 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
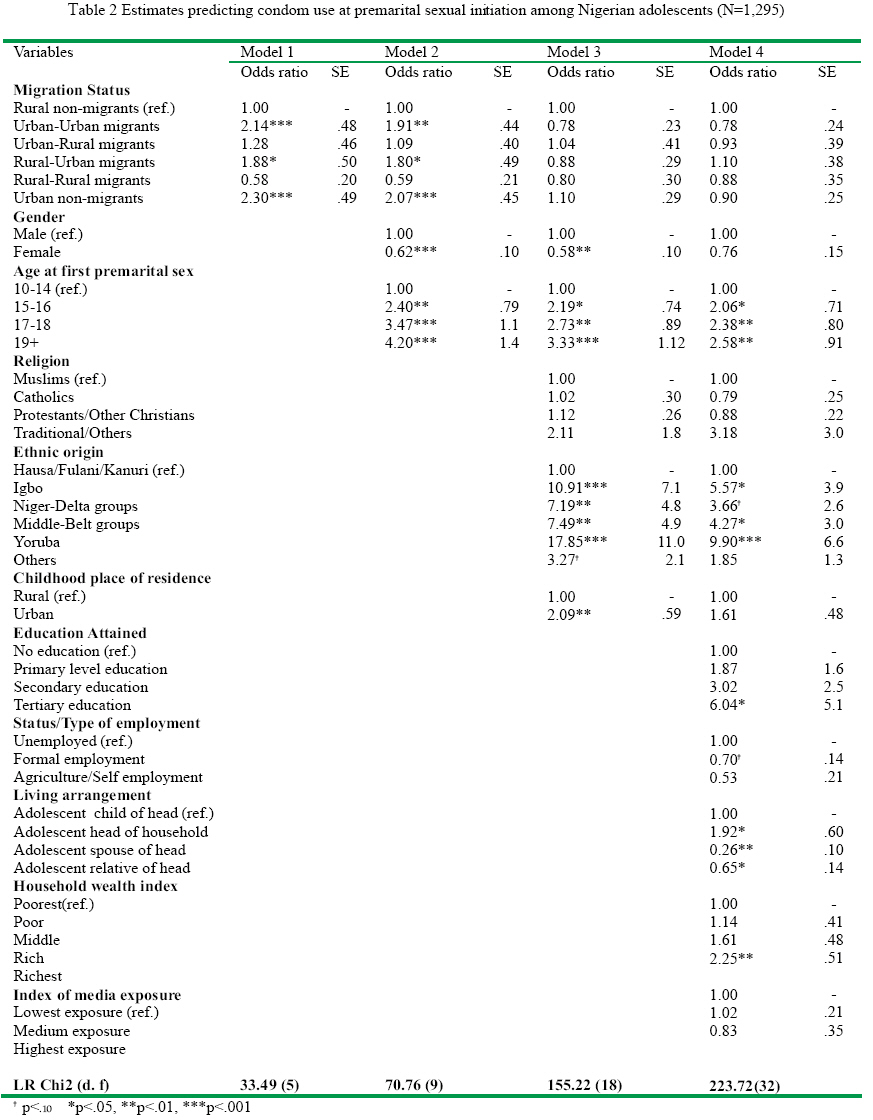
African Population Studies/Etude de la Population Africaine, Vol. 23, No. 1, 2008, pp. 57-83 Protection before the harm: The case of condom use at the onset of premarital sexual relationship among youths in Nigeria Blessing Uchenna Mberu African Population and Health Research Center, Nairobi, Kenya Code Number: ep08004 Abstract Condom protection has been linked to HIV decline, but the goal to prevent infections before any harm informs this focus on condom use at premarital sexual debut. The study builds on the proposition that condom use at first intercourse is an immediate indicator of the risks associated with the encounter and the propensity of subsequent condom use consistently and regularly. Data from the 2003 Nigeria Demographic and Health Survey and binary logistic regression models were utilized to examine the predictors of condom use at premarital sexual debut among Nigerian youths aged 15-24. The analysis identified significant independent effects of age at sexual debut, living arrangements, level of education, and household economic status, with the strongest effect linked to ethnic origin. The findings underscore the complexity of socio-cultural contexts that influence sexual behavior across groups within one country, and the importance of a multi-factor policy perspective for effective behavior interventions. Key Words: Condom use, Protective behavior, Premarital sexual debut, Youth, Nigeria. Introduction The study of protective behavior at the onset of sexual engagement among youths in Nigeria follows from the prognoses that the reproductive health of African youths yielded the worst indicators relative to other regions of the world (Okonofua, 2007). In many countries in the region, the onset of sexual encounter is premarital and this happens in the context of low levels of contraception and protective measures. The consequent debilitating outcomes (including sexually transmitted infections (STIs), HIV/AIDS, unwanted pregnancies, unsafe abortion, and high fertility rates among youths) underscores the enormity of the challenge in dealing with the consequences of youth sexuality in the region and the continued need for better understanding of the dynamics of young people's sexual engagement, in order to inform successful interventions. Following the renewed focus on young people's reproductive health engendered by the Millennium Development Goals, a corpus of new research in sub-Saharan Africa (SSA), have addressed protective behavior among youths. The consensus is that condom use is one of the most effective risk-reducing strategies available to young people who have initiated intercourse. Consistent and correct use of condoms was linked to 9095% prevention of HIV infections among sexually active youths. Part of the success of Abstain, Be Faithful and use Condom (ABC) program in HIV reduction in Uganda was linked to condom use (Singh et al. 2003). Evidence from the United States supports that along with the delay of sexual activity, contraceptive use plays a critical role in the declines in the birth rate for females aged 15-19 years from 61.8 births per 1,000 females in 1991 to 41.2 births per 1,000 females in 2004, a 33 percent decline (Hamilton et al. 2005; Santelli et al. 2006). While most of the studies are focused on knowledge, attitudes, correct and consistent use of condoms (e.g. Bankole et al. 2007; Guiella & Madise, 2007; Mahraj & Cleland, 2005; Adetunji & Meekers, 2001), particular attention on the timing of condom use by sexually active youths is lacking. The stage in young people's sexual engagement when condom is first introduced is critical not only for the outcome of each sexual encounter but also for the future trajectory of their behavior and reproductive health. Researchers have identified contraceptive use at first intercourse as an important indicator of not only the likelihood of an adverse outcome or otherwise of sexual debut but also the propensity to use contraception consistently and regularly thereafter (Abma and Mcgill, 2007; Shafii et al. 2004). Building on the premise of the foregoing, this paper focuses on condom use at premarital sexual initiation among Nigerian youth aged 15-24, seeking to identify significant predictors. Understanding key predictors of protective behavior at the onset of premarital sexual activities speaks directly to the goal of promoting protective reproductive behaviors before any reproductive health harm ever occurs. Background: Why Nigerian Youth and Protective Sexual Behavior? Nigeria's population of 140 million people is predominantly young: the estimated median age is17.4 years and about 63 percent are less than 25 years (Isiugo-Abanihe, 2003). Competing values around premarital sexuality pitches parental, family, and religious messages of immorality against those of powerful peer pressure and forces of modernization and globalization that equate sexuality with modern, educated, urbane lifestylesidentities for which significant number of young people yearn (Smith, 2000; 2003). While these views continue to engender discussions about social change and sexuality, the reality is that premarital sexual relationships are increasingly common in contemporary Nigeria. Youths in the country are increasingly linked to risky sexual behaviors such as casual sex and keeping of multiple partners, some of whom may include commercial sex workers (Isiugo-Abanihe, 2003; Arowujolu et al. 2002; Smith, 2000). Such behavior portends grave implications for reproductive health, and reports on the current situation in the country are hardly optimistic. The U.S. National Intelligence Council (2002) projected the next wave of the AIDS epidemic in Nigeria to grow to 15 million cases by 2010. The current HIV/AIDS prevalence rate is 5 per cent with about 3 million adults living with HIV/AIDS. Other estimates confirm rising rates of HIV prevalence in the country, from 1.8 per cent in 1992 to 3.8 per cent in 1994, 4.5 per cent in 1996, 5.4 per cent in 1999 and 5.8 per cent in 2001, with most of the new cases found among young people (Federal Ministry of Health, 2001). Other problems linked to young people's sexual activities in the country include unwanted pregnancies and unsafe clandestine abortions often by untrained or poorly trained providers (Aja-Nwachuku, 2004; Aziken et al. 2003; Bankole et al. 2006; NPC and ORC/MACRO, 2003; Otoide et al. 2001). The 2004 new national policy on population for sustainable development underscored the objective of effectively addressing the reproductive health needs of young Nigerians. However, the dearth of research and scientific evidence informing most reproductive health policies and programs has hampered similar policies in the past (Slap et al. 2003). Therefore, achieving the objectives of population policies, particularly as it concerns youths, requires an updated understanding of factors that influence young people's reproductive behaviors in the country. Relative to its population size in Africa, fewer studies are conducted in Nigeria, and most studies in the country are largely constrained by limited coverage. Some are based on data collected from youths in schools, leaving out nonschool youths, who are estimated to constitute over 60 percent of the youth population (Slap et al. 2003; Amazigo et al. 1997; Arowujolu et al. 2002). Other studies are limited to urban Nigeria leaving off the rural areas where an estimated 65% of the population lives (Smith, 2004; Makinwa-Adebusoye, 1992; Feyisetan & Pebley, 1989), and some are constrained by focus on ever-married women or unmarried female youths, entirely leaving out the male gender (Isiugo-Abainihe & Oyediran, 2004; Ajuwon et al. 2002). Such studies continue to overlook men in sexual and reproductive health initiatives, as well as the need to understand their needs, perceptions and motivations in reproductive health matters. The importance of studying men is premised on their considerable authority and power as decision makers in the home and society in the African patriarchal context (Isiugo-Abanihe, 2003). The focus on men is more so important following recent studies from a spectrum of developing countries including South Africa, Nigeria, and Cameroon suggesting the vulnerability of young men to some of the problems faced by young women such as sexual coercion, unwanted sexual touch, penetrative sex and being “rented” as prostitutes by older men and women (Ganju et al. 2004; Jejeebhoy & Bott, 2003; Ajuwon, 2003). Further, very little national level research on condom use is done in Nigeria and none simultaneously addressed condom use at premarital sexual debut for men and women. Also research that simultaneously compares Nigeria's heterogeneous ethnic groupings has received scant attention. Consequently we know very little about the genesis of adolescent protective reproductive behavior at the national level, as well as the social and behavioral mechanisms underlying them. This paper addresses these gaps using data from the 2003 nationally-representative Nigeria Demographic and Health Survey, with samples of school and non-school men and women, aged 15-24, from all the regions of the country including rural and urban areas. The study specifically identifies the predictive roles of individual, household and community factors in condom use at premarital sexual debut. Theoretical and Empirical Literature Review Studies in sexual risk behavior have identified three levels of theoretical and empirical influences: personal factors, the proximal context (interpersonal relationships and physical and organizational environment) and the distal context (culture and structural factors) (Eaton et al. 2003). Among the personal factors that may influence sexual risk behaviors include evaluations of vulnerability to a health risk, perceived severity of health outcome, the costs versus benefits associated with risk behavior, perceived emotional and social consequences of health-related behavior and perceptions about social norms (what other people think and feel and motivation to comply to such social pressures) (ibid). The influences of personal factors on sexual risk behavior are the key focus of a whole range of social psychological theories collectively dubbed the “social cognitive theories.” Notable among these theories are the Health Belief Model (Janz and Becker, 1984; Rosenstock et al. 1994) and the Social Cognitive Learning Theory (Bandura, 1991). Despite the validity of individual cognition models in Western societies where they have been largely applied, their key limitation is the scant attention to broader environmental and economic forces that may influence individual health-related behavior particularly protective sexual behavior. Moreover, evaluations of interventions based on the Health Belief Model for instance, have shown consistent disappointing effects on risky behavior, giving strength to the criticism that the individual is an inadequate unit of analysis (Auerbach et al. 1994). The need to transcend individual subjective characteristics and focus on objective proximal and distal factors in sexual risk behavior has been widely recognized in Africa. The proximal factors comprise interpersonal relationships, the physical and organizational environment. The distal factors are culture and structural factors. While cultural factors include traditions, the norms of the larger society, shared beliefs and values, and variations in such factors across subgroups and segments of the population, the structural factors are the legal, political, economic and organizational elements of a society (Eaton et al. 2003). Empirical literature on sub-Saharan, identifies correlates of protective behavior (condom use) at the onset of sexual activities among youths, that are consistent with the interaction of factors at individual, proximal and distal levels. Population migration has become a central theme in the discussion of the HIV/AIDS epidemic in sub-Saharan Africa. A growing body of studies, mostly in Eastern and Southern Africa, has recognized geographic mobility as one of the main facilitating conditions for HIV transmission (Lurie, 2004; Brockerhoff & Biddlecom, 1999; Fontanet & Piot, 1994; Hunt, 1989). In particular, massive migration of young, unmarried adults from presumably conservative rural environments to more sexually permissive African cities in recent years has been linked to the much higher AIDS seroprevalence levels observed in urban than rural areas (UN, 1994:8). The dynamics of transmission becomes more complex as frequent movements between cities, towns and the home villages remain the norm for many urban migrants in sub-Saharan Africa (Andersson, 2001; Geschiere and Gugler 1998; Gugler, 1971, 1991). The key role of migration is related to the notion of migrant selectivity. The consequent act of voluntary movement -often over long distances between radically different sociocultural environments and with uncertain consequences and social support networks at destinations - defines migrants, to a greater or lesser degree as innovators or risk-takers (Peterson, 1958; Massey et al. 1994). Further, econometric studies of migrant behavior routinely attribute differential outcomes to migrants and non-migrants' unobservable risk tendencies or characteristics (Moreno, 1994; Rosenzweig and Wolpin, 1988). Consequently, migrants may be predisposed towards heightened risktaking behavior including riskier sexual behavior than others in their new social settings, owing to personal traits established before migration (Brockerhoff and Biddlecom, 1999). However, what is not clear nor answered in literature is the extent to which migration of youths engender freedom of access to reproductive health services and the use of protective measures such as condoms. This study provides a unique opportunity to examine how migration status of young Nigerians relate to their condom use at the onset of sexual activities. Following an extensive review of literature, Abma and McGill (2007) linked socioeconomic status and characteristics of the family of origin to contraceptive use at first intercourse. Maternal education, the age at which a teen's mother had her first birth, family structure, race and ethnic origin have all been shown to affect the chances of teens' contraceptive use at first sex (Abma & Sonenstein, 2001; Bankole et al. 1999; Franzetta et al. 2006; Manning et al. 2000). However, Cooksey and colleagues (1996) examined changes in sexual debut and contraceptive use that occurred in the 1980's and concluded that not only did correlates of these behaviors change, but their effect changed across groups. Findings on the association of religious affiliation and religiosity with contraceptive use at first sex are mixed. Brewster et al. (1998) found that more strongly religious teens are less likely to use a method at first intercourse, but also found changes in the impact of religion across time. Similarly, an earlier study of adolescent males found fundamentalist affiliation to be associated with higher levels of sexual risk behavior (Ku et al. 1992). Conversely, others have found no association between religion and contraceptive use (Nonnemaker et al. 2003; Jones et al. 2005). In Africa, little knowledge exists on these relationships and researchers are only beginning to highlight the importance of religion in reproductive behavior of African youth. Smith (2004) underscored how the fervent Christianity of young migrants in eastern Nigeria created or at least solidified for some an important arena for individual sexual choices. Consequently, a significant percentage of born-again Christian youths in eastern Nigeria identified themselves as primary or secondary premarital sexual abstainers. A youth's age at first sex is associated with the likelihood of contraceptive use, although the relationship differs by gender. Older female youths are more likely to practice contraception at first sex (Manning et al. 2000; Abma et al. 2004; Abma & Sonenstein, 2001; Franzetta et al. 2006). Recent studies found older male youths more likely to use condom protection (Abma et al. 2004; Franzetta et al. 2006), but an earlier study found decreased likelihood of condom use (Ku et al. 1993). The important influence of the characteristics of the male partner and the nature of the relationship on young female's contraceptive use at first sex has been severally documented. The older the male partner relative to the female youth, the less likely is contraceptive use at first sex (Abma et al. 1998; Manlove et al. 2003; Manlove et al. 2005). This is linked to the fact that older males are less likely to use the condom (Ku, et al. 1993), and against the increased likelihood that sex among such partners may be unwanted or forced (Abma et al. 1998). These findings are corroborated by evidence that age asymmetry of sexual partners is related to transactional sex (Luke, 2003), a context not likely to enable younger female partners to negotiate safe sex particularly the use of condoms. Notwithstanding, there are no consensus on the effects of the nature of relationships on contraceptive use at first sex. Some studies find a lower likelihood of contraceptive use within more casual relationships, compared to more serious relationships (Lescano et al. 2006; Manning et al. 2000; Manlove et al. 2003) and other analyses have found the converse (Santelli et al. 1996). According to Okonkwo et al. (2005) the social environment plays an important role in the health-related behavior of young people, and this include friends and peers, sexual partners, family members as well as the community, school and other youthserving institutions ( see also WHO, 1999). The impact of peers on reproductive and sexual behavior of young people has particularly been strong (Diclemente, 1991; Ary et al. 1999; Staton et al. 2002). The belief of young people about the behavior of their peers is shown to influence their health behavior. Young people who believe that their peers were using condoms have been shown to be more likely to use condoms compared to those who had contrary belief (Diclemente, 1991; Staton et al. 2002; Diclemente, 1992). The social learning theory and the structural-environmental models are key theories that offer explanations on the role of social contexts in premarital reproductive behavior at the social and community levels (King, 1999). The structural-environmental theories of behavior change, which primarily posit that sexual behavior is a function of individual, social, structural and environmental factors also provide an appropriate framework for understanding the social context of adolescent reproductive behavior (see McLeroy et al. 1988; Sweat & Denison, 1995). A major limitation of most of the studies reviewed is that they were conducted in the United States, and the relevance of their findings for understanding premarital condom use in the African context is at best speculative. Again some of the findings are based on studies that focus primarily on female youths and their relevance for male youths are not obvious. Despite the lack of data to examine the role of all the factors identified in the review, this study represents a unique opportunity to identify and examine the independent effects of key variables on condom use at the onset of premarital intercourse in an African context. The study seeks to fill identified gaps by focusing on Nigerian male and female youths, using a nationally representative data set and covering the country's heterogeneous ethnic groups. Data The data used for the study is from the 2003 Nigeria Demographic and Health Survey (NDHS), an unbiased nationally representative sample of eligible respondents within all regular households in the entire country (NPC/MACRO, 2003). The survey interviewed 7,620 women aged 15-49 years and 2,346 men aged 15-59. From the male and female data files, 1,295 youths aged 15-24, who have initiated premarital intercourse and who have information on all relevant defined predictors were selected into this study. The survey used household questionnaires to obtain information on housing characteristics, living facilities and household composition. Individual questionnaires for men and women provided information on current and previous places of residence, duration of stay in current residence, respondent's age at sexual initiation, education, religion, ethnic origin, nature of employment, reproductive behavior and intentions, knowledge and use of contraception, marriage, etc. From the information gathered, variables relevant for this study were selected and defined: condom use at premarital sexual debut, individual and household characteristics, ethnic origin and other predictor variables. One key limitation of the data and by extension the study is evidence that sexual activity, particularly sex outside marriage, is normally underreported by women, more so by youths (Mensch et al. 2001; Adegbola and Babatola, 1999). Consequently, it is plausible that condom use at premarital sexual debut may be under-reported. However, since the goal of this study does not include establishing absolute levels of condom use and given that there is no basis to expect that underreporting, if it exists, varies systematically across settings, the study compares the relative occurrence of condom use at premarital sexual initiation across all youths as self-reported. Methods Definition of Variables The primary goal of this study is to determine the characteristics of youths aged 15-24 at the time the survey, who used condom at premarital sexual debut. The comparative group is youths of the same age bracket and characteristics who have also initiated premarital sexual activities but did not use condom in that encounter. The relevant question on condom use at first sex (the outcome variable) elicited a binary response category: Yes = 1, No = 0. To explore the multi-factor predictors of condom use at first premarital intercourse following literature reviewed and available data, the study examined individual characteristics of youths: migration status, age at first intercourse, gender, educational attainment, and religious affiliation. The 2003 NDHS has no direct questions on migration status of respondents. However there are questions on childhood place of residence before age 12, current place of residence, duration of stay in current residence and type of previous and current places of residence (rural or urban; city, town or countryside). Using responses to these questions (questions are available on request), including current age and age at first intercourse, migrant status at the time of sexual initiation were determined: Rural and Urban Non-migrants, Rural-Rural Migrants, Rural-Urban Migrants, Urban-Urban Migrants and Urban-Rural Migrants. Non-migrants are youths whose childhood place of residence remains their current place of residence. Migrants are those whose current places of residence are outside their places of childhood residence prior to the survey. The appropriate age variable examined is not the age at survey but age at first intercourse and this is recoded into four categories: 10-14, 15-16, 17-18 and 19 and above. Gender is coded 0 if male and 1 if female. The survey provides information on four levels of educational attainment: No education, primary education, secondary and higher education. The religious affiliation of respondents is recoded into four categories: Catholic, Protestant/Other Christians, Muslim and Traditional/Other. Catholics are separated from other Christian groups following the denomination's more traditional and conservative views on sexual behavior and contraceptive use. In examining the role of the nature/status of employment, youths were classified on the basis of the nature of independence from parental supervision, which each employment confers: formal employment, self/agricultural employment, and the unemployed. Youths in formal employment are most likely to be economically independent and spatially separated from parents and relatives when compared to others. Unemployed youths on the other hand, are most likely to depend on parents and relatives for sustenance, and therefore more likely to be close to their scrutiny. The association between household variables and condom use at premarital sexual debut is examined using living arrangements (household structure) and household socioeconomic status. The survey provided information on the relationship between youths and the head of household. Young people who are heads of households are perceived as having transited into independent living outside the authority and supervision of parents. They are compared to youths who are living under their parents as children, or with a relative or a spouse. In determining household economic status, the 2003 NDHS constructed wealth index and quintiles through principal components analysis of household possessions (see also Montgomery et al. 2000; Gwatkins et al. 2000; Filmer and Pritchett, 1999; Mberu, 2006; 2007), The role of community-level variables in predicting condom use at premarital sexual debut is examined through place of current residence (rural or urban), place of childhood residence before age 12, and ethnic origin. While place of current residence is provided in the survey as urban or rural, place of childhood residence is provided in four response categories: “Capital, large city”, “City”, “Town”, and “Countryside” . The countryside was defined as rural following other studies in the region, and the complementary categories were defined as urban. To deal with multicollinearity, current place of residence was not included in the multivariate models. The survey provided information on 112 ethnic groups in Nigeria. To assess variations in the use of condom at premarital sexual debut across these diverse cultural groups, they were classified into six major cultural categories, approximating the nation's geopolitical zones and following similar categorization by the Nigerian Institute for Social and Economic Research (1997). The three main groups (Hausa-Fulani/Kanuri, Yoruba and Igbo), represent the core North, South West and South East cultural regions respectively. The Minority tribes of Central Nigeria and those of the Niger Delta were respectively grouped into two cultural zones. Finally the myriad of groups that could not fit into these five clear categories were grouped together as others. The other control variable in the study is the index of media exposure. The survey asked whether respondents listen to radio every day, read newspaper and magazines once a week and watch television every week. Using the simple summation of frequency method, 1 for yes and 0 for no, I constructed three levels of exposure index to the mass media. Statistical methods and models This study employs univariate (frequency tables), bivariate (crosstabulations, Chi -Square tests of associations), Kaplan-Meier survival curves, and binary logistic multivariate regression techniques for the analyses of data. The binary logistic model developed for this purpose is written as: Log (Pi / (1- Pi) = â0 + â1X1 +â2X2 +â3X3 +â4X4…..+ âpXp + E1 where Pi is the probability of any of the defined event of interest for an individual i and 1 - P is the compliment. â0 is the base log odd of the reference categories of Xs and âj is the estimate of log odds of each outcome due to the net effect of a given category of the explanatory variables Xj. E is the error term associated with regression. All reported binary logistic regression models were estimated using the STATA statistical package. Condom use at premarital sexual initiation: Descriptive analysis Graph 1 shows the age at which youths in the study initiated premarital sexual intercourse ranging from age 10 to 24. Table 1 indicates that only 15.8 per cent of youths used condom at premarital sexual initiation. The table shows significant bivariate association between migration status and the use of condom at sexual debut. Both migrants to urban destinations from rural and urban areas and urban non-migrants indicate higher propensity for condom use at sexual initiation than rural destination migrants and rural non-migrants. These results are consistent with the principle that ruralurban migrants adapt to the new economic, social and cultural environment at the places of destination, resulting in changes in behavior. However, that migrants to rural destinations are less likely to use condom at sexual initiation suggests that the result may be speaking more to the role of urban areas in access to condoms than that of migration status. This is reinforced by the outcome that youths who lived in urban than rural areas before age12, indicate higher proportion of use of condoms at premarital sexual initiation than others. The proportion of youths who use condom at premarital first intercourse is lowest among those who initiated premarital sex in their earliest years. Conversely use is highest among those who initiated premarital sex after age 18, underscoring a strong age effect. Also higher proportion of males than females, Christians than Muslims used condom at premarital sexual initiation. The result shows large variation in condom use at premarital first intercourse among youths from different ethnic groups. The proportion ranges from 1.9% among the Hausa/Fulani/Kanuri; to 19.6 % among the Igbo; and 34.6% among the Yoruba. For time-variant covariates, higher levels of educational attainment are associated with increase in condom use at first premarital intercourse, with the highest proportion of use among those who attained tertiary education. Further, youths who live independent of their parents or relatives, those with more exposure to the media, and those from the richest households indicate higher condom use at premarital sexual initiation than others. The Chi-square (÷2) statistical tests of association between individual, household and community characteristics and condom use at premarital sexual debut mostly yield significant results. Apart from religious affiliation, which indicated no statistically significant association, all other independent variables examined in Table 1 are significantly associated with condom use at first sex. However, these outcomes are further refined in the subsequent multivariate models to account for bias that may be related to confounding variables. Condom use at premarital sexual initiation: Multivariate models I further estimate multivariate logistic regressions on the likelihood of condom use at first premarital sex and present the results in Table 2. Four binary logistic models are estimated. Models 1 through 3 successively include groups of time-invariant predictors, while Model 4 adds all the time-variant covariates (variables that are measured at the time of survey). As in the bivariate analysis, Model 1 confirms that urban-urban, rural-urban and urban non-migrants are strongly associated with condom use at premarital sexual initiation. In Model 2, with the introduction of time-invariant personal characteristics of youths, the advantage of urban resident migrant and non-migrant youths remain significant. In Model 3 however, with controls for ethnicity and place of childhood residence before age 12, the migration dummies became nonsignificant. The results suggest that unprotected premarital sexual debut is gendered. Female youths are 38% and 42% less likely to use condom at premarital sexual debut than male youths in Models 2 and 3 respectively. In the full Model 4 there remains a 24% female disadvantage in condom-protected premarital sexual debut relative to male youths, though the outcome is no longer statistically significant. This finding is consistent with the conclusion drawn from the four African country study referred to above (Ghana, Burkina Faso, Malawi and Uganda), which suggests that girls are likely to have first sex in circumstances outside their control or consent (APHRC, 2007). Under such circumstances, the ability to negotiate condom use seems remote. An interesting dimension of the result suggests that sexual initiation among young men is more likely to involve the use of condom and may therefore be safer. Consistent with findings in other settings, young Nigerians who initiated premarital sex in later years are more likely to do so using condom protection than those who initiated sex at younger ages. This outcome is consistent in all models, and in the full model (net all other effects), young people who initiated sex after age 18 are 2.6 times as likely as those who initiated sex before age 15 to use condom doing so. An intriguing aspect of the result is the significant variation in condom use at premarital sexual debut that exists between youths across different ethnic groups. In Model 3 the Igbo are 10.9 times and the Yoruba are 17.8 times as likely as the Hausa/Fulani/Kanuri to use condom at premarital first sex. Groups in the Niger-Delta are 7.2 times and those in the MiddleBelt are 7.5 times as likely to use condom at sexual debut as the reference group. While the strength of these estimates is reduced in the full model, the magnitude of the variations remains consistent and significant. Residence in an urban area before age 12 is a significant independent predictor of condom use at premarital sexual initiation. In Model 3, youths resident in an urban area before age 12 are 2.09 times as likely to use condom at premarital sexual initiation as those that reside in rural areas for the same period. In the full model, the direction of the association remained at 61% advantage for urban resident youths before age 12, though the estimate is no longer statistically significant. Among the time-variant covariates, education, living arrangement and household wealth status indicate significant association with use of condom at premarital sexual debut among Nigerian youths. As level of education increases, the magnitude of the association with condom use at premarital sexual initiation monotonically increases. In the full model, youths with tertiary education are 6.04 times as likely as those with no education to use condom at premarital sexual initiation . Youths who live independently are more likely to initiate premarital sex using condoms than those who live with their parents. Relative to youths living with their parents, those who initiated premarital sex but already living in unions at the time of the survey are 74% less likely to have used condom at premarital sexual debut. This outcome suggests that early union formation may be a strong indicator of unprotected premarital sexual vulnerability. Similarly, adolescents who live with relatives are also vulnerable to unprotected initiation of premarital intercourse without condoms. Finally, youths from richest households are 2.24 times as likely as those from poorest households to use condom at premarital sexual initiation. The estimates for households between the richest and the poorest categories fall within the continuum. Though the outcomes for these wealth status categories were not statistically significant, the estimates suggest a monotonic increase in the likelihood of condom use as the level of wealth status increases. Discussion and Conclusion The low level of condom use at premarital sexual initiation (15.8%) in Nigeria is comparable to low prevalence among youths in most countries of sub-Saharan Africa; for example 15% in Tanzania, Malawi, and Ethiopia (Zlidar et al. 2003; William et al. 1999); and 15.2% in Angola (Ndola et al. 2005). However, the prevalence rate is lower compared to Lesotho (34% for men and 59% for women), Uganda (43% for men), and Ghana (18% for men and 27% for women) (Tumwesigye et al. 2005). The result underscores the potentially high levels of vulnerability to sexually transmitted infections (STIs) and unintended pregnancy among young Nigerians at their first premarital sexual encounter. Against the backdrop of the proposition that contraceptive use at first intercourse predicts contraceptive use subsequently and consistently (Abma & Mcgill, 2007; Shafii et al. 2004), the result points to the enormity of challenge that must be surmounted in any effort at protecting the next generation of Nigerians from the consequences of unprotected premarital sexuality. The high level of use reported for Uganda linked to ABC campaigns, however, suggests the potential of focused campaigns to boost use (Finger, 1998). The result identifies urban-urban and rural-urban migrants, together with urban non-migrants, as more likely to use condoms at premarital sexual initiation relative to rural non-migrants. This outcome generally suggests a key role for present contact with the urban environment as a migrant or a nonmigrant. The explanation may be located in the role of the urban area in access to information and condom than in rural areas. It is important to note here that while rural-urban and urban-urban migrants are more likely to use condom at premarital sexual initiation relative to rural nonmigrants, these outcomes however, were no longer statistically significant in Model 3, which controls for the net effects of adolescent age at first sex, childhood place of residence and ethnic origin. The analysis finds a strong age effect consistent with literature on condom use. As the age at premarital sexual initiation increases, the propensity of condom use in the encounter increases as well. This outcome reiterates the increasing protective value of sexual initiation at an older age and gives quantitative evidence that empowering young people to abstain from and delay premarital sexual initiation, as a choice, can make a significant difference in promoting protective behavior from STIs, and enhances young people's chances of successful transition to adulthood in Nigeria. That protective condom use is highest among those who initiated sex after age 18, lends an empirical research support to international conventions that established 18 years as the legal age of consent to a sexual union. The association between gender and condom use at premarital sexual initiation is supported by recent findings in other African countries, and consistent with the explanation that young women are often unprepared for their first sexual encounters due to coercion, insistence of their often older partners, and powerlessness in transactional sexual encounters (Luke, 2003; Abdool Karim, 1998). Therefore, better quality policies and programs will need to address female disadvantages to access and use of protective services as condom. However, a more intriguing aspect of the result relates to the finding that young men in Nigeria are more likely to use condom at premarital sexual debut than young women. This outcome questions the notion that masculinity in Africa implies that young men have unprotected sex with numerous partners (Mac-Phail and Campbell, 2000), and challenges the justification that impulsive, unprotected sex is related to the male biology and desire (Eaton et al. 2003) . The significant role of urban place of childhood residence before age 12 is consistent with the adaptation principle of the social environment theories, and finds plausible explanation in the advantages offered by the urban environment for young people's access to knowledge and condoms relative to rural areas. This finding is reinforced by the observed strong ethnic effect on the likelihood of protective sexual behavior, which independently underscores the importance of socio-cultural context in shaping young people's sexual choices. The strong association between the Yoruba and condom use at premarital sexual initiation may be located in their high exposure to the urban environment as urban-urban and urban non-migrants (34. 6% and 35% of Yoruba youths in the sub-sample are urban-urban and urban non-migrants respectively). The same can also be said of the Igbo in a lesser dimension as ruralurban migrants. The strong independent ethnic effect observed finds support in the theoretical and empirical findings of the cultural diffusion theory, generally employed in explaining the demographic transition, particularly the acceptance of contraceptive innovation and fertility decline in Europe. Proximate areas with similar socioeconomic conditions but dissimilar cultures were identified to have entered the fertility transition period at different times, whereas areas differing at the level of socioeconomic development but with similar cultures entered the transition at similar times (Knodel & van de Walle, 1979). It is therefore instructive that this study located significant variation in condom use at first premarital sex among Nigerian youths within ethnic boundaries. These findings, consistent with findings in other parts of Africa, reiterate the suggestion that social and cultural contexts are primary determinants of sexual behavior of young people (APHRC, 2007). In Nigeria for instance, opposition to sex education and condom use campaigns vary along ethno-religious lines, underscoring the need for systematic intervention strategies for different groups. The findings that young people with higher education are more likely than those with no education to use condom at premarital sexual debut is as expected and continue to highlight the opportunities provided by higher education for promoting awareness, empowerment and the exercise of individual agency in the promotion of protective sexual practices. That youth from the richest backgrounds are more likely than those from the poorest households to use condom at premarital sexual initiation may be related to the cost of obtaining condoms. Researchers have strongly linked condom use in sub-Saharan Africa to access, and poverty constitutes a primary hindrance to accessibility (Campbell et al. 2007; ICASO, 2007; Ntozi et al. 2003; Klein, 2000). Finally, young people that live independent of parents and relatives are significantly more likely to use condom at sexual debut than otherwise. This finding advances more evidence of the hindering roles of parents and relatives in accessing and utilizing sexual-related information and services even when they are available. Sex remains part of the sacred norms in many African cultures and young people who live with their parents or relatives may be discouraged from accessing sex-related services such as condoms for fear of being identified as sexually promiscuous or being reprimanded if discovered. It is for similar reasons that health care providers are identified as unwelcoming to young people, consequently hindering them from seeking sexual and reproductive health information and services in the region. The key problem here is the inadequacy of parental door-keeping to successfully hinder premarital sexual engagement. The primary danger is the consequent thriving of clandestine and often unprotected premarital sexual activities with ominous implications. The outcome as it relates to youths living with relatives underscores the concern that the sexual behavior of such youths has rarely attracted focus, despite the high level of child fostering and apprenticeship prevalent in African societies generally (Isiugo-Abanihe, 1993; Chukwuezi, 2001). The key challenge here for both policy and programs, will be how to reconcile parental and relatives' control of adolescent sexual behavior, with the need to create opportunities for access to protective services for youths that need protection. There is also need to pursue policies that speak to the needs of young people under fosterage and apprenticeship. In conclusion, to the extent that selfreported condom use at sexual debut represents protective sexual behavior, this study quantifies the high-risk context that premarital sexual engagement entails among Nigerian youths. The adoption of protective behavior before any harm occurs to the reproductive health of Nigerian youths requires that policies and programs take into account the positive roles of delayed age at first sex until age 18; the roles of youth independence in their exercise of contraceptive choices; the role of the urban environment in enhancing access to knowledge and services, and the challenge posed for access to knowledge and services in rural Nigeria. Other important issues for consideration include the significant role of higher educational attainment and the hindering role of poverty in young people's demand for reproductive health services. Apart from deliberate supply of services, policies and programs can create demand through the economic empowerment of youths. Finally, the positive roles of some ethnic groups and the hindering role of others, highlights the complexity of social contexts that exist across groups in one country, and the importance of accounting for contextual nuances in the quest for policies and programs that will be effective for behavior change interventions. 1 The Millennium Development Goal Six seeks to reverse the spread of killer diseases, especially HIV/AIDS and malaria, diseasesthat have erasedagenerationof developmentgains (UNDP, 2002). 2 (See the Universal Declaration of Human Rights (1984); The Convention on the Elimination of All Forms of Discrimination against Women (1979); the convention on the Rights of the Child (1989); and the African Charter on the Rights and welfare of the Child (1990). References
© Copyright 2008 - Union for African Population Studies The following images related to this document are available:Photo images[ep08004g1.jpg] [ep08004t2.jpg] [ep08004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}