 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 20, No. 2, 2005, pp. 125-141 Influence of User Fees on Contraceptive Use in Malawi Monique Hennink, Nyovani Madise Associate Professor, Rollins School of Public
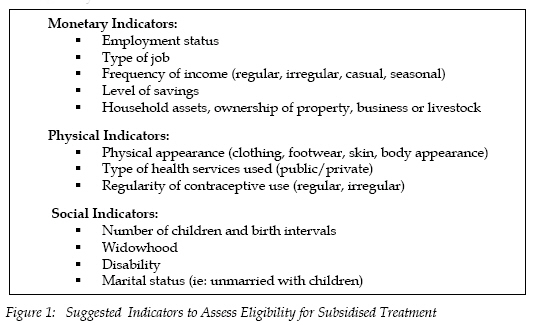
Health, Department of Global Health, EmoryUniversity Atlanta, Georgia, USA Code Number: ep05014 Abstract The introduction of cost-sharing strategies such as user-fees for health care in developing countries has received increasing attention due to declining government expenditure on health and reduced donor funding. Many governments of developing countries face the dilemma of introducing fees for family planning services while maintaining contraceptive prevalence rates. This study conducted 16 focus group discussions with poor communities in urban and rural areas of Malawi, to identify their views on the affordability of contraception and the perceived effects of user fees on their contraceptive use. The results show that amongst poor communities the long term health benefits of contraception are considered to be greater than a marginal increase in the cost of methods. An increase in the cost of temporary methods was seen as bearable, while financing permanent methods was seen as more problematic. The introduction of user-fees for family planning at government facilities would need to be accompanied by an increase in the quality of services provided to be acceptable. Those most likely to be affected by user fees are rural residents, for whom targeted assistance may be required to maintain contraceptive use. The introduction of user-fees with a subsidised treatment option was the most feasible strategy. However, the difficulties in determining eligibility for the subsidies are a critical issue. Results highlighted that the application of broader eligibility criteria are needed to account for social and non-monetary indicators of poverty in conjunction with economic indicators. Background According to evidence from the Demographic and Health Surveys (DHS), many countries in sub-Saharan Africa have started to experience the long-awaited demographic transition so that the demand for contraceptive methods is increasing. However, high fertility in the past has led to the current large proportion of women in their childbearing years, which has put heavy demand on family planning services. The health systems in many African countries are struggling to cope because of HIV/AIDS and also partly because of lack of resources. As countries face significant reduction in donor funding for reproductive health services, the issue of financial sustainability is now becoming of high priority. One solution for health providers is to introduce some form of cost-recovery scheme to generate revenue with which to improve or expand facilities. The most common of these schemes is the introduction of user fees (Collins et al., 1996; Russell, 1996; Gilson, 1997; Thomas et al., 1998; Killingsworth et al., 1999). The persistent high level of fertility in sub-Saharan Africa has prompted many governments to formulate population policies with clearly defined demographic targets. These demographic targets assume that contraceptive use will increase substantially over coming years. Clearly, many factors are necessary for contraceptive use to increase; increasing demand and acceptability for methods and improving access should be the priorities. Thus the challenge for many governments is how to achieve cost-recovery from family planning services and an increase in the contraceptive prevalence. Contraceptives are regarded by many to be social goods since they are perceived to benefit not only the individual couples but the general population. Thus, the impact of user fees on the use of contraception is a major concern for policy planners. One of the concerns of introducing user fees is that contraceptive use will fall, particularly among poor and vulnerable communities. Studies from developing countries show mixed evidence of the impact of user fees on contraceptive use. Several studies have found little or no impact of user fees on contraceptive use. Feyisetan and Ainsworth (1991), who used a DHS-type survey in Nigeria and also collected quality measures from facilities found no relationship between contraceptive use and registration fees. Oliver (1995) who used data from the Ghana Living Standards Measurement Survey and data from health and family planning facilities also found little impact of price on the use of family planning methods although the price of spermicides in private facilities was negatively associated with use. In contrast, a 32% decline in client numbers was observed in Swaziland after the Ministry of Health increased prices by 300-400% (Yoder, 1989). In Bangladesh, a social marketing project increased condom prices by 60% which led to a drop in condom sales of 29%; when prices were subsequently lowered, use rates increased again (Ciszweski and Harvey, 1995). Some economists have suggested that prices of about 1% of income appear not to affect demand (Lande and Geller, 1991) and where quality improves together with price increases, the effects of improved quality offset the demand-dampening effects of price (Janowitz et al., 1999). A review of 13 studies in Asia by Lewis (1986) found that prices were generally inelastic where increases were modest (increases of up to 20 US cents). Lewis also found that there was no difference in demand between low or moderately priced contraceptives and free contraceptives; suggesting that clients value commodities where they pay (even a small fee), which explains why fee increases of 10-20 cents may not to lower utilisation (Lewis, 1986; Foreit and Levine, 1993). Lewis did, however, find that income was a factor in determining the elasticity of demand implying that the poor were more likely to be affected by user fees than those with middle-level incomes or the wealthy. Many studies on the impact of user fees on health service utilisation in sub-Saharan Africa have tended to focus on curative services rather than preventive services. This causes difficulty in generalising the findings of price inelasticity of demand to preventive services, such as family planning, since these may not be a priority for poor people (Harvey, 1991). However, some lessons can be learnt; modest increases in user fees (e.g. up to the price of a litre of soft drinks) designated for specific items appear more readily acceptable than introducing a consultation fee (Collins et al., 1996; Gilson, 1997). Karanja-Mbugua et al. (1995) report that when user fees were introduced in Kenya in 1989, attendance at government health facilities in some rural areas dropped and only increased again after the registration fee was removed. One of the recommendations of the UNICEF’s Bamako Initiative was to use the revenue from user fees to improve the quality of health care in local communities. Indeed, this has been an argument of the proponents of user fees for family planning services. There is some evidence that where this works, there can be an increase in utilisation. A study in Cameroon found that when fees were introduced and the quality of the health services improved, the poor also increased their use of services (Litvack and Bodart, 1993). Of the studies reviewed by Russell (1996), those who increased their use of health services after the introduction of user fees, also reported an improvement in the quality of care provided. Identifying a clients’ ability to pay for family planning services is difficult. Firstly, it would involve determining the services and/or commodities foregone as a result of paying for these services. This may require lengthy determination of household income, expenditure and allocation of resources among household members. Second, most researchers and policymakers have confused the concepts of willingness to pay with ability to pay (Russell, 1996; Gilson, 1997). Some households may be willing to pay for contraceptives at the expense of other vital commodities (ie: food, safe water, school fees) or may sell assets (ie: livestock, land) to finance family planning service or method use. However, this makes them vulnerable to lower economic productivity in the long term (Sauerborn et al., 1996). To ensure that the most vulnerable people are not denied family planning services, some providers have exemptions or subsidy systems which offer free or heavily subsidised services to people below a certain income. However, evidence from previous research suggests that these strategies have not been successful (Russell, 1996; Thomas et al., 1998; Janowitz et al., 1999). Firstly, these schemes involve high administrative costs in determining eligibility and they may be inaccurate in determining an individual’s ability to pay as some household members (ie: women, young people) may be given lower priority for household resources. Secondly, subsidies may not be widely publicised to prevent abuse, so the poorest individuals may be unaware of the subsidies and not avail such schemes. One method of providing contraceptive methods to cater to individuals’ ability to pay is to provide the method at a range of prices, so that individuals self-select the price level they can afford. This method can work successfully as clients can select contraceptive methods within their means (Thomas et al., 1998). For example, variations in condom packaging may be used to obtain higher fees from those who prefer luxuriously packaged condoms and the revenue gained can be used to provide more affordable basic packaged condoms for poorer people One of the problems with interpreting studies on the impact of user fees on contraceptive use is that of methodology. Janowitz and Bratt (1996) identified two main methodological approaches: econometric theoretical modelling and the experimental or quasi-experimental approach. They argue that a basic problem with the econometric modelling approach is whether the model outputs can actually be used to predict real impact of price changes. Also the use of cross-sectional data may be problematic in that it fails to take account of consumer behaviour, whereby consumers adapt their consumption patterns to the new prices (Griffin, 1988). The experimental or quasi-experimental approach attempts to measure the changes in demand to actual price changes. One of the short-comings of this approach, however, is the neglect of method switching or consumers using alternative sources as a reaction to cost increases (Janowitz and Bratt, 1996). If a single provider increases their prices, clients may go elsewhere to obtain contraceptive methods or they may switch to a cheaper method so that the overall impact on contraceptive use may be minimal. Clearly, the impact of user fees on contraceptive use is not fully understood and more detailed research is required to fully identify the complexities of price change on contraceptive behaviour. Context of Malawi Malawi is ranked at 165 on the UNDP’s Global Human Development Index, with more than three quarters of the population living below the poverty line of US$2 per day (UNDP 2004). In addition, approximately 60 % of the rural population live in poverty and 65 % of urban residents are poor (Malawi Government, 1993). Malawi’s health system faces huge strain due to the rapid increase in population and the very high morbidity and mortality rates. At the 1998 census, Malawi’s population stood at 9.8 million, with 1.9 % annual growth (National Statistical Office, 1998). Fertility is 6.3 births per woman and the under-five mortality rate is among the highest in the world, with 234 deaths per every 1000 live births (National Statistical Office and ORC Macro 2001). Maternal health is also poor, more than 1000 women out of every 1000,000 die giving birth every year. Only 55% of pregnant women are attended by skilled personnel. About 17% of women have birth intervals of less than 24 months with the resultant risk of higher mortality (National Statistical Office and Macro International, 2001). The use of modern_contraception in Malawi is still very low. Although the contraceptive prevalence rate has tripled since 1992, only 26% of all married women were using contraception in 2000. However, there are huge differentials in use according to socio-economic and demographic factors, and the place of residence. For example; 42% of married women with secondary or higher levels of education use modern methods compared to 22% of women with no education, and 38% of urban women use modern methods while less than a quarter of rural women are users (National Statistical Office, ORC Macro 2001). Malawi also faces huge strains on its health system because of long-term illness from AIDS. Approximately 14% of adults are infected with HIV and nearly 87,000 had died in 2003 as a result of AIDS (National AIDS Commission, 2003). The provision of family planning services in Malawi has been through both the public and private sector, but only since 1987 have private-for-profit providers emerged (Ngalande Banda and Simukonda, 1994). Government health centres and hospitals offer family planning services free of charge, moderate fees are charged at family planning clinics, such as Banja la Mtsogolo(BLM) and mission hospitals, while the highest fees are charges at private clinics. Prices at private outlets are unregulated and vary considerably, for example the cost treatment for a sexually transmitted infection may range from US$0.50 to $12. Banja la Mtsologo, a non-government organisation, is an important provider of family planning services in Malawi and accounts for 61 % of the market share. It operates on a market basis to recover some costs, which enables the provision of subsidised treatment for those unable to pay. Private clinics and hospitals also offer family planning services but these are small scale compared to BLM. Other organisations such as Population Services International provide condoms through social marketing. Aims Much previous research on user-fees has focussed on the impact of fees on curative rather than preventative health services. In addition, many of the previous studies have adopted a quantitative measurement approach only and have thus not sought the views of those most affected. Although the Malawi Government has commissioned several studies to assess cost recovery from general health services (Ngalande Banda and Simukonda, 1994), no previous research has been undertaken to assess the potential influence of user fees for family planning services in Malawi. The central aim of this study is to identify the views of poor communities in Malawi on the affordability of contraception and the likely effect of introducing or increasing user-fees for family planning services on their contraceptive use. Methods The target population for this study was residents of poor urban and rural communities in Malawi, as these are likely to be most vulnerable to price fluctuations. The data were collected in 2001. Focus group discussions were used to collect information for this study as the purpose was to explore the range of influences on payment for family planning services amongst poor communities. Sixteen focus group discussions were conducted, eight each with men and women, each group comprised between 8-10 participants. The groups were stratified by gender and included only those within the reproductive ages of 15-45 years. The initial pilot group discussions were also stratified by age group, however little differences were found in the issues raised between these groups to warrant stratification by age for the rest of the study. The groups were further stratified by geographic region (north, central and south) and residence (urban, rural). The three districts selected for the study were Zomba (southern region), Lilongwe (central region), and Mzimba (northern region). These districts were selected due to their large concentrations of urban poor and the provision of both public and private family planning services in the regions. Zomba district comprises a large rural population, while the urban population comprises of a small affluent community and large poor communities in unplanned settlements.Chinamwali, an unplanned urban settlement, and Makawa village were selected as the study sites in Zomba district. Lilongwe district includes the capital city, which has large unplanned urban settlement areas; KawaleTownship was selected as the urban poor area, and Nzuluwanda village as the rural study site. Mzuzu city is the main urban location in the northern district,Zorozoro area was selected within the city and Nkhorongo village was selected as the rural site. Permission for the study was sought from appropriate community ‘gatekeepers’ in each study site; the village chief in rural areas or the community leader in urban areas. These gatekeepers identified all potential participants according to age (15-45), and asked them to gather on the day of fieldwork, the research team then randomly selected participants and assigned these to separate groups by gender. The discussions were conducted in local houses or in open fields. The fieldwork was conducted during the statutory public holidays when most residents were at home. The discussion guide included the following topics: local employment activities, family planning service use; defining poverty; affordability of contraceptive methods; and strategies for payment of family planning services Discussions were conducted in Chichewa or Tumbuka by moderators whose characteristics were matched as far as possible to those of the respondents in terms of age and gender, so to reflect the group homogeneity. Discussions were tape-recorded, transcribed and translated into English. Data analysis involved coding the textual data by themes raised by participants and entering the coded data into the ETHNOGRAPH software package. The textual data were then analysed using thematic analysis, which involves identifying issues, opinions and processes from group discussions and analysing these across the whole data set to build a comprehensive picture of collective experience. Themes were also compared between subgroups of the target population (i.e. gender, location) to identify variations in opinions or behaviour by these strata. Verbatim quotations from respondents are used to illustrate key issues or patterns of behaviour. ResultsParticipants were asked about the income generating activities within their community. In the Lilongwe urban area participants reported that the majority of men and approximately one- quarter of the women in the study areas were formally employed as drivers, mechanics or office workers. In all other study sites, the majority of the community was not formally employed. In the urban study areas many undertook informal employment such as vendors of clothing, firewood, vegetables, or roadside snacks, and beer-brewing, while in rural areas the majority was involved in brick-making or farming crops such as maize, groundnuts, beans, and tobacco. Both men and women in rural areas stated that many people relied on ganyu (casual labour) for an income. Affordability of Family Planning Services Focus group participants were asked their views on the affordability of contraceptive methods. In general, women considered the cost of contraception not in monetary terms but in relation to their health and to the costs of raising a child; an unwanted pregnancy was seen as a high cost compared to the cost of contraceptive methods. Women felt that the long term benefits of contraception were greater than the initial costs and thus thought that contraceptive methods were affordable. In contrast, men tended to assess the cost of contraceptive methods against the duration of protection. Some indicated that the condom was relatively expensive for a single sexual episode, while others highlighted that the protective health benefits of condom use were far greater than the cost. These issues are illustrated below: The price for the injection is appropriate because with K20 (US$0.20) you cannot buy a baby's napkin, but you will use contraception for three months. Even the K450 (US$4.50) for sterilisation, it’s OK because it’s expensive to be pregnant, this will help you for the rest of your life (urban women) You'd rather part with K250 in order to undergo the hysterectomy than to lose your life through excess childbirth (urban women) R1 The cost of condoms is K3.50 for pack of three. It is cheap and reasonable because the majority of people can afford to buy. Those who use them care for their dear lives as compared to the charge they pay. R4 The price generally is expensive because it is for 3 in a pack and these can only last a day. So, how much can you spend on condoms in a year? The charge is expensive. (rural men) In addition, women contrasted the more affordable costs of temporary methods (i.e. pills, injections) against the relatively expensive costs of female sterilisation. Women felt that the cost for sterilisation was harder to bear; but noted that free services were available if these costs were not affordable. It is difficult to part with K250 (for sterilisation) whereas parting with K30 (for injectables) is bearable. The cost of the short term contraceptive is quite bearable whereas the money for the permanent contraceptive is difficult to part with since it is on the higher side. (urban women) After visiting BLM I was scared of the charges (for sterilisation), I went back later and decided to buy condoms (rural women). Although family planning services are provided free of charge through government health centres and hospitals, participants highlighted a range of hidden costs which mean that users still incur costs in using the free services. Many urban participants walked to family planning services, however in rural areas distances to such services are greater, therefore using cost-free government services often entailed travelling to urban areas. In addition, rural residents stated that they had no choice of family planning provider, so if they required contraceptive methods they were often compelled to pay for these at private clinics or pharmacies available locally. The following extracts highlight these issues in rural areas: If we want to visit a government health centre then we have to pay an average of K60 per person (for transport) to and from the health centre….to hire a taxis is K350 per trip to the health centre. (rural men) Sometimes you plan to go (to a family planning clinic) on a certain date, then you don’t have money on that date for transport… sometimes you wait at the bus stop but by the time you arrive the clinic is closed (rural women) Those who live close to the health centre get them (contraceptives) free of charge, while those who live far from the health centre have no choice but to buy them. (rural men) Participants reported that the government health facilities sometimes had stock-outs of contraceptive methods. In such situations users were asked to return at a later date or were referred to family planning clinics such as BLM or private providers to obtain contraception and ensure continuous contraceptive coverage. Officially such referrals are meant to receive free contraceptive methods from the alternative services but the reality is that women were still required to pay for additional costs such as registration fees or pregnancy tests. For example, it is a requirement at BLM clinics that women undergo a pregnancy test before receiving contraceptive methods. However, the cost of this test can be prohibitive to those seeking free services. For example: In some instances, at these free service centres you may be greeted by non-availability of the products and consequently you are advised to go back some time later. By that time contraception becomes a non-starter (urban women) It sometimes happens that at free health service centres there are no medicines, so you are constantly advised to go to Banja La Mtsologo clinic, but you don’t have any money. (urban women) Some don’t use methods because the government clinics have run out of supplies and they can’t afford to buy pills at the pharmacy (urban women) When you go to BLM and say that you want to start using family planning methods they tell you that you must provide proof that you are not pregnant. So they do tests on you but you must pay for these. I think that the charges for the tests are too high. These tests should be free. So all together, you may end up paying K360. That is a lot of money especially if you are not working. (urban women) Almost all participants highlighted that the quality of care provided at the government health facilities was a disincentive even though the services were free. In particular, the long waiting times, poor treatment by staff and frequent stock-out of contraceptives discouraged the use of these facilities. Many participants stated that if they have the money they prefer to utilise BLM or private services to obtain contraception. The following extracts show typical comments made: As soon as you arrive at Banja La Mtsologo clinic, present your problem and declare your favourite method you are instantly attended to, so that before long you return home. In contrast, when we go to a public health facility you are made to wait intolerably long hours unattended. That’s why we reluctantly take recourse to the private centre. (urban women) If you have cash you would certainly proceed to BLM clinic because you know you would be given immediate attention and return home quickly… You would leave behind those people who were in your company and opted for the Government hospital… (urban women) Although participants identified that the direct and indirect costs of family planning services could discourage contraceptive use, they also noted that cost barriers were just one of a range of barriers to the use of contraception. Participants also identified non-financial barriers to contraceptive use, such as fear of side effects, desire for more children, religious opposition, husband’s disapproval of contraception and method dissatisfaction. Therefore the cost barriers need to be considered within a context of other non-monetary barriers to contraceptive uptake. Effect of Price Increases Participants were asked whether they would be willing to pay a contribution towards the costs of using family planning services. Participants stated that they would only be willing to pay for curative health care and would be willing to forgo essential items (i.e. food) to cover the costs, as the treatment would be essential for survival; but payment towards preventative health, such as contraceptive methods, was given low priority. However, when asked if contraceptive use would continue if fees were introduced in government outlets and increased at BLM and other private providers, many felt that contraceptive use would continue and that the costs would be covered, albeit with some difficulty, as shown below: What if the contraceptive pill is raised from K30 to K45, would people be discouraged? We can manage to buy. We can still buy, but with difficulties. (urban women) If prices are adjusted upwards, people automatically adjust and would go on using, not so many would be discouraged. They could go on to the extent of borrowing money so that they are able to purchase the contraceptives. (rural men) In my view, if Banja La Mtsogolo clinic raised the cost of its family planning service the number of attendees or customers wouldn't change that much. However, potential customers from the village would be tremendously discouraged. People would want to have their desire satisfied, despite the price increases. (rural men) Some felt that the introduction or increase in fees for contraceptive methods would lead to an abandonment of contraceptive use and an increase in unplanned pregnancies and transmission of sexually transmitted infections. For example: Some will go on. If you are serious about family planning you will continue, however, if you are having difficulty making ends meet you might stop using the pills (rural women). If the cost of the condom goes up…it would be a problem and therefore the spread of venereal diseases becomes wide. If one doesn't have K5 (for the condom), one would go ahead with unprotected sex to release frustrations because of protracted abstinence. (urban men) It was clear that those who would be most disadvantaged by an introduction of costs or cost increases would be rural residents and the urban unemployed. Many rural participants stressed that they currently experience difficulty to purchase essential items for survival, so would face extreme difficulty to pay for continuous contraceptive coverage if fees were introduced, as shown below: Think of an unemployed person, where would he get money for condoms? (urban men) If people don’t have enough money to go to the hospital when they are ill, it is difficult to pay for contraceptives. You cannot buy contraceptives when your family is hungry (rural women) There is no way if one has toiled for a whole day to do a job to earn money for food, then later on he uses it for family planning methods. If you are failing to buy food how can you put condoms on a budget? It’s impossible. If I find money I will buy food for my family. I can’t spend money on useless things! (rural men) Participants stated that they would not be willing to pay for family planning services from government facilities, which they perceived to provide the poorest quality of care, particularly with respect to waiting times, treatment by staff and availability of supplies. Others feared that an introduction of fees would soon escalate and services would no longer be economically accessible. However, participants were more willing to accept payment for services from private family planning clinic providers or BLM since they recognised the better quality of service provided. Cost-Sharing Strategies Focus group participants were asked about the feasibility of a range of cost-sharing strategies, including, health care subsidies, health insurance and credit schemes. The range of issues discussed is highlighted below. a) Subsidised Treatment One strategy for cost-sharing of family planning services is to introduce a user fee with the availability of subsidised treatment for those unable to meet the charges. Subsidised treatment funds were seen as a viable cost-sharing strategy by many participants as they felt it would enable users to continue contraceptive use whereby they would only contribute a manageable amount for service use. Most participants felt that this was a fair strategy as those who are able to pay will be charged for services, while the most disadvantaged would receive reduced fee services. However, some felt that in poor communities even a small contribution towards service use was not feasible. Let's consider the costs at Banja La Mtsogolo which were K300…then the government introduces a subsidy to the effect that the service consumers have to pay only K100 to access the family planning service. People would discuss in their families and decide to seek the K100. Now to pay K300 to Banja La Mtsogolo clinic is so disturbingly hard because it leaves you helpless… (rural men) Yes, the government should help us a little. Even those of us who have a little money would appreciate government subsidies. We would be willing to pay a little. (urban women) Are you saying that the government wants us, poor people, to pay something toward our treatment? We have no money. We shall die! (urban men) The key issue in implementing subsidised treatment schemes is the criteria used to determine eligibility for subsidies. While monetary indicators may seem a viable means to assess eligibility, participants opined that amongst poor communities income-based measures may be unreliable due to the high level of unemployment and erratic incomes from casual or seasonal employment. This was particularly true of rural incomes. For example: If I produce some timber I'd make K300 per month. It's not possible to state [average earnings] because work can be seasonal. There are times when crops become quite affordable, such seasonal changes affect timber sales. There are other occasions when timber is plentiful at the market. What that implies is that a piece of timber that would normally fetch K20 can be sold for as low as K9. Thus it becomes difficult to estimate the average income. (rural men). Therefore, participants stated that monetary indicators alone were not sufficient to identify an individual’s eligibility for subsidised services, consideration also needs to be given to a range of social indicators of poverty to more clearly identify those who may be disadvantaged and require access to subsidised services. Figure 1 shows a range of economic, social and physical indicators identified by all participants which may more fully determine poverty status. Participants highlighted that any one of these indicators alone was not sufficient and may be misleading, but a combination of social and economic indicators would be required to assess the eligibility of individuals for the subsidised treatment funds. b) Health Insurance Schemes Participants discussed the feasibility of community-based health insurance schemes to assist with the payment of health care, including family planning services. This may involve community members contributing to a common fund and accessing the fund when healthcare is required. Although community members saw the benefits of community insurance schemes, particularly for emergencies and when money is limited, they felt that this strategy would be less feasible amongst poor communities primarily due to the lack of surplus money to contribute to the fund. Participants also felt it would be difficult to decide which illness warranted assistance from the fund and family planning services may not be seen as a priority. In addition, high unemployment and a transient population in urban slum areas would mean that many would not contribute. There was also a fear of mismanagement of the fund and that its use may be dominated by richer or influential community members and the poorer members would lose access. These issues are shown in the extracts below: Sometimes, an emergency difficulty occurs when you don't have money. Therefore the notion of a fund establishment would prove beneficial in that people would resort to the fund to meet health service costs. That sounds possible (urban men) R1 I accept to have the fund set up to assist the government, but not by the poor people in villages… R5 The set back to such kind of a fund is that there will be a lot of pretences of illness in order to take the money to solve other personal problems. It will be difficult sometimes to decide on which illness could be allowed to benefit from the fund. (rural men) We don't have money, where would we find the money for such a fund, it’s very difficult… here there are only unemployed people. People in this area are rough, they might attack the chief, wanting the money to use for alcohol. (urban men) c) Credit Schemes The use of credit systems or borrowing money to cover the cost of using family planning services was not seen as a viable option due to poverty and repayment difficulties amongst the poor and unemployed. The benefits of credit schemes for health care emergencies were acknowledged, but only seen as an option for richer communities and those in regular employment. Participants in urban areas noted a range of payment options with some private health care providers, including, deferred payment arrangements and payment in instalments. Make an arrangement for deferred payments…then the use of the family planning service would be promoted that way (urban men) In private hospital you are allowed pay in parts for an agreed period of time… (urban women) What about if you got treatment on credit so that you could pay at the end of the month? Yes. This is okay for those who are employed. However this would not work for the unemployed. What would you pay with? (urban women). Discussion and ConclusionThis study found that poor communities assessed the affordability of contraception not only in simple monetary terms of the cost of a method, but in relation to the health benefits of avoiding a further pregnancy and the cost of raising another child. Therefore, many residents of poor communities felt that contraceptive methods were affordable. Many felt that the actual cost of temporary methods (pills, injections) was acceptable and would still be affordable even with price increases of 30-50%, but financing permanent methods of contraception was much more difficult. This may imply that with user-fees for family planning services, poor women may opt for more affordable temporary methods of contraception even though they would prefer sterilisation. Even though family planning services are currently free of charge at government health facilities, a range of situations (i.e. method stock-outs) and hidden costs for referrals (i.e. transport, registration fees or pregnancy testing fees) meant that users still incurred costs to use the free services. These costs placed a greater burden on rural residents wishing to access family planning services, either due to high transport costs to access services, or the lack of provider choice in rural areas which compelled them to use private facilities. The implications of these findings are that the introduction of user-fees is likely to have a greater burden on rural residents wishing to use contraception. To overcome a possible decline in contraceptive users there needs to be greater co-operation between public and non-public service providers, perhaps to identify cost-waivers for the additional fees incurred by those referred from Government facilities. Would the introduction of user fees alienate the poor from using family planning services? The findings of this research show that although poor residents may experience difficulties in paying for contraceptive methods, most would continue to use contraception, as long as the cost (or cost increase) was modest (say by 10-20 cents). However, the introduction of user fees may have a differential impact on poor communities, with the greatest hardships placed on rural poor residents whose incomes are meagre and dependent on unreliable crop yields. Rural communities currently face high levels of poverty and increased costs in using family planning services, therefore the additional burden of user-fees would not be sustainable. In addition, the unregulated price structure of contraceptives in private outlets could also impose additional burdens on rural communities, as it is possible for prices to be higher in rural than urban areas. Although there was a willingness to pay a small fee for family planning services, this would need to be accompanied by a noticeable increase in the quality of service provided. Many participants in this study were not willing to pay for current services at government facilities which they felt offered the lowest quality of care. An implication of this finding is that the introduction of user fees may lead to a change in consumer behaviour, with clients forgoing fee-paying government services for higher quality of care provided at other outlets. Although the provision of subsidised treatment for those most vulnerable was seen as a positive strategy, the difficulties in determining eligibility for subsidies was seen as the critical issue. This study showed that identifying eligibility for subsidised services solely via economic indicators is inadequate; poor communities themselves consider a range of social and physical indicators together with economic determinants in assessing poverty. Therefore, eligibility for determining access to subsidised family planning services needs to apply broader criteria and should include non-monetary indicators of poverty. Other cost-sharing strategies such as health insurance or credit schemes were not seen as viable in poor communities due to the lack of surplus cash and the high unemployment. In conclusion, there are three key findings from this study with regard to the dilemma of introducing user fees for family planning services while maintaining contraceptive prevalence rates. First, contraceptive users in poor communities consider the non-monetary benefits of contraceptive use to be greater than an increase in cost of methods, and therefore an introduction of fees is likely to have little impact on contraceptive prevalence. However, user-fees at government facilities would need to be accompanied by an increase in the quality of care in service provision to be acceptable. Second, those most likely to be affected by price increases are rural residents and the unemployed urban residents for whom targeted assistance may be required to maintain or increase contraceptive use. Third, the introduction of user fees with subsidised treatment funds appears to be a feasible strategy; however, the application of broader eligibility criteria which account for social and economic indicators of poverty would need to be developed. This study has provided an understanding of how poor communities themselves regard the affordability of family planning services and the likely impact of user-fees on their contraceptive use. Further research is needed to identify how households would finance user fees for family planning methods and whether this would have longer term detrimental effects, through sacrificing vital commodities to pay for contraception and thereby creating greater vulnerability amongst poor communities. Acknowledgement This study was funded by the UK’s Department for International Development Knowledge Programme, Opportunities and Choices, based at the University Of Southampton, UK. References
Copyright 2005 - Union for African Population Studies The following images related to this document are available:Photo images[ep05014f1.jpg] |
| |||||||||

{kind=link}