 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
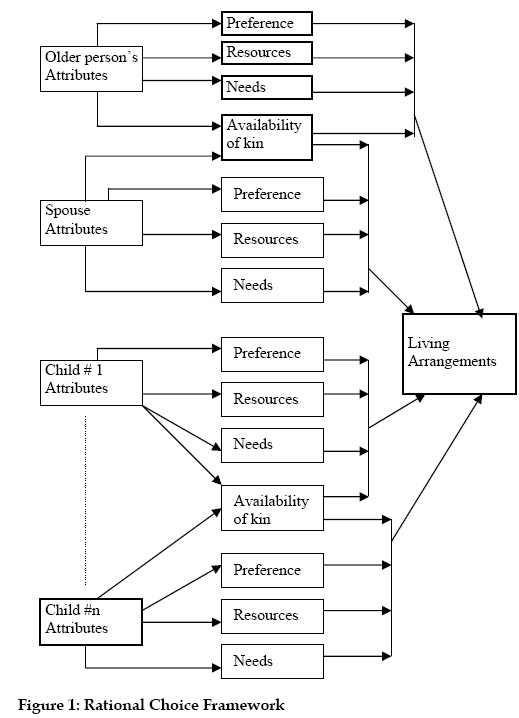
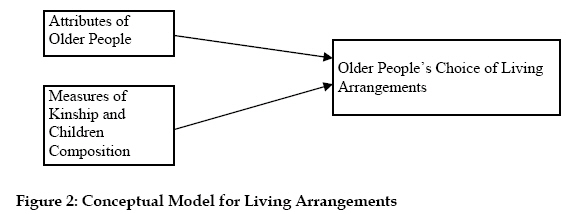
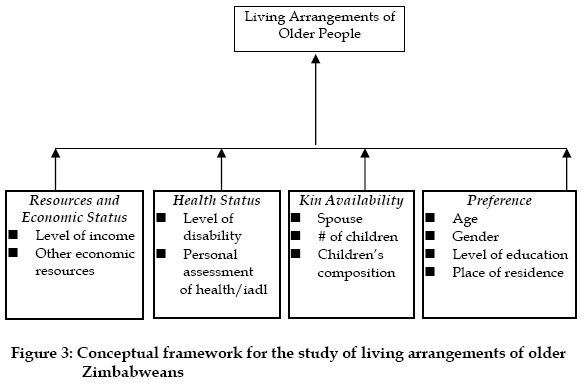
African Population Studies/Etude de la Population Africaine, Vol. 20, No. 2, 2005, pp. 143-163 Living Arrangements and Conditions of Older People in Zimbabwe Sitawa R. Kimuna Department of Sociology, EastCarolinaUniversity, A-408 BrewsterBuilding, Greenville, NC27858-4353, USA Code Number: ep05015 Abstract This research uses data from the 1994-1995 Zimbabwe Aging Survey complemented by the 1999 Zimbabwe Demographic and Health Survey to examine living arrangements and conditions of older people in Zimbabwe. Living arrangements in Zimbabwe are similar to those found in other sub-Saharan African countries. Older people are likely to be living with other kin and in a variety of arrangements involving family members. To determine gender preference for co-resident with children and other kin, we adjust living arrangement patterns for sex, dominant proportion of living children and marital status. Data show that older people with living adult children are more likely to co-reside with kin. However, older people with a dominant proportion of married children are significantly (p<0.01) less likely to co-reside with married children. Furthermore, households headed by older women are significantly (p<0.001) less likely to co-reside with kin. Introduction Like any other country in sub-Saharan Africa, the population of older people in Zimbabwe is increasing. The increase in Zimbabwe’s older people is due in part to the decline in fertility rate that started since 1980s. The total fertility rate was six children per woman in 1985; currently it is 3.6 children per woman (ZDHS, 1999). This decline could largely be attributed to successful government and voluntary family planning programs and efforts to provide the population adequate access to family planning methods. The continued changes in the levels of fertility are spearheading a transformation of aging to the Zimbabwean population (Kimuna, 2005a; 2005b). Whereas 42% of Zimbabwe’s population was under age 15 years in 1999, 4% was aged 60 and above (UN, 2000). With rapidly declining fertility, the proportion of the aged would continue to increase, altering the age structure of the population. As the age structures of countries such as Zimbabwe undergo dramatic changes, governments may want to plan for populations that have been previously overlooked. In most sub-Saharan African countries and especially Zimbabwe, older people have not been considered as a policy issue due to the belief that families still remain as the strongholds of support. Although traditionally the family was the single most important source of support for older people in sub-Saharan Africa (Adamchak et al., 1991; Adamchak, 1996; Kimuna, 1999; Nyanguru, 1994; Nyanguru et. al., 1994 and Wilson et. al., 1991), the current demographic and social changes occurring in Zimbabwe and elsewhere in Africa have disrupted some of the inbuilt safety nets that were in place for older people. Studies on the social support systems of older people have increased in the last three decades; however, research on living arrangements in sub-Saharan Africa is scarce. Studies of living arrangements of older people can therefore make an important contribution to understanding their survival, especially older people in sub-Saharan Africa. In this study we examine the living arrangements of older people in Zimbabwe. The aim is to identify the existing structure of living arrangements and support, and the nature of family relationships of older people. We analyze the attributes of older people on living arrangements and also examine their co-residence with adult children to determine whether the prevalence is associated with socioeconomic variables, region and gender of the older person. Theoretical Explanations: Rational Choice on Living Arrangements of Older People To address the living arrangements of older people in Zimbabwe, we assume that their living arrangements are responsive to the changes in the life course of their children or kin1. Family is the locus where older people live and are often supported by kin (Chilungu, 1989). Different types of living arrangements are shaped, sustained and transformed by both structural and cultural conditions that permeate different societies. Blieszner and Bedford (1995) noted that living arrangements are not only determined by migratory status and availability of children, but also by a set of individual characteristics such as sex, marital status, economic status and health. These researchers suggest that choice, necessity, and social customs molded by the historical fabric of society invariably generated diverse conditions for living arrangements, which then led to support. Rational choice recognizes the effects of demographic factors such as the availability of kin, which circumscribe living arrangements and support of different family members. Also, it accounts for the interdependence of needs, resources, and nonmaterial factors (Ofstedal, 1995; Wolf and Soldo, 1988). Accordingly then, rational choice framework includes resources, needs, kin availability, and preferences (see Figure 1). Preferences underlie family members’ choice of living arrangements and support when needs, resources and other potential opportunities do not define these factors. Ruggles (1987) introduced the preference factor to capture non-material elements such as emotional bonds and social values. These four factors, resources, needs, kin availability, and preferences encompass many aspects of older people’s attributes including their current and past experiences. Socioeconomic factors such as age, gender, educational attainment, marital status, work history, income, place of residence, visiting patterns of kin and friends are implicitly or explicitly part of the four main factors of the framework. A model derived from the above framework (see Figure 2), which concentrates on the attributes of older people is estimated in this study. This model has been widely used in the study of older people’s support systems (Tsuya and Martin, 1992; Spitze et al., 1992; Spitze and Logan, 1990; Ofstedal, 1995). In addition to older people’s attributes, the model incorporates some measures of kinship network and older people’s children. Other measures include gender, age composition, marital status, educational attainment and occupation of children and kin, who might play a role in the relationship. The contributions of the other family members’ attributes are limited to defining the potential opportunities available to older people (see Figure 3). The conceptual framework has been used in many studies of older people’s living arrangements and social support around the world (Burr, 1992; Da Vanzo and Chan, 1994; Wolf, 1984; Wolf and Soldo, 1988). The framework acknowledges that observed living arrangements and other aspects of social support within the family are the net outcome of the interactions between the significant attributes of different family members. In other words, family members choose their living arrangements according to their resources and needs. For example, sufficient economic resources and good health have been cited as factors that promote solitary living arrangements. On the other hand, declines in health and economic need encourage co-residence with other family members (Adamchak et al., 1991; Asis et al., 1995). Also, the model recognizes the effects of other factors, which are introduced through kin availability. These factors identify the opportunities that circumscribe living arrangements and support of different family members. Non-material factors are introduced through preferences, which underlie family members’ choice of co-residence, when these are not defined by needs, resources and potential opportunities. The strength of the model is its ability to account for the influence of needs, resources, demographic and non-material factors in defining the living arrangements for different members of the family. We begin by describing the factors that determine co-residence of older people. Resources of Older People Research has shown that the needs and resources of older people determine the feasibility of the available living arrangements (Burr 1992). Feasibility relates the economic and health variables to the living arrangements of older people. Thus, being healthy and having adequate resources would make independent living a possibility. Other research has stressed the effects of economic status on living arrangements and social support of older people. However, there are distinct effects for two different types of economic resources: First, income levels and ownership of real assets and personal income, while the second, human capital, refers to the personal resources generated through time and experience, which also requires a certain level of education. In sub-Saharan Africa, where agriculture dominates, there is no retirement provision for the labor force other than illness and disability (Hampson 1985). The economics of aging in sub-Saharan Africa and particularly in Zimbabwe cannot be reduced to the extent of work, and income. Work as defined here is an activity performed for others for which the individual is rewarded monetarily. The link between the individual and work is important because of the relationship between the individual’s income and his or her work status. The importance of work to the older person lies in the fact that income is closely related to previous or current work status. In Zimbabwe and elsewhere in sub-Saharan Africa, mostly older people are illiterate, poor, and live in rural areas. Heslop (1999) noted that older people in rural locations engage in informal work or activity that does not guarantee steady income. Moreover, in most sub-Saharan African countries, centrally developed systems for income security in old age are extremely limited (Kimuna and Adamchak, 1999; Kimuna, 2005a). In practice, eligibility is restricted to a small minority of workers previously employed in the formal sector in urban areas, such as government staff and employees of large-scale public or private enterprises. The World Bank estimates that over 70 percent of the world’s older people rely on informal systems of security (World Bank, 1994) and this percent is certainly higher among older people in developing countries, especially in sub-Saharan Africa. Research has shown that assets and personal income, which is associated with high levels of education, enable older people to have privacy and reduce the likelihood for co-residence (Michael et al., 1980). Others have indicated that older people prefer to maintain a separate household but keep close contact with their family members, a phenomenon that researchers refer to as “intimacy at a distance” (Shanas, 1980; Soldo et. al., 1990; Hashimoto, 1991). On the other hand, lack of resources or poverty increases the probability of co-residence. Another important factor that determines co-residence is the extent to which older people provide economically valued resources to co-residing members in the household. For example, older people may provide services such as childcare and other types of support to the family (Martin, 1989). Older People’s Needs In addition to sufficient economic resources, good health is the other major requirement for self-reliance and independent living (Soldo and Freedman, 1994). Self-reliance of older people is strongly related to their current economic situations, activity, health, living arrangements and availability of social support. With declines in health status and increased disability, older people experience difficulties with many activities of daily living ranging from the preparation of meals to bathing, dressing, grooming, housework, planting, weeding, harvesting, collecting water and collecting firewood. These needs increase the chance of co-residence and social support. The tendency for co-residence due to disability also depends on the marital status of the older person and the health of the spouse. The presence of an able spouse lessens the probability of co-residence with kin since the spouse can care for the disabled partner. Single older people including widows, separated and never married are more likely to depend on other family members in cases of poor health. The unmarried women face a double challenge in responding to the gender implications of aging. On the one hand, they are disadvantaged in the life expectancy “advantage” for women (Ewing, 1999) often-outliving husbands who might otherwise provide economic support. Older women are one of the poorest population groups, yet they are often the primary caregivers for another impoverished group, children. In Zimbabwe and elsewhere in sub-Saharan Africa, the poorest older women, be it urban or rural grandmothers, have taken on the responsibility of caring for the most vulnerable in their communities; that is, children and grandchildren with HIV/AIDS in the absence of any state or formal support (Kimuna, 2005b). Elderly women are thus most vulnerable and are at risk of being more dependent on informal support. The need component also recognizes the importance of cultural preferences. Even when older adults have adequate resources, they may still want to live with kin simply because it is culturally appropriate. Kin Availability There is now a growing body of research on older people’s social networks and availability of kin, including some research on variations in these networks between, for example, rural and urban areas (Wenger, 1996). Other studies have identified kin availability as the major source of support available to older people (Soldo et. al., 1990; Heslop, 1999; Gorman, 1999). The assumption underlying these studies is that a positive relationship exists between the size of kin network and the probability of co-residence and receiving social support. Waite (1995) found a relationship between kin and social network availability and psychological well being of older people. Others have incorporated detailed information about kinship network (Wolf and Agree, 1990; Spitze and Logan, 1990; Wolf, 1990; Wolf and Soldo, 1988). These studies found that the size and structure of kin network can significantly strengthen explanations of older people’s living arrangements. They argue that the number of children and their characteristics such as gender, marital and economic statuses may affect their ability to support older people. However, research on poverty among older people has provided an understanding of its consequences beyond the lack of physical necessities, income andmaterial assets (Chambers, 1995; 1997). Illiteracy, unemployment, powerlessness and physical weakness due to malnutrition and illness are often concomitant of poverty and lack of support for older people. Preferences The preference factor captures those elements of older people’s attributes that are not captured by the measures of needs, resources, kin availability and other opportunities. The preference factor assumes that there are differences between cultural and ethnic groups regarding older people’s living arrangements. Since such differences are difficult to capture, socioeconomic and regional variables are commonly used as proxies for them (Wolf and Soldo, 1988; Da Vanzo & Chan, 1994). Studies of cross-cultural comparisons have used ethnic characteristics as proxies (Burr, 1992; Casterline et al., 1990). In African societies, Chilungu (1989) noted that preference factors of older people can be identified with their adoption of traditional and non-traditional attitudes. Traditionalists have a high level of co-residence and social support mainly provided by their families. This is because of older people’s respected status within the family and not necessarily because of needs. Conversely, with non-traditionalists, preferences will result in low levels of co-residence, and support is provided only on the basis of rationalization of resources versus needs. We use personal as well as regional (rural and urban) factors to examine preference factors in this study. Although age, gender, educational attainment, and region are part of the older people’s life course attributes and are implicitly included under other factors affecting living arrangements, these factors are used as proxies for preference because of their distinct effect on older people’s choices. Age is frequently associated with high levels of declining health and economic need. In developing countries, old age and poverty are intimately linked (Kalache and Sen, 1999). Health in old age is greatly determined by the patterns of living, exposure and opportunities for health protection over the life course. Age also reflects to some extent a cohort effect on older people’s preferences. That is, older people tend to be more traditional than young people. Consequently, high levels of co-residence are expected. The same argument holds for educational attainment. Although educational attainment can provide older people with means and resources that can influence their economic and health status, it has the distinct effects of exposing them to new and non-traditional attitudes (Da Vanzo and Chan, 1994; Chilungu, 1989; Burr, 1992). Data and Methods The study uses data from the 1994/1995 Zimbabwe Aging Survey Project. These data were collected by international researchers in collaboration with the University of Zimbabwe to provide a portrait of Zimbabwe’s aging population. The protocol of the survey was to collect information on the demographic, social, economic, cultural, sources of support, life-style habits, health and access to health resources, activities of daily living (ADL) and physical characteristics of older people. Trained and supervised indigenous interviewers used a standardized questionnaire to collect data from respondents during interviews in the respondents’ homes. A total of 278 respondents aged 60 years and over from the sampled urban and rural areas were interviewed with nearly 100% response rate. Sampling Design The survey used a three stage random cluster sampling design to ensure that respondents were distributed throughout the targeted areas: Maramba, Pfungwe, Uzumba, Bindura and Marondera. The rural sample of 174 respondents was from Maramba, Pfungwe and Uzumba, in North Eastern Zimbabwe covering an area of 2646 km (CSO, 1969 quoted in Allain et al., 1997). The rural area’s farthest point from the capital city of Zimbabwe, Harare, is 245 kilometers and its nearest point from Harare is 120 kilometers. The area was divided into 15 wards, each ward with six village development units (VDUs). Each VDU comprises 60-100 households. The population in 1992 was 86,308, with 5,793 (6.7%) over 60 years (CSO, 1969 quoted in Allain et al., 1997). For each ward, one VDU was selected at random and interviewers proceeded to visit alternate households where members over 60 years were requested to participate in the survey. The urban area sample of 104 respondents was from Chipadza in Bindura and Dombotombo in Marondera. Both towns are approximately 85 km from Harare. Bindura had a total population of 21,167, of whom 508 (2.4%) were aged over 60; the population of Marondera was 39,384, with 1,194 (3.0%) over 60, respectively. The urban townships were organized on a grid pattern and respondents were selected from alternate houses within alternate streets, using the same criteria as rural respondents (Allain et al., 1997). In addition, for both rural and urban areas, wherever possible, males and females were selected alternately to obtain an equal sex ratio. However, when there was only one subject aged over 60 in the next household, they were asked to participate regardless of sex. This resulted in a slight excess of females in the study population. In the households where there was more than one eligible member of the same sex only one was counted (alternately the younger and the older of the pair). Many subjects did not accurately know their own age. For these subjects, age was estimated based on physical appearance, the age of oldest children, grandchildren or great-grandchildren and memory of major historical events, such as the influenza epidemic of 1918, the locust plagues of the 1920s and the Second World War (when many Zimbabweans were conscripted). The appropriate institutional ethical review board in Zimbabwe approved the survey. Ideally extended time-series data on co-residence and comprehensive development indicators should be used for an analysis such as this. Unfortunately, these data are not available. Hence, we rely on this available baseline data to examine the living arrangements of older people in Zimbabwe. Further, the data set contains a considerable amount of information useful in the study of older people, but the size of the sample and limitations in the sampling area tend to restrict the representative ness of the sample. Table 1 shows percent distributions of the survey sample by age groups, place of residence and gender. The majority of the sample (63%) was located in the rural area. Older people between the ages of 60-69 were almost 44%, while the majority (56.4%) were 70 years and over. The mean age of the study sample was 72 years of age. A breakdown of the percentages for each age group is also presented in Table 1. There were more females represented in the population sample, almost 56 percent (55.8%; N=155) than male population sample of 44.2% (N=123). Older adult women outnumber men in almost all countries of the world. However, the trend is more so in developed countries than in developing countries. Table 1: Percent Distribution of Respondents’ Age Group, Gender and Place of Residence
Source: 1994/1995 Zimbabwe Aging Survey Project Study Variables Living Arrangements Data regarding living arrangements were specified by unique categories of relationship to older people. Several categories that reflect living arrangements of older people were constructed. The two categories of “living alone” and “living with spouse only” were pooled into one as the reference category. In order to create this reference category, older people living with spouse only were included in the “living alone” category. A dummy variable was created for living arrangement with respondents living with other family members. Table 2 explains the independent variables, availability of kin (we use the number of living children), age, economic status, gender, education and place of residence. Demographic Indicators The demographic variables of gender, marital status and age are indicated by female headed household, couple household and age. The variable for female headed household is coded as “0” or “1” with “1” representing female headed household and “0” representing male headed household. A dummy variable was created for couple household, which indicates “not married” with the value “0” (including divorced, separated, and widowed) and the value “1” referring to married. Two dummy variables were created for age. Age65 as dummy variable is “0” if older people are not between ages 65 and 74 and “1” if they are between the ages of 65 and 74. Age75 dummy variable is “0” if older people were not age 75 and over and “1” if they were age 75 and over. The age category of 60-64 was used as a reference category so no dummy variable was needed. Table 2: Definitions of the Dependent and Independent Variables Included in the Statistical Models of Living Arrangements
a instrumental activities of daily living; 1includes those older people who reported being able to perform the IADL with some help. Potential Opportunities for Co-residence Family size was drawn from the question that asked about the number of living children the respondent had and their characteristics. Answers to this question varied from “0 to 14”. Another variable was living with children in the same household. This was derived from the question that asked the respondent to identify other household members. A choice of potential persons was given and multiple answers could be expected. A dummy variable was created for the variable “living children”, “0” for those older people who did not have living children and “1” for those with living children. Needs This category had two variables derived from several questions in the survey. Respondents answered questions regarding their health status and whether or not they suffered from any chronic illness that prevented them from performing instrumental activities of daily living. The variable “suffering a chronic illness” was coded “1” and “not suffering from a chronic illness” was coded “0”. Health status variable was derived from an index of instrumental activities of daily living. Older people who were not able to perform instrumental activities of daily living were coded “0” and those able to perform one or more of these activities were coded “1”. Resources This category was derived from the question that asked respondents to indicate if they owned a home and land. This is one of the variables that might facilitate independent living and also reflects economic status of the elderly. A dummy variable was created indicating “0” for older people who did not own both land and a house and “1” for those who owned land and a house. For the education variable, respondents were asked to indicate the number of years they had attended school, based on six educational levels, illiterate (never went to school), primary school, secondary/high school, teacher training, technical college/polytechnic and university. In Zimbabwe, primary school takes seven years. For the purpose of this study, this variable wascoded as a dummy variable with “0” for older people with less than primary education and “1” for those with 7 years of education or above. The education variable will also be used in the analysis as a proxy to measure traditional attitudes. Cultural Factors The place of residence is a factor that is considered to be crucial in assessing social support of older people. Thus, the geographic location is an important factor in this study since 63% of the sample population was rural. The urban place was coded as “0” and rural place as “1”. Regression Analysis Logistic regression analysis was used to test the study hypotheses stated below: Cultural Factor H1. Owing to the out-migration of young people from rural areas, location of older people in an urban area will increase the likelihood of co-residence with children. H2. Female older people who are heads of households are more likely to co-reside with other family members than male older people who are heads of households. Kin Availability H3. Older people’s households with adult living children are more likely to co-reside with children. H4. Having a dominant proportion of children who are married increases the probability of older people co-residing. Needs H5. Older people who experience poor health and any disability in activities of daily living are more likely to co-reside with adult children. Resources H5. Older people with higher economic status are less likely to co-reside with other family members. H6. Older people with a high level of education are less likely to co-reside with other family members. Due to the categorical nature of the dependent variable (living arrangements), we used a multivariate logistic regression model. The association of living arrangements and the attributes of older people were examined in three models plus a fourth model that included all predictor variables. The first model examined the association between each of the older people’s attributes on living arrangements without controlling for the effects of other attributes. The second model introduces three control variables (female headed household, age and place of residence) to the relationship. The third model introduces the potential opportunities and needs variables. In the fourth model, all independent variables are included: (1) the effects of the demographic attributes of older adults on their living arrangements; (2) the effects of kin availability on the living arrangements; (3) Needs or health status; (4) social and economic status on the living arrangements, and (5) the cultural and regional factors. Results The first model in Table 3 tests the hypothesis that female older people who are heads of households are more likely to co-reside with other family members than male older people who are heads of households. The odd ratios in Model 1 show a significant negative effect on co-residence for older female headed households. This result contradicts our hypothesis. This is an unexpected finding given that elsewhere, research indicates that female older people display closer relationships with kin than do male older people (Schrage-Dijkstra, 1994), and therefore, they are more likely to co-reside with kin. Nonetheless, in a predominantly traditional society such as Zimbabwe, male older people continue to maintain their positions as heads of households in later life, whereas female headship increases with age largely due to widowhood, which also contributes to the declines of average household size. Further, results indicate no significant difference regardless of the place of residence. In our sample, the majority of older people lived in the rural areas (63%) compared to the urban residence (37%). As noted in the cultural factor hypothesis, rural to urban migration of young people would increase the likelihood of older people living with kin in urban areas. However, the findings in model 1 are not significant. To assess the influence of the potential opportunities variables, we included two variables in Model 2: “number of living children” and their attributes (dominant proportion of children that are married) to the base model. The results show that the number of living children increases the likelihood (at p<0.0001 level) of older people living with kin. This finding supports our hypothesis that kin availability will decrease the likelihood of older people living alone or with spouse only. Martin (1989) points out that the negative association between kin availability and the probability of living alone/with spouse only is not restricted to countries where co-residence is the norm. He notes that even in developed countries where co-residence is not the preferred arrangement, there is a significant relationship between kin availability and co-residence. Further, model 2 shows that having a dominant proportion of children who are married has a significant negative effect on living with kin and therefore, increases the likelihood of older people living alone/with spouse only. This finding contradicts the hypothesis that older people with a dominant proportion of children who are married are more likely to co-reside. To assess the influence of needs, we added indicators: “able to perform instrumental activities of daily living (IADL),” suffers from a chronic illness and one other potential opportunities attribute of the number of living children (has adult living children) to model 3. Results indicate that older people with adult living children are significantly more likely to co-reside with kin. However, variables, “able to perform instrumental activities of daily living” and “suffers from a chronic illness” do not have any effect on older adults co-residing with kin. Many older people who live alone have kin living nearby with whom help is exchanged. However, the extent of the presence of nearby kin is likely to differ by place of residence, but this issue was not examined in this study. In Model 4, we included the resources variables. Socioeconomic status (SES) and education as measures of older people’s available resources show no effect. This finding is not surprising, because most of the older people in the sample owned their own dwellings (81.6%). It is arguable, therefore that these older people may choose to live alone or with spouse only. As noted earlier, also, it can be argued that they choose to live alone or with spouse only because their kin live nearby. Nonetheless, it would not be an overstatement to opine that as a result of culturaltraditions, older people often choose to live with other family members whether or not they own a home.Another interesting finding is that education did not have an effect on co-residence. Older people in the sample had none or very little education and thus we expected that they would be more likely to co-reside. Our hypothesis was not confirmed. Research has found that older people with high levels of education are significantly more likely to live alone or with spouse only than those without education (Bongaarts and Zimmer, 2002). The preceding analysis has supported the hypothesis regarding kin availability, which is found to be an important predictor of living arrangements of older people. Accordingly, we can conclude that kin availability defines the potential opportunities for co-residence for older people. The cultural factors defined by place of residence have no impact on older people’s choice of living arrangements. Nonetheless, a surprising and interesting finding was the significant negative relationship on older people’s living arrangement with a dominant proportion of children who are married. Older people who have a dominant proportion of children that are married are significantly less likely to co-reside. This contradicts the assumption that older people with a dominant proportion of children that are married would be more likely to co-reside with those children because of the implicit built-in support system. This finding emphasizes the complexity of living arrangements for older people in diverse societies. Table 3: Odds Ratios for Older People’s Living Arrangements (Living alone/with Spouse only Vs. Living with Kin), N=278
Statistically significant at *p<0.05 level; **p<0.01 level; ***p<0.001 level, and ‡p<0.10 level Reference categories of the independent variables are age group 60-64, male headed household, urban residence, 50% or less of living children are married, has no living children, not able to perform IADL, does not suffer from a chronic illness, has no adult living children, < 7 years of education, and owning neither land nor house. Discussion and Conclusion In this study, we focused on the living arrangements of Zimbabwean older people. We argued that it is important to analyze their living arrangements because it would help in identifying the existing structure of social support and the nature of family relations. The conceptual framework that guided the study incorporated elements of rational choice perspective in a model that explained several demographic, socioeconomic and cultural factors that influence living arrangements. Two hypotheses were supported. Kin availability increased older people’s likelihood of co-residence with other family members. In addition, older people with adult living children were significantly more likely to co-reside with kin. However, an interesting finding in this research was a new dimension to the challenges faced by older female-headed households. In later life, female older people are more likely to be living alone thus, less likely to receive help or support of any kind. Older women are more likely to need support than older men partly due to longevity and a history of poor nutrition and health care. They also need support more than men because of the difficulties they face earning an income because of the high rates of illiteracy among older women. The factors that make older women “useful” may also make it easier for kin to leave them to fend for themselves. Further, it may be that they cannot live with their married sons or daughters due to cultural norms or because they might not get along with their in-laws. Traditionally, very few older people of either sex lived alone, but for very different reasons. For men, it is difficult to become a widower because the occurrence of polygyny rises with age until late in life; hence, only 4.3% of older adult males reported being widowed whereas 36.3% of older adult females reported that they were widowed. In Cattell’s (1996) study on issues of personal and economic power among African women in regard to their marital situation, she found that 11% of older adult men were widowed compared to 49% of the women. In Kenya, it was 7% of men and 50% of women who were widows. This striking difference in rates of widowhood and the importance of marriage for women’s status and support illustrates the challenges for older women. It also indicates that although older men had lost their wives, these men may have remarried or may still be married to a second or third wife and hence did not consider themselves as widowers. Thus, older men are more likely to co-reside with other family members than older women. Nonetheless, a number of studies indicate that the majority of older people in developing countries live with their children, but very little is known about the reasons behind the decisions of older people and their children to live together. Cultural norms such as filial piety offer part of the explanation, but closely interwoven with these cultural preferences are the economic realities. Data in this study have highlighted a number of important characteristics of older people’s living arrangements in Zimbabwe that point to cultural influences rather than rational choice model. Most of Zimbabwean older people co-reside with other family members, especially adult children. The proportion of older people living alone with no subsequent person in the household is very small in both rural and urban areas (11.6% and 6.8%) respectively (data available upon request). Moreover, studies on developing countries (Chilungu, 1989; Cattell, 1990; Khasiani, 1987), and particularly on Zimbabwe (Hampson, 1982; 1985), suggest that older people’s living arrangements are determined by cultural norms that define family types. They note that living arrangements of older people are never a consequence of negotiations in which the older person evaluates his or her needs and resources to choose the most beneficial arrangement. Also, this study has highlighted a distinct feature of older people in Zimbabwe that contradicts earlier findings on the effect of economic status on living arrangements. Bongaarts and Zimmer (2002) note that older people with sufficient economic resources tend to live alone/with spouse only. However, in Zimbabwe data tend to suggest that economic resources have no influence on older people co-residing with children. In addition, rural and urban residences have no effect on the older people’s living arrangement. Although migration of young people from rural areas to urban areas may have altered the living arrangements of older people in the rural areas, the study shows that this had no effect on the living arrangements of both rural and urban older people. Furthermore, findings indicate that older people are less likely to live with their married children, but are more likely to live with their adult children. These factors have to be understood within the context of Zimbabwean cultural norms concerning living arrangements. As earlier indicated, older people may not live in the same household with their married children, especially their married sons, but they may live in the same homestead and hence the significant likelihood of co-residence with adult living children. The study shows the importance of demographic attributes of the children in decisions about living arrangements. The probability of living alone/with spouse only is less for those with living children. Thus, given the social changes happening in Zimbabwe, the proportion of older people living with adult children may decrease but those older people living with grandchildren will dramatically increase. Zimbabwe is witnessing a dramatic decline in its fertility rate, and, at the same time, witnessing very high mortality rates among economically active adults. Therefore, it is clear that in places where co-residence is a cultural ideal, the increase in older adults living alone is slow because older people will in fact live with grandchildren. Furthermore, in societies where mutual dependence is highly valued, it can be expected that even when demographic availability of children declines, the pattern of living arrangements of older people will not resemble that of the industrialized countries. In Zimbabwe and perhaps elsewhere in sub-Saharan Africa, older people who live alone or with spouse only do not do so by design, but for other reasons such as the unavailability of kin. Hopefully, the seemingly deep-rooted values about duty and obligation toward parents, or the emphasis on mutual dependence, will maintain patterns of living arrangements. This discussion reveals that the rational choice model, as it is currently developed, was not able to account for and capture the culturally specific factors affecting the living arrangements of Zimbabwean older people. Therefore, researchers should reexamine the rational choice model and work out a more comprehensive framework that is capable of incorporating cultural factors that influence the lives of older people. In addition, future research in sub-Saharan Africa could examine the gender imbalance in living arrangements and social support flow from older people to other kin. This should shed light on the potential value of aging populations in Africa. References
Copyright 2005 - Union for African Population Studies The following images related to this document are available:Photo images[ep05015f3.jpg] [ep05015f2.jpg] [ep05015f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}