 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
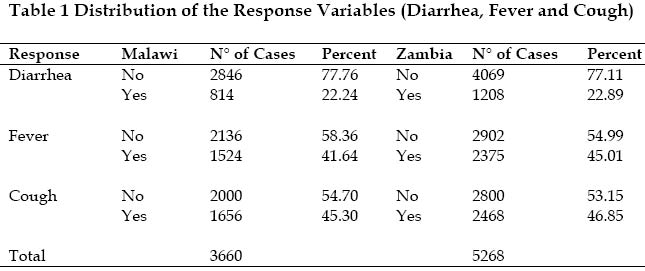
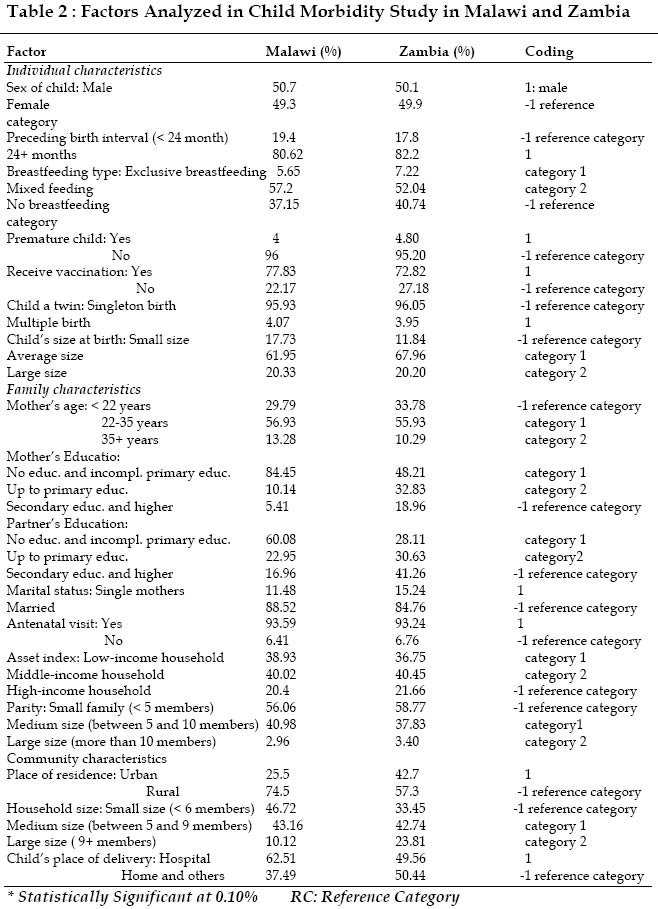
African Population Studies/Etude de la Population Africaine, Vol. 19, No. 2, Sup. B, 2004, pp.199-226 The Spatial Epidemiology of Childhood Diseases in Malawi and Zambia Kandala Ngianga-Bakwin and Nyovani Madise Southampton Statistical Sciences Research Institute, Division of Social Statistics, University of Southampton Highfield, SO17 1BJUK Code Number: ep04042ABSTRACT This paper applies a Bayesian geo-additive generalized linear model to describe the spatial variation, at the district level, on the prevalence of diarrhea, fever and cough among children under 5 years of age using the 1992 Demographic and Health surveys (DHS) from Malawi and Zambia. The modelling technique employed here may be applicable to other research questions in the DHS data sets. The range of observed childhood diarrhea, fever and cough were dichotomized into high or low districts in Malawi and Zambia. We mapped the residual districts spatial effects of these three ailments and explored the clustering of high or low diarrhea, fever and cough rates districts across space after controlling for all other confounding factors. We find visual evidence that high or low morbidity districts spatially cluster together within each country. This evidence suggests that relatively high or low childhood morbidity persist within a spatial region and population, suggesting that research efforts may be focused on these clusters to assess local causes (environmental, cultural etc...) of high or low childhood morbidity. INTRODUCTION The major diseases of children in Malawi and Zambia are malaria, diarrhea, respiratory diseases, particularly pneumonia, and AIDS (UNICEF, 2000). These ailments are still a major cause of mortality among children in many developing countries, particularly in Sub-Saharan Africa. Yet, except for some descriptive reports by National Statistics offices of these countries, few systematic studies of factors that influence the prevalence of malaria, cough and diarrhea among young children in these countries were carried out. The success of any policy or health care intervention depends on a correct understanding of the socioeconomic, environmental and cultural factors that determine the occurrence of diseases and deaths. Until recently, any morbidity information available was derived from clinics and hospitals. Information on the incidence of diarrhea, malaria and pneumonia obtained from hospitals represents only a small proportion of all illnesses, because many cases do not seek medical attention (Black, 1984). Thus, the hospital records may not be appropriate for estimating the incidence of diseases for program developments (Woldemical, 2001). The mapping of variation in risk of child morbidity can help improve the targeting of scarce resources for public health interventions. Bearing in mind that direct mapping of relevant environmental risk factors (which may vary considerably in both space and time) is difficult and this has led to investigations of environmental proxies (Kandala et al., 2001). The use of DHS data in the understanding of childhood morbidity has expanded rapidly in recent years (Woldemical, 2001; Yoannes et al., 1992; Ryland, 1998; Walter, 2001). However, few attempts have been made to address explicitly the problems of spatial auto-correlation and nonlinear effects of metrical covariates in the interpretation of results. Woldemicael 2001 and Walter 2001 reported a regression analysis of the prevalence of diarrhea among children in Eritrea and Kenya, including child and mother level covariates but they failed to control for the spatial autocorrelation in the data. This neglect leads to underestimation of standard errors of the fixed effects that inflates the apparent significance of the estimates (Bolstad and Manda, 2001). This study shows how the geo-additive model framework (Fahrmeir and Lang, 2001) can be adapted to extend the analysis of Woldemicael (2001) and Walter (2001) to provide an explanation of the residual spatial variation in the data and in particular to assess whether the variation is spatially structured. If this is true, it implies that adjusted prevalence is similar among neighboring districts, and then the possible explanation must be partly environmental. If not, a more likely explanation is that the residual spatial variation is induced by variation in unmeasured districts-specific factors. The rationale is that a spatial effect is usually a surrogate of many unobserved influences, some of them may obey a strong spatial structure and others may be present only locally ((Fahrmeir and Lang, 2001). DATA AND METHODS The Demographic and Health survey (DHS) program of Malawi and Zambia conducted in 1992 was a first attempt to obtain population-based morbidity data. Individual data records were constructed for 3660 children in Malawi and 5268 children in Zambia. Each record consisted of morbidity information and a list of covariates. The DHS data only permit one to attribute child morbidity to specific causes for the last two weeks before the surveys. Table 1 shows the distribution of diarrhea, fever and cough morbidity during the last two weeks before the interview and Table 2 shows factors analyzed in this study (DHS, 1992). In this paper, we apply the geo-additive logistic model on the probability of a child having fever, cough and diarrhea during the reference period to determine the socio-economic, demographic variables that are associated with these three ailments while simultaneously controlling for spatial dependence in the data and possibly nonlinear effects of covariates. The model allows us to borrow strength from neighboring areas in order to obtain estimates for areas that may, on their own, have inadequate sample sizes. The analysis was carried out using BayesX-version 0.9 (Brezger et al., 2003), software for Bayesian inference based on Markov Chain Monte Carlo simulation techniques. The modelling framework is as follows (Kandala et al., 2001). Consider regression situations, where observations (yi; xi; wi); i = 1; … ; n, on a metrical response y, a vector x = (xi; … ; xp) of metrical covariates, times scales or spatial covariates and a vector w=(w1;… wr) of further covariates, in which categorical covariates, are often given. The generalized additive modelling framework (Hastie and Tibshirani, 1990) assumes that, given xi and wi, the distribution of the response yi belongs to an exponential family, with mean μi= ( yi| xi , wi ) linked to an additive semi-parametric predictor μi= h(), i = f1(xi1) + ... + fp(xip) + fspat(si) + w’i ; where h is a known response function, and f1,...,fp are nonlinear smooth effects of the metrical covariates and fspat is the effect of district si Î {1,...,S} where mother i lives. Models with a predictor that contains a spatial effect are also called geo-additive models (Kammann and Wand, 2003). In a further step we may split up the
spatial effect fspat into a spatially correlated (structured)
and an uncorrelated (unstructured) effect fspat(si) =
fstr(si) + funstr(si). The
rationale is that a spatial effect is usually a surrogate of many unobserved
influences, some of them may obey a strong spatial structure and others may be
present only locally. By estimating a structured and an unstructured effect we
aim to separate the two kinds of factors. As an added feature, we are able to
assess to some extent the amount of spatial dependency in the data by observing
which one of the two effects is larger. If the unstructured effect exceeds the
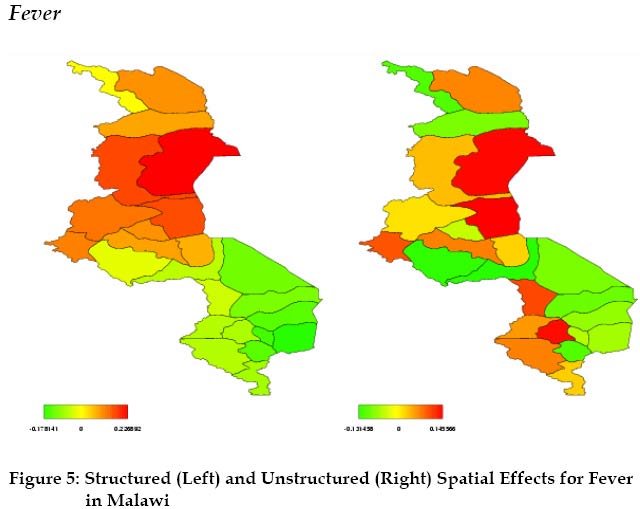
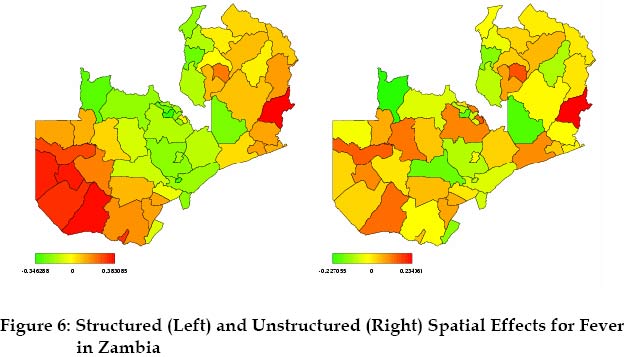
structured effect, the spatial dependency is smaller and vice versa. Such models are common in spatial epidemiology
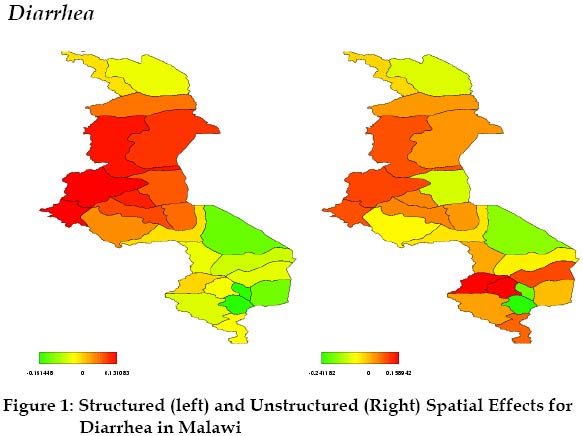
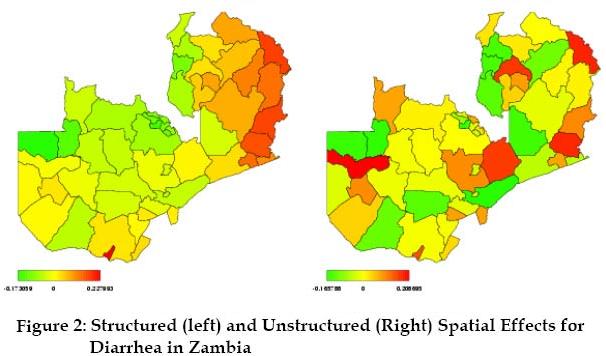
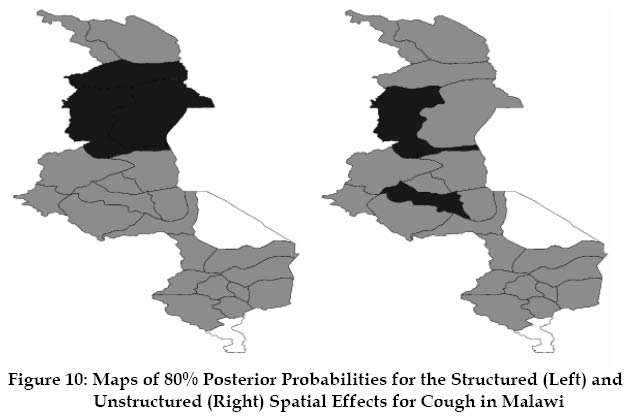
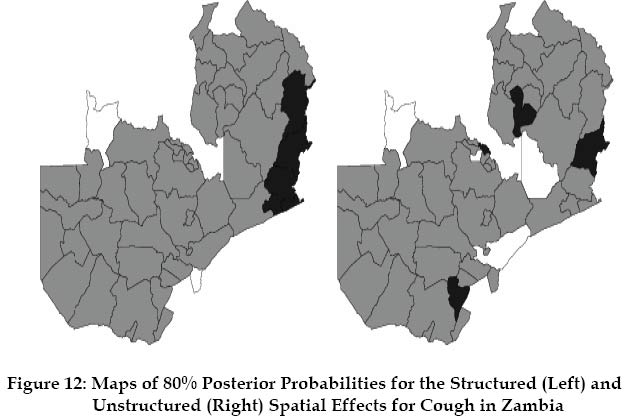
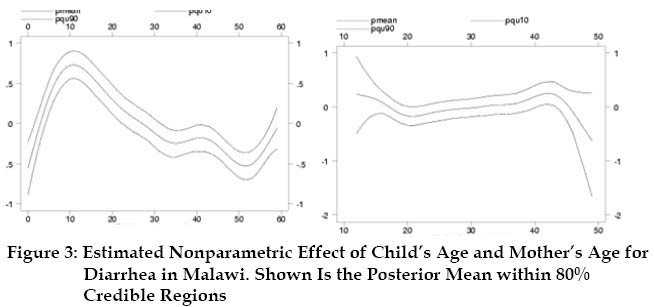
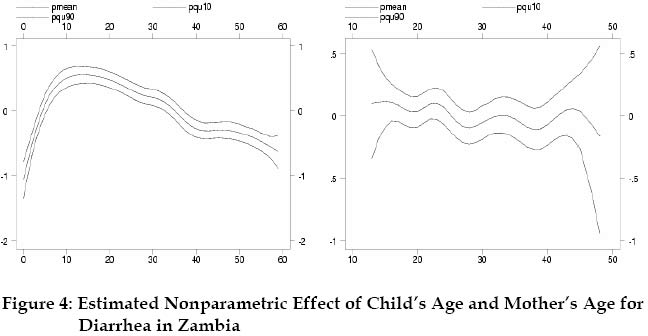
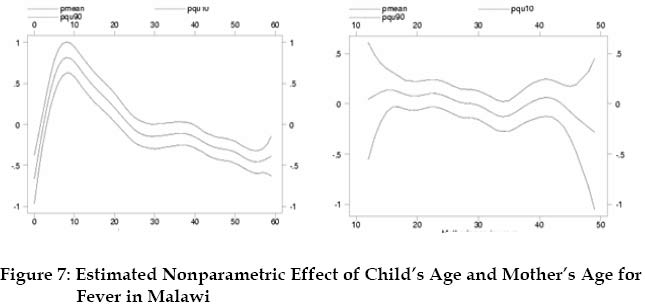
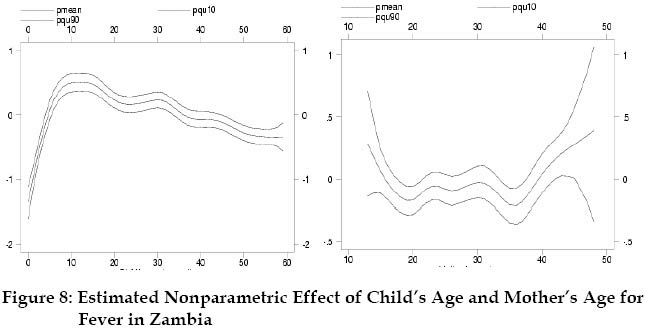
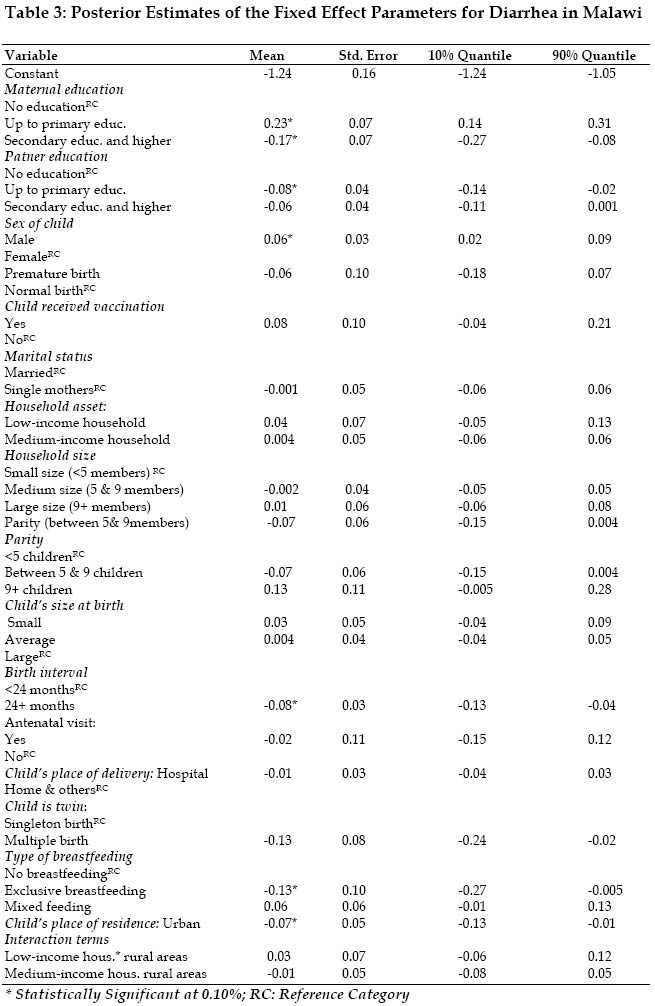
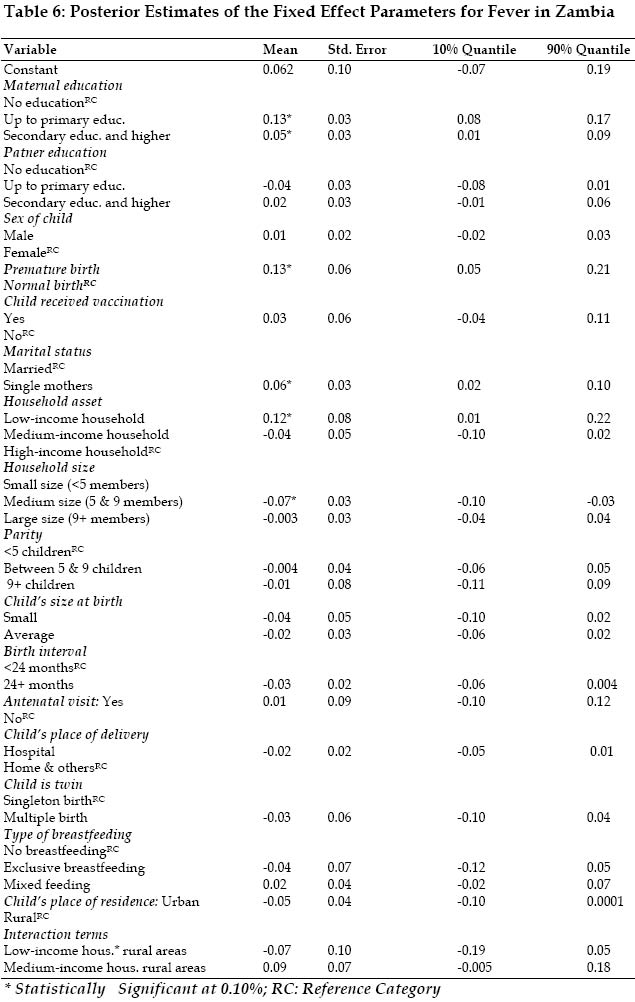
(Besag et al., 1991). The Deviance Information Criteria (DIC) (Spiegelhalter et al., 2002) was used for model fit and comparison. The non-linear effects in (1) of fi, f2, etc.. were modeled by cubic penalized splines (P-splines) with second order random walk penalty. For the spatial effect fstr(s) we experimented with different prior assumptions (two-dimensional P-splines or Gaussian random field (GRF) priors based on radial basis functions (Kammann and Wand, 2003). For both countries we estimated models where either a structured or an unstructured effect was included as well as a model where both effects were included. Based on these results, Markov random field (MRF) priors were used for fstr(s). We investigated the sensibility to the choice of different priors for the nonlinear effects (second random walk: RW2) and the choice of the hyper-parameter values a and b. We noticed that results for this application are not sensitive to the choice of the priors and hyper-parameter. RESULTS The presentation of the empirical results starts with residual spatial effects of the districts where the child lives. It continues with results of nonparametric effects of the mother’s age at child’s birth and child’s age. Finally results from various logistic regressions are presented that identify particular socioeconomic and environmental characteristics as significantly associated with childhood morbidity. The results are robust with respect to the prior specifications and emerge from a unified model framework that enables thorough investigation into the associations of childhood morbidity incidence and aerial-level risk factors, accounting for residual variation and spatial auto-correlation that likely arise from unmeasured confounders. When we attempted to fit the standard model with constant fixed effects for metrical covariates (child’s age and mother’s age at first birth of the child) and the spatial location (district in dummies), we found that there was not enough information in the data to estimate the parameters xit’correctly (confidence interval included zeros indicating no effects on the response variables). The posterior mean estimates for each model demonstrated that the district-level area factor did not adequately explain the short-range spatial structure. Various models were tried, but these made no difference. For both countries we then estimated models where either a structured or an unstructured effect was included as well as a model where both effects were included. Based on these results we found clear evidence for both countries of spatial correlation among neighboring districts. Hence, a spatially correlated effect fstr(si) was included into the predictors of our final models. We additionally include an unstructured effect funstr(si) because there is evidence of local extra variation in the highly urbanized areas of Zambia. We therefore considered including the spatial component funstr(si) + fstr(si) in addition to the nonlinear effects of mother’s and child’s age, thereby increasing model complexity. With standard regression models and multilevel models, it is assumed that the random components at the contextual level (district) are mutually independent. Even though, in practical, this assumption is not actually implied by these approaches, so correlated random residuals can also be specified (Langford and et al., 1999). The estimates of the presumed spatial correlated district level random effects in fact showed strong evidence of spatial dependence. This is indicated in Figures 1-2-5-6-9-11, which plots the posterior mean estimates of the spatial district effects. Though the spatial unstructured district effects for fever turns out to be insignificant, both maps show a strong spatial variation (results available from authors). Since prediction of spatial residual is our goals, the non-spatial model is clearly inadequate. We therefore focus on model (1), to give the results that were obtained during the fitting. Figures 1-2-5-6-9-11 map the estimates of the spatial effects (spatial residuals: the levels correspond to”high risk of morbidity (black colored)” and ”low risk (shades of grey colored)”)) with the significance maps (Figures 10 and 12), showing ”probabilities maps”. For a nominal level of 80% the levels correspond to ”high risk of morbidity (black colored)”, ”non-significant (grey colored)”, i.e. zero is within the credible interval around the estimate, and ”lower risk of morbidity (white colored)”. Figures 3-4-7-8-9-13-14 give the result of the non-linear effect of child’s age and the mother’s age. Shown are the posterior means together with 80 % credible intervals. Tables 3 through 8show the posterior mean and 90% credible interval for each of the fixed effects parameters for categorical covariates in model (1). There are sizeable fixed effects, which are highly significant (i.e. credible intervals are either strictly positive or strictly negative). The residual spatial effects (Figures 1-2-5-6-9-11) suggest district variation in the prevalence of diarrhea, cough, and fever in Malawi and Zambia. Diarrhea The data suggest considerable spatial auto-correlation in the underlying posterior means. The left panel of Figures 1 and 2 reveals high risk clusters mainly in the central districts of Malawi and in the northeast of Zambia. The result of non-linear effects of child’s age (Figures 3-4-7-8-9-13-14) suggests that there is continuous worsening of child morbidity up to about 6 months of age. This deterioration sets in right after birth and continues, more or less linearly, until 10 months and decreases thereafter. We find the influence of the mother’s age (right panel of Figure 3) on diarrhea morbidity to be in the form of an inverse U-shape in Malawi, while in Zambia (Figure 4) we have a U-shape. While the U or inverse U looks nearly symmetric, the descending portion exhibits a much larger range in the credible region. Children from younger (< 20 years) and older (35+ years) mothers are at higher risk of diarrhea morbidity compared to children from middle age group (20-35 years). The interpretation of results at the end of the observation (wide credible interval) is particularly unreliable in regions where there are few observations. With regard to the
fixed parameters, Table 3 shows that the prevalence of diarrhea in Malawi is
lower among infants who are exclusively breastfed, whose mothers are well
educated with a father having up to primary education, a long birth interval
(24+ months), a multiple birth and infants living in urban areas. Lower
parental education and male children are associated with higher risk of diarrhea.
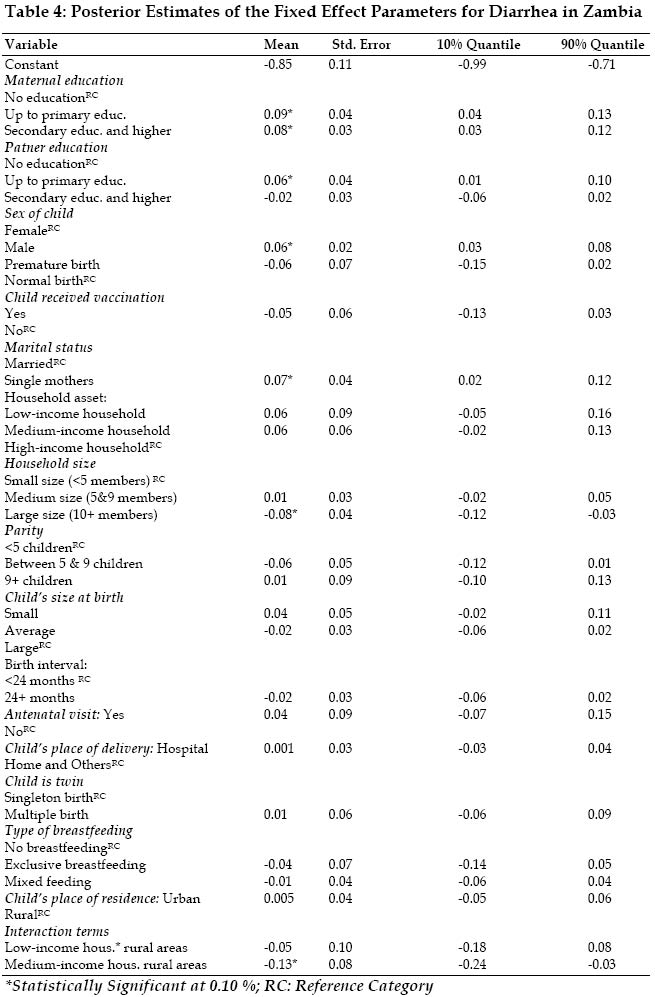
In Zambia (Table 4), higher
risk of diarrhea is associated with lower and higher parental education (up to
primary education for both parents and secondary education and higher for
maternal education), male children, and mother’s marital status (single mother).
Children from large size household are associated with lower risk of diarrhea.
In Zambia, children from medium
economic status households had lower risk of diarrhea morbidity if they lived
in rural areas. However, this analysis indicates that, in the two countries,
premature children, vaccination status, the antenatal visit during pregnancy,
child’s place of delivery (whether hospital or home), the economic status of
the household and child’s size at birth have little or no influence on diarrhea
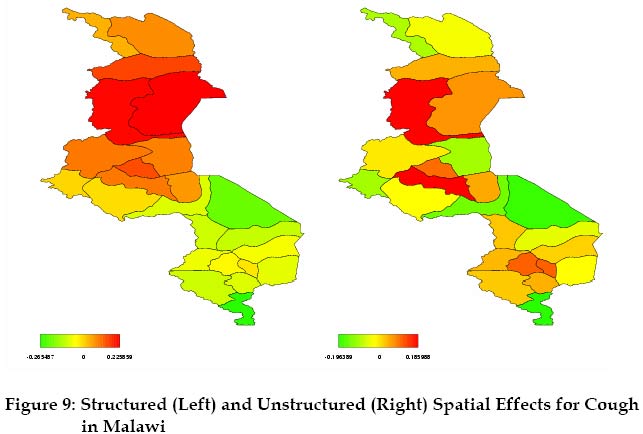
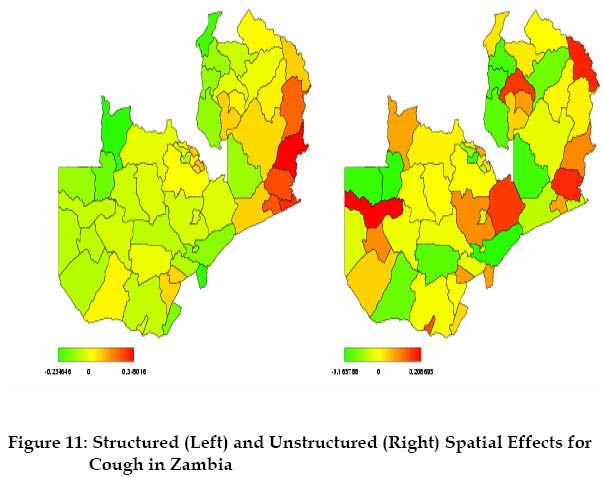
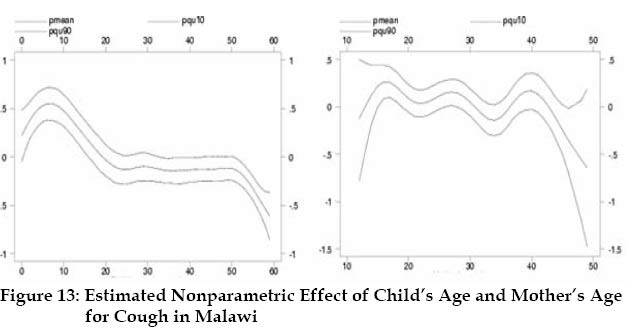
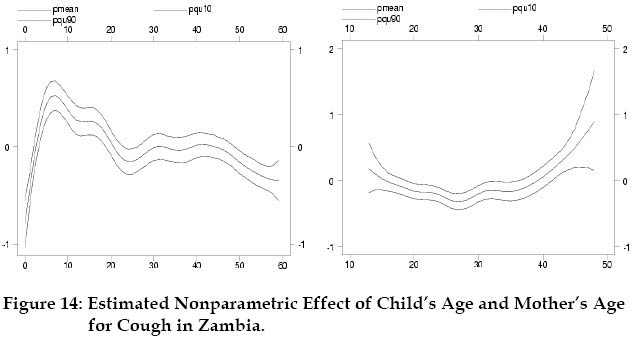
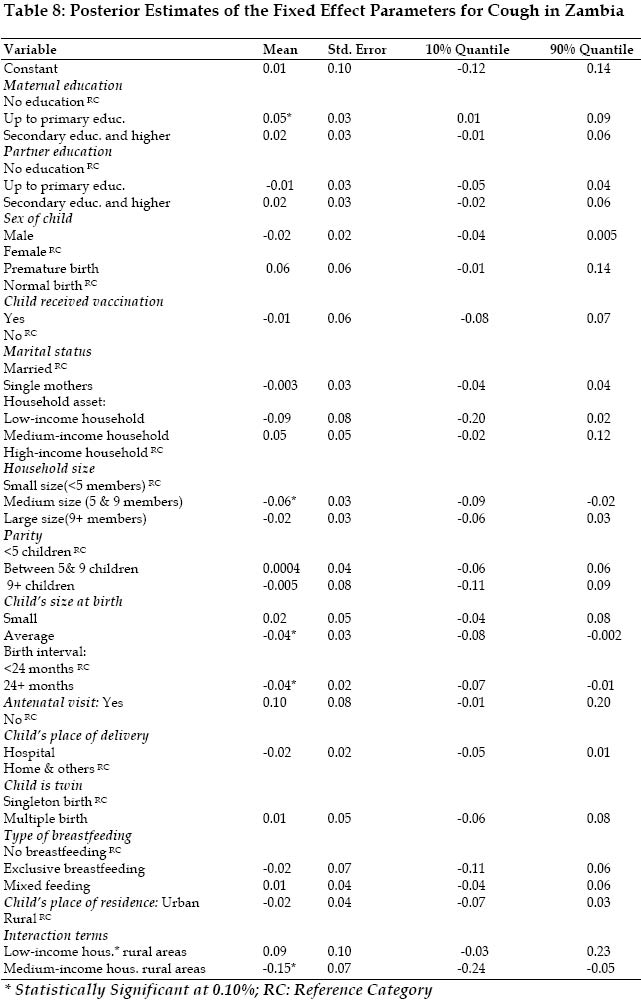
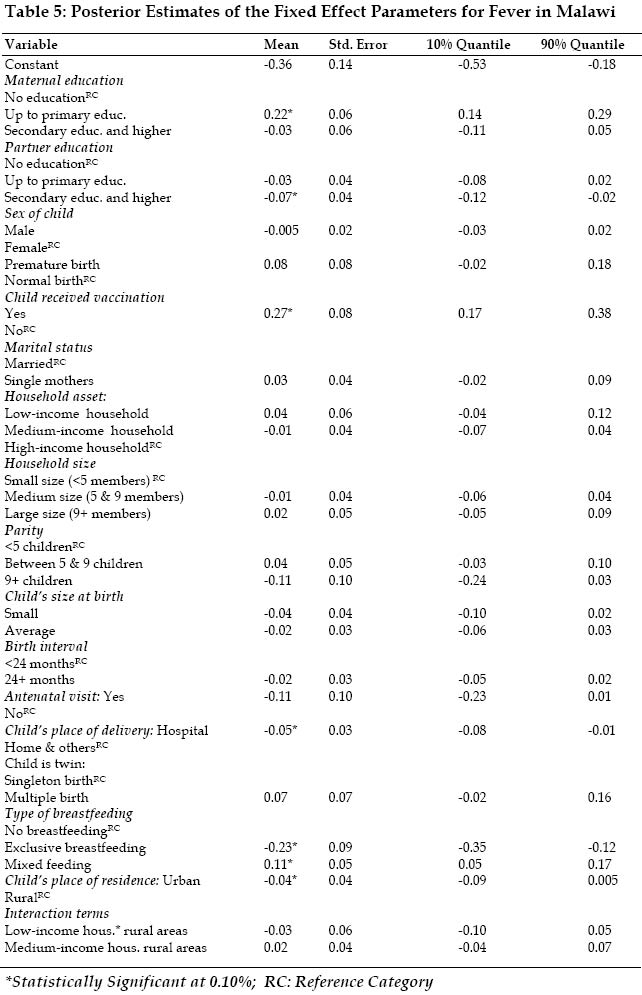
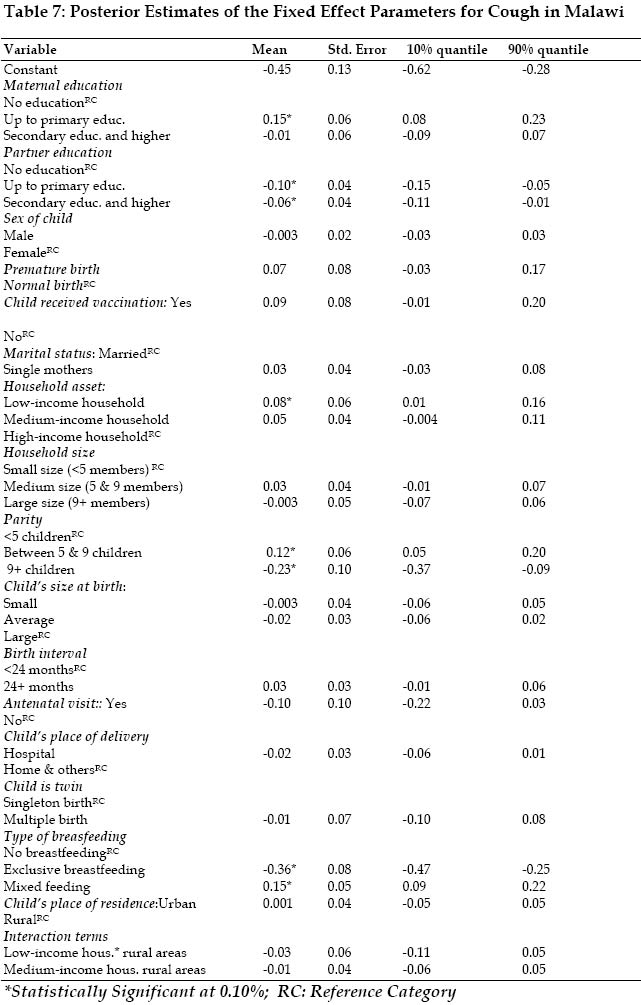
risk. Over and above the impact of the fixed effects, there appear to be negative influences on fever morbidity in the north that are spread and affect most of the districts there. The right panel of Figures 5 reveals also lower risk of fever morbidity in the capital Lilongwe in spite of being surrounded by some of the high risk districts. High risk clusters of fever morbidity in Zambia (Figure 6) are mainly located in the southern and north-east districts. The result of the non-linear effect of child’s age in the two countries (Figures 7 and 8) suggest that there is continuous worsening of the child morbidity up to about 10 months of age. The right panel of figures 7 and 8 associate the influence of mother’s age on fever morbidity to be in the form of an inverse U-shape in Malawi and a U-shape in Zambia. Children from younger (< 20 years) and older (35+ years) mothers are at higher risk of fever morbidity compared to children from middle age group (20-35 years). The fixed parameters show that the prevalence of fever in Malawi (Table 5) is higher among infants of low maternal education (up to primary education), vaccinated children and infants who are mixed feeding. Children born in hospital, breastfed exclusively and have a father with secondary education and higher are associated with lower risk of fever. In Zambia (Table 6), higher risk of fever morbidity is associated with lower and higher maternal education (up to primary education and secondary education and higher), premature birth, mother’s marital status (single mothers) and low economic status households. Children from medium size households are associated with lower risk of fever morbidity. However, this analysis indicates that, in the two countries, child’s sex, family size, child’s place of delivery, the antenatal visit during pregnancy, the type of breastfeeding, child’s size at birth, and child’s place of residence have little or no influence on fever risk. There is a strong north-south (left panel of Figures 9) gradient in the district spatial effects in Malawi with a fairly sharp dividing line that runs through the capital (Lilongwe) of the country. There appear to be negative influences on cough morbidity in the north that are spread and affect most of the districts there. The data suggest considerable spatial auto-correlation and local variation in the underlying posterior means for cough morbidity in Malawi and Zambia. The left panel of Figures 9 and 11 reveals high risk clusters mainly in the central and northern districts of Malawi and in the northeast of Zambia. This becomes even more obvious with Figures 10 and 12 showing the significance maps. The result of the non-linear effect of child’s age (Figures 13 and 14) suggest that there are continuous worsening of the cough morbidity up to about 6 months of age and a decrease thereafter. We find the influence of the mother’s age (right panel of Figures 13 and 14) on cough morbidity to be in the form of an inverse U shape in Malawi and a U shape in Zambia. Children from younger (< 20 years) and older (35+ years) mothers are at higher risk of diarrhea morbidity compared to children from middle age group (20-35 years). The fixed parameters (Table 7) show that the prevalence of cough in Malawi is higher among children from low economic status households, infants who are mixed feeding and infants with poor maternal education. Children who are breastfed breast milk exclusively, with higher parental education and a large family size are associated with lower risk of diarrhea. For Zambia (Table 8), higher risk of cough is associated with lower maternal education (up to primary education). Children from medium size household (between 5 and 10 members), have a long birth interval, were born with average size are associated with lower risk of cough in Zambia. In Zambia, children from medium economic status households had lower risk of cough if they lived in rural areas. However, analysis of these data sets indicates that, in the two countries, the variables child’s sex, vaccination status, child’s place of delivery, mother’s marital status and child’s place of residence have little or no influence on cough risk. DISCUSSION To gain an understanding of the geographic variation or patterns based on the observed morbidity prevalence, we began our analysis by first fitting the Bayesian hierarchical model without the inclusion of spatial (district) and nonlinear metrical (mother’s and child’s age) covariates. The Bayesian estimation of this model alone is impractical given the fact that we have to consider 31 dummies for the 32 districts in Malawi and 61 dummies for the 62 districts in Zambia, from which the reduction in variation in childhood morbidity can be readily assessed. We noted that the issues of particular interest in this study, and perhaps in health services research of similar kinds, are whether there is a significant geographic variation in childhood morbidity; if the answer is yes, can such variation be explained by potential risk factors? Spatial Residual Sub-Saharan Africa is geographically, demographically, socially, and culturally heterogeneous, and the extent and spread of child morbidity have accordingly been heterogeneous as well. This study has shown a sizeable district specific geographical variation in the level of child morbidity in Malawi and Zambia. Over and above the impact of the fixed effects in Malawi (Figure 1), there appear to be negative influences on child morbidity in the central districts affecting most of the districts there. The central districts are at a lower altitude than other parts of the country. It is likely that climatic factors and associated diseases are responsible for this pronounced district pattern. Food insecurity associated with drought and flooding in the shire valley, which is a result of hazardous effect of climate variation are among possible explanation for these negative effects. Furthermore the central districts are among high density population areas which affect the child’s physical environment, which in turn influence exposure to disease. At the district level, for Zambia, Figure 2, it appears that children living in provincial capital (Lusaka and Kabwe), Solwezi, Milenge, Chilengi, Kasama, Lundazi or Luangwa are significantly better-off than children in the rural areas. The negative spatial effects on child morbidity in Eastern districts (left panel of Figure 2) correspond to districts that are among density populated areas in the province, therefore their share of disease spread may be one of the major factor of this negative impact on child morbidity. From the analysis, it also appears that living in the capital cities Lilongwe and Lusaka is associated with significantly lower risk of fever in Malawi and lower risk of diarrhea, fever and cough in Zambia despite being surrounded by areas with negative district effects. Living in the capital may provide access to mosquito’s nets and health care that is superior in ways that have not been captured adequately in the fixed effects. The residual spatial effects nevertheless point in interesting directions. In particular, they suggest a fair amount of variation over and above the structured effects. Particularly noteworthy is the fact that for some urban centers, the unstructured effects point to lower child morbidity, once the fixed effects (which include a positive effect of urban areas) and the structured effects are controlled for. This is particularly noteworthy for Kitwe in the Copperbelt, but also visible for Lusaka and Kabwe in the Central part of the country. In contrast to Malawi, it thus appears that some urban agglomerations are associated with better child morbidity. The economic environment or environmental factors may cause such differentials from one district to another, differences in food prices may also be a possible reason. To explore districts differences further we postulate also that districts differences in total cost of health care and living may be indicative of the observed districts differences. Health care costs and living costs in the two countries may fluctuate considerably from one district to another due to the presence of heath facilities and erratic rainfall patterns. It is also, in this respect, of immediate policy relevance to examine the direct effect of relative food prices on childhood morbidity (Kandala, 2002). This analysis has provided an explanation of the residual spatial variation in the data and in particular it has shown that the variation is spatially structured. If this is true, it implies that adjusted diarrhea, cough and fever prevalence are similar among neighboring districts, then the possible explanation must be partly environmental. If not, a more likely explanation is that the residual spatial variation is induced by variation in unmeasured districts-specific factors. Nonlinear Effects In Malawi and Zambia, childhood morbidity is associated with child’s age and the mother’s age at birth of the child for the three ailments. While the effect of the variable “mother’s age” is almost linear for diarrhea in both countries, its effect and that of the variable ”child’s age” are clearly nonlinear. The curve has a bathtub shape, and indicates that not only children from younger mothers but also children from older mothers are at higher risk, compared to ”middle” age mothers (20-35 years old). The relationship varies across socio-cultural settings depending on levels and age patterns of fertility. Part of the negative association of morbidity risk of children between a younger mother’s age and child survival may be attributed to the tendency for young mothers to be socially and economically disadvantaged (Woldemical, 2001) and the fact that younger mothers do not often use obstetric and antenatal services much as older mothers (Magadi et al., 2000). As suggested by the literature, we are able to discern the continuous worsening of the child morbidity up to about 6 months of age. This deterioration sets in right after birth and continues, more or less linearly, until 10 months. Such an immediate deterioration in child morbidity is not quite as expected as the literature typically suggests that the worsening is associated with weaning at around 4-6 months. One reason for this unexpected finding could be that, according to the surveys, most parents give their children liquids other than breast-milk shortly after birth which might contribute to infections. Fixed Effects After controlling for the spatial dependence in the data, the fixed effects show the importance of mother’s education, household economic status, residence, the birth interval, and the antenatal visit during pregnancy, the marital status of the mother, and child’s sex on child morbidity. As we show, the key results are highly plausible and consistent with the literature. These findings point to the potential for child morbidity reduction that could result from successful efforts to improve and maintain adequate child physical environment in the two countries. We find that the risk of child morbidity through breastfeeding appears to be greatest in the first few months of life and is lower among infants who are breast-fed milk exclusively than among those who are mixed feeding in Malawi. But in Zambia, the data did not show any protective effects of exclusive breastfeeding for the three ailments. It is interesting to note that in Malawi children from large households are at lower risk of cough and children in Zambia are at lower risk of diarrhea. The impact of the household's size should, however, not be over-interpreted, since to some extent it directly mirrors infant mortality. For instance, a household with high mortality risk will remain small. In contrast, a household's size might also reflect its wealth, as a rich household will attract occupants. Again, in a large household a child might benefit from the help of several adults (Kandala, 2002). Large households may benefit from scale economies in time for child care as well as in expenditures. Alternatively, they may have become better at raising children through accumulated experience (Christiaensen and Alderman, 2001). An interesting funding for this study is that, we found that the level of maternal education was highly significant in the two countries. We also found that childhood morbidity was lower among educated women irrespective of paternal education but for fever higher the paternal education was beneficial for thr risk of fever and that although this effect attenuated with the inclusion of other socio-economic factors in the models, maternal education remained significant. CONCLUSION This analysis suggests that if interest focuses on the regression parameters β there is little to be gained from an elaborate spatial modelling exercise for these data. However, in many spatial epidemiology applications including this, the practical interest extends to constructing predictive maps for the risk of diarrhea, cough and fever throughout the country, as an aid to the targeting of scarce public health resources. Our results suggest that this requires smooth spatial interpolation of estimated districts effects in addition to smooth point estimates at any given location (district). A failure to take into account the Posterior uncertainty in the spatial location (district) would overestimate the precision of the diarrhea, fever and cough prevalence prediction in unsampled districts. The general interpretation of the inclusion of the spatial effect is that the spatial effect fspat(si) = funstrt(si) + fstr(si) represents the cumulative effect of unidentified covariates which, if they had been available, would have been included in the estimation. These possible unidentified additional covariates could be environmental, social and even cultural. Maps could be used for targeting development efforts at a glance, or for exploring Relationships between welfare indicators and others variables. The visual nature of the maps may highlight unexpected relationships that would be overlooked in a standard regression analysis. ACKNOWLEDGEMENTS This study was funded by the UK Department for International Development. The funding body had no role in the design or conduct of the study or in preparation of the manuscript. Authorship Contributions and Confirmation Both authors have access to all data in the study and hold final responsibility for the decision to submit for publication. Both authors designed the study, KNB carried out the analysis and both authors wrote the manuscript. REFERENCES
The following images related to this document are available:Photo images[ep04042t3.jpg] [ep04042f12.jpg] [ep04042f1.jpg] [ep04042t7.jpg] [ep04042f8.jpg] [ep04042f14.jpg] [ep04042f3.jpg] [ep04042t8.jpg] [ep04042f4.jpg] [ep04042f10.jpg] [ep04042t6.jpg] [ep04042t1.jpg] [ep04042f7.jpg] [ep04042t4.jpg] [ep04042f2.jpg] [ep04042t5.jpg] [ep04042f13.jpg] [ep04042f5.jpg] [ep04042t2.jpg] [ep04042f11.jpg] [ep04042f9.jpg] [ep04042f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}