalent among the older children aged less 2-3 years. The prevalence of fever by educational attainment indicate that maternal education has a protective effect on child illness. About 60% of children of women with at least secondary level education were ill with fever in the two weeks’ prior to the survey, compared to 70% of children to women with none or incomplete primary education. The prevalence of fever is highest among the Luo (70%) and Luhya (72%) ethnic groups and lowest among the Kikuyu (58%). Consistent with fever morbidity, diarrhea morbidity shows little variation with demographic factors, other than child’s age. Diarrhea is most prevalent among the 12-23 month old children (42%), as well as the older infants aged 6-11 months (40%), and least prevalent among the younger infants aged less than 6 months (17%), which is not surprising since most children at this age are exclusively breastfed. The prevalence of diarrhea appears to vary considerably by division, although the small number of cases in some of the divisions such as Pumwani and Makadara may be responsible for the observed variations. As would be expected, education seems to play an important role in the prevention of diarrhea diseases. About 25% of children to women with at least secondary level education had diarrhea, compared to 38% and for children of women with no more than incomplete primary education. Again, the highest prevalence of diarrhea was reported among the Luo (42%) and Luhya (40%) children. Multivariate Analysis of Factors Associated with Maternal Health Care Table 3 gives logistic regression results of factors associated with inadequate antenatal care (fewer than 4 visits during pregnancy or late start, after 6th month) and home delivery. The effects of maternal age, educational attainment, marital status and preceding birth interval on antenatal care persist after the effect of other important factors are controlled for. However, some of the factors showing significant associations in the bivariate analysis are not significant in the multivariate analysis, suggesting that the observed associations were presumably a manifestation of other important factors associated with these variables. For instance, the high risk of inadequate antenatal care observed among high order births in the bivariate analysis is likely to be due to the fact that such births are more common among older women who are more likely to have inadequate antenatal care. The multivariate analysis confirms that maternal age 20-24, at least secondary level education, being ever married, and preceding birth interval of at least 3 years are all associated with more adequate antenatal care. Mothers aged at least 35 years and those with no more than incomplete primary level of education have about double the odds of inadequate antenatal care compared to those aged 20-24 years and with at least secondary level education, respectively. Single women or births where the preceding birth interval is 2-3 years have odds of inadequate antenatal care about 1.5 times those of their counterparts who have ever married or where preceding birth interval is less than 3 years, respectively. The results for delivery care confirm the important role of educational attainment on maternal health care. Women with no more than incomplete primary education level have more than triple the odds of non-facility delivery, compared to those with at least secondary level education. Anther important result relates to the effect of desirability of a pregnancy on maternal health care. Desired pregnancies have about half the odds of being delivered outside a health facility as unwanted pregnancies. Net of other important factors in delivery care, including educational attainment, the Kikuyu women are significantly less likely to have non-facility deliveries compared to their counterparts belonging to the other ethnic groups. Multivariate Analysis of Factors Associated with Child Health in Nairobi Slums The results of the logistic regression analysis for child health indicators are presented in Table 4. In addition to the covariates considered in the analysis of maternal health care, additional variables relating to age and sex of child are included since these are have been observed to be associated with child morbidity in studies elsewhere (Magadi, 1997; Woldemicael, 2001). However, the analysis showed neither evidence for sex preference with respect to child vaccination, nor significant gender differences in child morbidity. Hence, sex of child was excluded in the final models. Maternal educational attainment again emerges as an important determinant of child health with respect to vaccination coverage. Children of women with at least secondary level education have about double the odds of being fully vaccinated compared to those whose mothers had no more than incomplete primary education level. Other important factors in child vaccination coverage include marital status and preceding birth interval. Children born after a short preceding birth interval of less than 2 years, or born to single mothers, have higher odds of incomplete vaccination compared to those of ever married women or long preceding birth interval of more than 3 years by a factor of 1.8. With respect to child morbidity, the child’s age emerges as the most significant factor. The odds of having fever is highest among children aged 6-11 months, followed by those aged 12-23 months, and lowest for infant aged less than 6 months. When age of child is controlled for, none of the other factors show significant associations with fever morbidity. Although the patterns of educational attainment by child morbidity indicators are in the expected direction, the effects are not statistically significant. For diarrhea morbidity, mother’s age and ethnicity have significant effects, in addition to age of child. Again, 6-11 and 12-23 months of age are associated with the highest risk of diarrhea, while less than 6 months of age is associated with the lowest risk. The risk of diarrhea morbidity steadily declines with maternal age, with children of adolescent mothers (aged 15-19 or 20-24) having odds of diarrhea at least 2.5 times higher than for mothers aged 35 years or over. Considerably higher risk of diarrhea morbidity is also observed among the Luo and Luhya ethnic groups. DISCUSSIONS AND CONCLUSIONS The results of this study are to a large extent consistent with findings elsewhere both with respect to the effect of urban poverty on maternal and child health as well as the association between these outcomes and various socio-economic and demographic characteristics. In particular, the adverse health consequences of urban poverty for children has been well documented (Timaeus and Lush, 1995; Brockehoff and Brennan, 1998; APHRC, 2002; UNICEF, 2002). The observed pattern of delivery care by urban poor, urban non-poor and rural residence is typical of sub-Saharan Africa region (Magadi, et al., 2003). With respect to the effect of various socio-economic and demographic factors on maternal and child health, the observed patterns by educational attainment, maternal age, child’s age, preceding birth interval and desirability of pregnancy conform to findings previously observed in other settings showing increased vulnerability for low maternal educational attainment, too young or too old maternal age, children aged 6 -23 months, short birth intervals and unintended pregnancies (Curtis et al 1992; Habtemariam, 1994; Magadi, 1997; Griffiths et al., 2001). In general, the quality of antenatal care in the slums is comparable to the rest of the Kenyan population. The proportion of births/pregnancies receiving antenatal care from medical personnel, the median number of antenatal care visits during pregnancy, and the median timing of first visit in the slums is comparable to the other communities in Kenya. It is interesting to note that the lowest proportion of births that did not receive any tetanus injection during pregnancy, was reported in the Nairobi slums. Although the quality of antenatal care in the Nairobi slums seems fair, there is need for special attention on specific sub-groups of women, namely those with low educational attainment (none or incomplete primary), older mothers aged 35 year or above and single mothers. These sub-groups of women have the highest risk of not receiving adequate antenatal care. The number of antenatal care visits made is often far from adequate and the visits are also likely to be started late in pregnancy. Hence, special IEC messages on the importance of appropriate antenatal care should target these groups. With respect to professional delivery care, the Nairobi slums seem to be better off than the rural communities or Kenya as a whole, but worse off compared to Nairobi as a whole or other urban communities in Kenya. About half of deliveries in the slums take place in a health facility, compared to just over a third in rural areas, and about thee-quarters in Nairobi as a whole. Assistance during delivery follows a similar pattern, since deliveries in health facilities are usually attended to by medical personnel. It is, however, interesting to note that traditional birth attendant deliveries are most prevalent in the Nairobi slums. A quarter of births in the slums are assisted by TBAs, compared to only 6% of births in Nairobi as a whole. This suggests that probably all TBA assisted births in Nairobi are in the slums. Delivery care in the slums is particularly poor among women with low educational attainment, those belonging to the Kamba, Luyha or Luo ethnic groups, or in cases of unwanted pregnancy. In consistence with the pattern of health facility deliveries, the proportion of births delivered through Caesarean section in the Nairobi slums is higher than the rural areas or Kenya as a whole, but lower than in Nairobi or other urban areas. The proportion of children reported to be small at birth is only marginally higher in the slum than the other areas. The observed advantage in professional delivery care among the Nairobi slums residents compared to the rural residents is most likely a factor of physical accessibility of services. The issue of physical access to health services is a critical problem in many rural parts of Kenya, where long distance to hospitals and poor road conditions are actual obstacles to reaching health facilities and often a disincentive to even trying to seek care. On the other hand, the fact that Nairobi slum residents compare quite unfavorably with the residents of Nairobi as a whole or other urban areas in Kenya is most likely due to economic hardships faced by slum residents, which make existing maternity care services unaffordable to many slum residents. In addition, the issue of physical accessibility is also a factor here, not so much in relation to physical distance, but due to lack of proper roads within the slum settlements. It is with respect to child health indicators that the slum residents in Nairobi show the greatest disadvantage, in comparison with the rest of the Kenyan population. While at least 80% of children in the other areas received the third polio vaccine, only half of children aged 12-23 months in the slums did so. As a result of this, less that half of children in the slums were fully vaccinated, compared to between two-thirds and three-quarters of children in rural areas, other urban areas, or Nairobi as a whole. The prevalence of both fever and diarrhea are substantially higher among slum children than in all the other areas. An alarming proportion (about two-thirds) of children in the Nairobi slums had fever in the two weeks prior to the survey, compared to about 40% or less in all the other areas. Similarly, almost one in three children in the slums had diarrhea in the two weeks period, compared to less than one in five in the other areas. Child health is clearly a critical issue in the slums, as manifested by the low proportions of full immunization coverage and high prevalence of common childhood illnesses. The Nairobi slum children compare rather poorly with the rest of the Kenyan population, including the rural areas. The unsanitary conditions, poor drainage systems, lack of safe drinking water, overcrowding, and poor access to health services in the slums are possible contributing factors to poor child health. All of these deserve urgent attention. One interesting observation relating to maternal and child health among descents of specific ethnic communities is the close association with their rural counterparts. For example, the poor health outcomes observed among the Luo ethnic group, and the more favorable outcomes for the Kikuyu community may be linked to the poor outcomes and the more favorable outcomes that have been observed in Nyanza and Central provinces respectively, regions predominantly occupied by these two ethnic groups. This suggests that the poor health outcomes (e.g high infant and child mortality) consistently observed in NyanzaProvince, for instance, may be more of a factor of cultural practices, rather than availability and accessibility of health services. There is need for more in-depth studies in these communities to identify harmful cultural practices that may endanger child health. ACKNOWLEDGEMENT The data analyzed in this paper is from the Nairobi Cross-sectional Slums Survey (NCSS) conducted by the African Population and Health Research Centre (APHRC) in 2000, with financial support from the Rockefeller Foundation (Grant #RF 99009#199). The author was a Research Fellow at APHRC at the time of the survey. An earlier version of this paper presented at the Fourth African Population Conference in Tunis, December 2003. REFERENCES
Copyright 2004 - Union for African Population Studies The following images related to this document are available:Photo images[ep04041t3.jpg] [ep04041t1.jpg] [ep04041t4.jpg] [ep04041t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}