 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Population Studies/Etude de la Population Africaine, Vol. 21, No. 1, 2006, pp. 19-36 A Minimum Data Set on Ageing and Older Persons in Sub-Saharan Africa: Process and Outcome Monica Ferreira1 , Paul Kowal2 1 Institute of Ageing in Africa, University of Cape Town, Faculty of Health
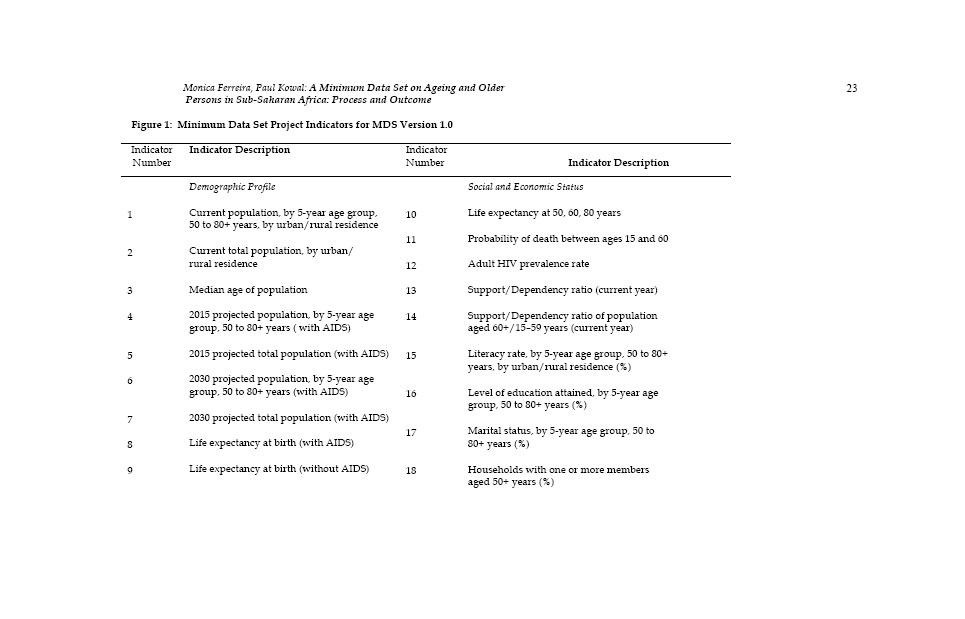
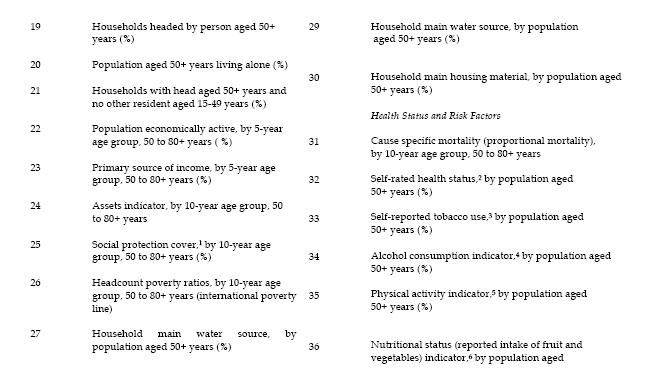
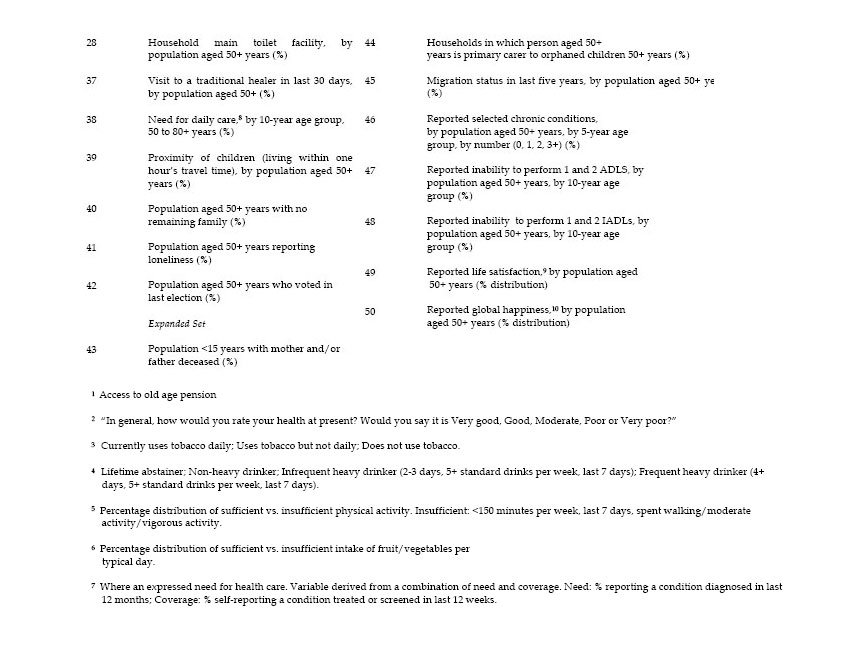
Sciences, Observatory 7925, South Africa Code Number: ep06002 Abstract Relatively scant knowledge is available on the situations of older persons in sub-Saharan Africa. Reliable and accessible demographic and health statistics are needed to inform policy making for the older population. The process and outcome of a project to create a minimum data set (MDS) on ageing and older persons to provide an evidence base to inform policy are described. The project was initiated by the World Health Organization and conducted in Ghana, South Africa, Tanzania and Zimbabwe. A set of indicators was established to constitute a sub-regional MDS, populated from data sources in the four countries; a national MDS was produced for each country. Major gaps and deficiencies were identified in the available data and difficulties were experienced in accessing data. Specific gaps, and constraints against the production and access of quality data in the sub-region are examined. The project and outcome are evaluated and lessons are drawn. Tasks for future phases of the project to complete and maintain the MDS are outlined. Key words: Sub-Saharan Africa, ageing, older persons, minimum data set, demographic and health indicators, policy Population ageing is a world-wide phenomenon. The world’s population aged 60 years and over1 is set to increase from 672 million in 2005, to 2 billion by 2050 (UNPD, 2003). At present, sixty-four per cent of older persons reside in developing countries; the percentage is projected to increase to 80 per cent by 2050 (USCB, 2003). Africa’s older population is expected to increase almost fourfold in that period: from 36.6 million to 141 million (United Nations, 2005). Constituting less than 5 per cent of the total population of sub-Saharan Africa (SSA) in 2005, the older population is projected to grow to 8.3 per cent by the middle of the century. In comparison, the older population of Europe is projected to increase from 20.7 to 34.5 per cent over the same period (UN, 2005). Although the pace of population ageing in Africa is slower than in other regions, increased longevity will result in growth in the absolute number of older persons. Average life expectancy at birth in SSA is projected to increase from about 45 years at present, to 63 years by 2050, resulting in an increase in the median age from 18 to 26 years (UNPD, 2003). However, the HIV/AIDS epidemics have greatly reduced life expectancy at birth in parts of Africa. In some countries – Botswana, Namibia, South Africa and Zimbabwe – HIV/AIDS mortality in the younger age groups may reduce life expectancy at birth by more than 30 years from otherwise expected levels (Kinsella & Phillips, 2005). Older persons in sub-Saharan Africa have particular vulnerabilities, which are exacerbated by social, economic, cultural, political and environmental factors. Poverty is widespread and the majority of countries lack formal social protection; older persons are consistently among the poorest of the poor. Natural and man-made disasters impact older persons’ livelihoods, security and well-being. Communicable disease is rampant – the direct and indirect consequences of the HIV/AIDS epidemics being most severe. Health systems must still grapple with the elimination of communicable diseases, and are unable to expend sufficient resources on treatment of an increasing prevalence of non-communicable diseases. Changes in family structures as a result of urbanisation and other forces diminish kin support for older persons (Ferreira, 2005a). Relatively scant knowledge exists on the situations of older persons in the sub-continent (Ferreira, 2005b; Velkoff & Kowal, 2003). Moreover, ageing related issues have a low priority in the policies and programmes of largely youthful societies. A lack of information relevant and specific to older persons’ physical, cognitive, social and economic well-being may contribute to their marginalisation in policy arena (Kinsella & Phillips, 2005). The exigencies of growing old and an inadequate knowledge base in the sub-region bolster a case for greater attention to be given to older persons. Although research on ageing and adult health has been conducted, or is ongoing in several SSA countries, studies have typically been small, piecemeal and unco-ordinated (Ferreira, 2005b; Velkoff & Kowal, 2003). Efforts to collect data have also been hampered by the unsuitability of Western standardised measurement instruments for use in African settings (Ferreira, 2005b). Data from large scale standardised national surveys, such as the Demographic and Health Survey (DHS), do not sample older persons (Kowal, Wolfson & Dowd, 2000). Reliable and accessible demographic and health statistics are needed to inform policy making for this population (Kowal, Dowd, Aboderin and Madzingira, 2002; Kowal et al., 2000). While an expanded knowledge base in the sub-region calls for a strengthened and integrated research endeavour, a concomitant need is for strong linkages to be developed between researchers and policy makers. To improve policy makers’ access to essential and quality data on the older population, a project to create a minimum data set (MDS) was launched by the World Health Organization in 1999. A minimum data set conceptualised for the project was a minimal priority set of indicators for policy and research, based on a common set of data items, definitions and standards, which should be used to collect and report information on the situation of older persons. The data should be comparable across countries within the sub-continent and over time (Kowal et al., 2000; WHO, 2000). The process to create an MDS and the project outcome are described. Aims of the Project The project aimed to establish a set of valid, relevant and timely data that describe the situations of older persons in sub-Saharan Africa. Data would be consolidated into an agreed set of indicators. An MDS should provide complete and reliable data on the health, social, economic, and physical and cognitive functional status of older persons for countries in the sub-region. It should be easy to use, update and disseminate, and could be used to monitor trends and progress in the health status and well-being of older persons. Specific project aims (see WHO, 2004, 2001, 2000) were:
An ultimate aim is for the MDS to be employed to inform policy and planning, and to guide new research sub-regionally. Country-specific minimum data sets should be developed and employed nationally and for cross-national comparisons. Thus might SSA countries contribute to and share in a contemporary knowledge base pertaining to the sub-region’s older population, and might African researchers represent and disseminate information on trends and issues of ageing in the sub-region globally. The Creation of the Minimum Data Set The MDS project was carried out collaboratively with partners in government, non-government and academic institutions in four African countries – Ghana, South Africa, Tanzania and Zimbabwe, in tandem with stakeholders and advisors in other regions (WHO, 2004, 2001; 2000; Kowal et al., 2000). Country representatives and stakeholders met initially in Harare, Zimbabwe (WHO, 2000), in 1999, to form working groups in the four countries, to review national data and metadata for suitability for inclusion in an MDS. Workshops were held subsequently in Dar-es-Salaam, Tanzania (WHO, 2001) in 2000 and Pretoria, South Africa (WHO, 2004) in 2003. Wide consultation and literature reviews were carried out in the interim to select indicators and to identify sources of data to populate the indicators. The development of the MDS was thus an interactive and iterative process of consideration and selection of indicators and identification of data sources by partners and stakeholders in multiple countries and regions, until a consensus was reached on what should constitute the MDS Version 1.0 (WHO, 2004, 2001, 2000). The Selection of Indicators The selection of indicators for inclusion in the MDS was based on a determination of key indicators that should inform policy makers about older persons’ situations. Numerous potential indicators were evaluated for their suitability to both assess needs and evaluate intervention, and meet stated criteria of being ethical, useful, scientifically robust, representative and accessible. Those indicators selected represented different ways of profiling the situations of older persons, from enumerating events, to describing the prevalence of characteristics in individuals, populations and institutions (Kowal et al., 2000). The finalised set of indicators comprises a core set and an expanded set (WHO, 2004), shown in Figure 1a, b and c. The core set indicators, a total of 42, are arranged according to Demographic Profile (# 1–18), Social and Economic Status (# 19–29) and Health Status and Risk Factors (# 30–42). An expanded set of eight indicators (# 43–50) is shown separately. Population of the Indicators A parallel process to the development of the sets of indicators was an identification of data sets from which data could be extracted to populate the indicators. Ancillary considerations were how data from various sources could be harmonised,2 or integrated, and what methods or tools were available to maximise the utility and extraction of information from the available data. An inventory was taken of all large data sets available in each country, including recent population censuses, national health statistics, nationally representative survey data (e.g. the Demographic and Health Surveys), localised studies and surveillance data. The quality and suitability of the data were determined in each case. Difficulties were experienced in gaining access to data, as well as the incompatibility of the format in which the data were available. These barriers were encountered for virtually all data sources and types, including vital statistics, population censuses, demographic and health surveys, hospital records, and other survey and study data, at both national and sub-national levels. A significant problem was the co-ordination of interaction with and access of data from the health information system of a country, which caused delays in the transfer of data. The identification of data sets and difficulties experienced are described for each country. · Ghana. Reliable data sources which could provide some of the data required identified by the Ghana working group were as follows: The population census (Ghana Statistical Service) (1970, 1984, 2000); the Ghana Demographic and Health Survey (DHS) (1993, 1998); the Core Welfare Indicator Questionnaire (CWIQ) (1997); and the Ghana Living Standards Surveys (GLSS-4, GLSS-5). Overall, data on the older Ghanaian population were found to be limited and appropriate data not always available. Neither the 2000 population census data nor the 2003 GLSS data were available at the time of compilation of data for the indicators in 2003. Data were often in an inaccessible or user-unfriendly format. Data sets did not easily allow for relevant age group analyses, e.g. by 5-year age groups, or 50 years and over. The transfer of data from the Ghana Statistical Service and the Births and Deaths Register was logistically problematic, in that it must be effected in person, and was hindered by distances, manpower shortages and delays involved. · South Africa. Compared to the other countries, South Africa was found to have a wealth of information sources from which data could be accessed. The main sources accessed, all which reside with Statistics South Africa, were the population census (1991, 1996; the 2001 census data were not available in 2003); vital registration data (1996–2000); the October Household Surveys (OHS) (1994–1999); the Labour Force Surveys (LFS) (1999–2002); the Income and Expenditure Survey (IES); and mid-year population estimates (1999–2001). Additional sources of information accessed were the Bureau of Market Research (BMR) annual surveys, which provide data for population projections and life expectancy; Medical Research Council (MRC) data on mortality and cause of death statistics; the National Department of Health (some statistics on HIV/AIDS); the National Department of Social Development (information on beneficiaries of the Older Person’s Grant); the Human Sciences Research Council (HSRC)(access to a wide variety of national opinion, and HIV/AIDS and older adult surveys); and the University of Cape Town (some information on the nutritional status of older adults). In general, once a data set was identified, access to the data was not problematic and data from different sources were largely comparable. However, some organisational departments and agencies where data sets reside were found to lack personnel to assist researchers to access the data. Numerous data sets must be purchased, e.g. from Statistics South Africa, which would be expected to be in the public domain. Some data are stored only in hardcopy, or in a format that is difficult to manipulate and requires specialised knowledge to access. In some cases clarification of indicators and indicator definitions was needed before data could be identified. · Tanzania. The Tanzanian National Bureau of Statistics (NBS) is a major source of data in that country, through a National Statistics Plan for official statistics. Previously, data collection in Tanzania mainland and Zanzibar was uncoordinated but is now co-ordinated by the NBS. The NBS is the main data warehousing agency in Tanzania, and establishes statistical standards and co-ordinates statistical activities in the country. Data sharing is encouraged. The NBS produces the Tanzania Socio-Economic Database (TSED), from which raw data may be accessed and tabulations made from input data sets, which include metadata. Data sources accessed by the Tanzania working group were the Population and Housing Census (1998, 2002); the Household Budget Survey (mainland) (2000/01); the Tanzania Reproductive and Health Survey (mainland) (2002); the Health Statistics Abstract (mainland) (2002); and the Integrated Labour Force Survey (2000/01). The 2002 census data were not available in 2003. No major problems were experienced in accessing and collating data, although data for some indicators could not be generated from existing data sources. · Zimbabwe. The Zimbabwe working group compiled data with the assistance of the Central Statistics Office. The main sources of information were the Ministry of Health and Child Welfare, and the Central Statistics Office. Data sources used were the population census (1992, 2002); the Poverty Assessment Study (1995); the Inter-Census Demographic Survey (CDS)(1997); the Demographic and Health Survey (DHS)(1999); and the Human Development Report (2001). Additional data sources accessed were vital registration statistics, and academic and NGO based research. Problems experienced by the Zimbabwe working group were as follows: Available data were often in an unusable format and incomplete. Access to data was often difficult due to the 2001 Official Secrecy Act. Although copious raw data are available, manpower is often unstable or lacking to analyse and manage the data. Limited data are available on the non-institutionalised population. Technology (software, the web) is needed to enable access to data. The population of indicators was undertaken by WHO and South Africa’s Human Sciences Research Council (HSRC), in co-operation with the working groups in the four countries. Data received from the countries were imported into a relational database and archived at the HSRC. All data remain the property of each country, but are in the public domain unless specified otherwise. Country working groups provided single point values for indicators in a spreadsheet or MS Access file format, rather than submitting values from different data sets or full data sets for a relevant indicator (WHO, 2004). Metadata were assessed for purposes of data comparability. Corresponding limitations of validity, reliability, comparability and completeness of the data are shown for each indicator in the case of each country. A spreadsheet of the MDS Version 1.0 indicators and separate listings of identified data sources for each indicator by country available at the time of compilation are extensive; due to space constraints the spreadsheet cannot be shown here. The matrix (MDS Version 1.0) is shown in full and may be consulted in the WHO final report (WHO, 2004). Data Gaps and Data Needs Major gaps3 and deficiencies were identified in the existing data and input data sets, and are reflected in the MDS Version 1.0. Numerous indicators in the country-specific minimum data sets could not be populated due to the non-availability, or unsuitability of the available data. Problems pertained mainly to the validity and comparability of data. Differences in definition and measurement (units and categories) largely limited comparability. For example, each country was found to have a different set of categories to describe marital status (WHO, 2004: 30). A specific data gap pertained to comparable health status and utilisation of health services. Accurate data on non-fatal health outcomes, e.g. morbidities and risk factors, remain difficult to obtain in all settings; the available data were neither comparable across countries. Data on health care service utilisation were similarly difficult to obtain. National mortality rates, and basic information on mortality risks and determinants in later life were lacking for most countries (WHO, 2004). Although numerous SSA countries have a legislated civil registration system in place (see e.g. Ghana, 1965; South Africa, 1992, 1997; Tanzania, n.d.; Zimbabwe, 1994), and some countries have good coverage of death registration, few have a system to collect cause of death details; the countries therefore mostly had poor coverage of death registration. Statistics on mortality provide primary inputs for the computation of summary measures of population health for local and national policy and planning purposes. Disease-specific rates can give useful feedback for monitoring health programmes, and identifying and prioritising health research activities and intervention. The data can provide a base for policy development, and the measurement and monitoring of the impact of policies. Because of the sparsity of older adult mortality data, SSA regional and national planners must depend on mode-based estimates of population, fertility and mortality. Empirical data used for these inputs are of variable quality and quantity, with resultant outputs only able to serve as benchmarks to guide policy and planning broadly (WHO, 2004). Routinely collected data were found to provide the most sustainable source of high quality data and to provide opportunities for comparison over a longer period. Statistics South Africa proved to be an exemplary agency in terms of routinely collected data provision and expansive data sets. In addition, the agency has access to sophisticated database and cross-tabulation software (e.g. Supercross) to optimise the extraction of data. Most data sets are stored in easy to use and accessible data set file formats (WHO, 2004). However, all country working groups experienced resource problems in assembling input data sets. National health information systems were found to need strengthening overall, but specifically their ability to provide valid and reliable routine data on mortality. Evaluation and Lessons The MDS Version 1.0 is evaluated briefly and lessons are drawn from the process to develop an MDS. An evaluation addresses both substantive and logistical issues. In general, a major need was identified for clarification andconsolidation of definitions of indicators. In the case of a number of indicators, appropriate, culture-specific assessment tools need to be developed and validated first, before reliable data can be produced to populate the indicators. Specific indicators in this regard are social protection coverage (indicator # 25 in Figure 1), literacy rate (# 15) and physical activity (# 34). Care is needed in both defining the indicator and selecting a method to collect the data, to ensure reliability and comparability. A number of logistical problems in assembling the data sets were experienced across the four countries. In general, agencies and departments had limited human resource capacity to assist researchers to obtain data. Inexorable time delays occurred between a request for data and release of the data. Data were not properly cleaned and analysed before release. Incompatible software and hardware often made data transfer a challenge. Some government departments lack access to the internet. Lessons learned in terms of how problems may be dealt with were as follows: Ideally, prior formal arrangements should be made and effective communication established with government agencies for access to data. Agreements should be entered, or work plans developed, to ensure that data can be provided on a regular and sustainable basis (WHO, 2004). Arrangements should be made with specialist researchers, or research organisations knowledgeable about data for various indicators, to source and extract data. Technical groups should be constituted to source data for a specific period, e.g. annually. The groups could work with agencies to produce data standards and formats in user-friendly, cross-tabulation software that allows improved ease of use and manipulation. The groups should develop a dissemination strategy, and identify colleagues to advise policy makers and planners in the use of the information. Yet other lessons drawn (WHO, 2004) were:
The WHO final report (2004: 29) outlines strategies to overcome some of the obstacles encountered in the process to create an MDS in a continuation phase of the project as follows:
Future Work The MDS Version 1.0 and the four country minimum data sets have the potential to provide comprehensive, up-to-date essential data to inform new policy development. However, the matrix is incomplete, and data gaps need to be filled and constraints to doing so overcome. Specific tasks that lie ahead are considered briefly. A primary task must be the identification and production of information to fill the data gaps. While suitable existing data may yet be identified, strategies are needed to produce new information for this purpose. To this end, primary data collection is already under way in two initiatives in SSA countries: The World Health Survey (WHS) (www.who.int/whs) and the Study on Global Ageing and Adult Health (SAGE) (www.who.int/sage). The WHS was conducted in 2002/03 in 70 countries in six WHO Regions, 18 of which are in sub-Saharan Africa. In three of the SSA countries – Ghana, South Africa and Zimbabwe – persons aged 50 years and over were over sampled (WHO, 2004) and the surveys will yield a rich dataset on the older population of these countries. Using the WHS as a baseline, the longitudinal Study on Global Ageing and Adult Health (SAGE), which focuses on older persons, will provide follow-up health and well-being data in a number of SSA countries, as well as methodologies to improve the measurement and assessment of health status and health care utilisation indicators. The SAGE programme will also make links with existing survey and surveillance activities in countries. Other tasks should include the design and implementation of strategies to strengthen primary data collections to measure adult mortality – specifically, vital registration systems, sample registration systems and survey methods. However, even where data collection systems are improved, a review of the data may be needed. Results of recent analyses of cause of death in South Africa have shown that ill-defined causes are more common in older persons than in other age groups (Bradshaw, Groenewald, Laubscher et al., 2003). Verbal autopsy methods can contribute to efforts to improve older adult mortality data – specifically, by obtaining basic information on causes of death and assessing the burden of diseases. However, the instruments need to be improved and methods developed for probabilistic cause assignment, in the place of currently used categorical algorithmic methods (WHO, 2004). In addition, indicators need to be reviewed. To serve their purpose, the indicators must represent priority issues of older persons and governments in a country, and must link with the country’s specific information needs and capacities. Not only do the quantities of interest and their relevant data sources need to identified clearly; methods for the estimation of indicators for the quantification of interests using standard definitions and analysis categories need to be developed and documented. An indicator review process thus needs to be started, which should include the setting of criteria for suitable data and standards for indicators. Major limitations in the extraction of data sets for the construction of cross-population comparable indicators will similarly need to be overcome. Values for single indicators within the MDS will need to be updated regularly. The maintenance and warehousing of the minimum data sets for medium term and longer term sustainability also require decisions. Decision making must pertain to infrastructural capacity and management costs of such maintenance and warehousing, as well as the accessibility of the data and how it will be updated. A strategy for the dissemination of information in the MDS will be critical to forging its employment and knowledge utilisation, both to guide future research and to support policy development. The WHO final report (2004: 31) outlines tasks to forge the dissemination of the MDS and the country-specific minimum data sets as follows:
Finally, the sub-Saharan African MDS indicators may in the future be employed in countries in other developing regions, in rapid appraisal of the situation of older persons in those regions and countries, to monitor changes and trends, and to measure the impact of policies and intervention, as well as for cross-regional and cross-national comparisons. The MDS therefore needs to be projected in global ageing arena, not only to disseminate information on ageing in Africa, but also to contribute to a global discourse on parameters of ageing and the profiles and situations of older persons in the developing world. Conclusions The process to create an MDS on ageing and older persons in SSA, constraints encountered and the project outcome have been described. Additional work is required to identify and generate data to populate indicators. A strengthened and integrated research endeavour in the sub-region, guided by the MDS indicators, will yield suitable data to fill gaps in the MDS and to maintain the national minimum data sets. A well populated and maintained MDS has a potential to serve as a valuable knowledge and information base to contribute to the advancement of research and policy development in the sub-region, through which the well-being and quality of life of older persons may be enhanced. Acknowledgement The contribution of numerous partners, stakeholders and consultants in multiple countries and workshops to the creation of an MDS on ageing and older persons in sub-Saharan Africa is acknowledged. Craig Schwabe in the Geographic Information Systems (GIS) Centre at the Human Sciences Research Council in Pretoria, South Africa combined data from the four countries to constitute the MDS Version 1.0. Opinions expressed in this paper are those of the authors and should not be attributed to other persons. The project was carried out under a grant from the Behavioral and Social Research Program of the United States’ National Institute on Aging through an Interagency Agreement with the World Health Organization. Notes
References
Copyright 2006 - Union for African Population Studies The following images related to this document are available:Photo images[ep06002f1.jpg] [ep06002f1d.jpg] [ep06002f1c.jpg] [ep06002f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}