 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
The African Journal of Food and Nutritional Security Vol. 1, No. 1, 2001, pages 60 - 70 New R&D Papers HIV/AIDS, The Disease and Hunger Complications Causing Confusion in Rural Western Kenya: A Case Study of Katolo
Richard N.O. K'okul
The Department of Food, Nutrition and Dietetics Kenyatta University, P.O. Box 43844, Nairobi, Kenya Code Number: fn01007 ABSTRACT
The objective of this study was to find out whether it was HIV/AIDS or hunger pinning down patients at Katolo location in Nyando Division, Nyanza in Western Kenya. Was it hunger or HIV/AIDS influencing the low quality of life in the region? In a number of households visited, patients suspected to have been suffering from malnutrition marasmus, but alleged to be suffering from cultural chira or HIV/AIDS or unnamed ailments, were common. This forced the authors to refer patients observed with severe 'thinning ailment complications' to Katito Nursing Home, where they were tested using the Elisa method for HIV/AIDS. Out of the 91 households visited, nine patients were identified at the village level with severe thinning disorder alleged to be suffering from either chira, HIV/AIDS or as simply having complications from other chronic disease disorders. After the test, all turned out to be "HIV positive". Yet widespread ill-health caused by poverty, malnutrition, malaria and other chronic diseases in the region were evident. when the results were discussed with the health officer in-charge; he warned that tests based on the Elisa method can sometimes be unreliable. Consequently, people suffering from disorders other than HIV/AIDS are often pronounced HIV/AIDS positive without being confirmed using other tests, such as the Polymerase Chain Reaction (PCR) test. The PCR test is more reliable, because it is capable of looking at the viral DNA, which neither Western Blot nor Elisa methods can do.
Key Words: hunger, HIV/AIDS incidence, malnutrition, vitamin A deficiency, eye problems, chira, akuodi, child health, force-feeding
Introduction The paper will look at the HIV/AIDS complications currently causing confusion in a hunger study conducted in Katolo in rural Western Kenya. Out of the 91 households visited, nine patients were identified at the village level with a severe thinning disorder.
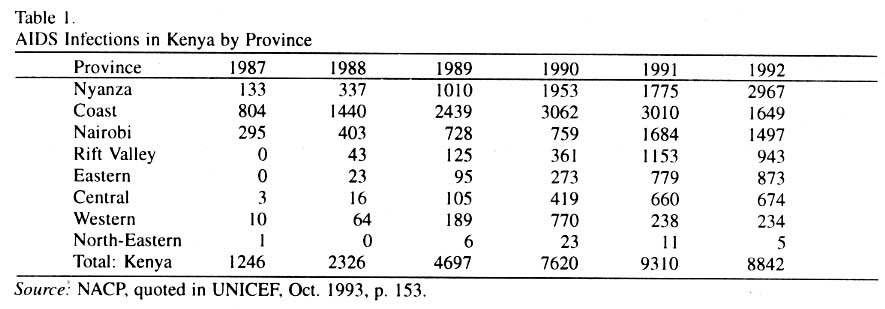
HIV/AIDS in Kenya The HIV/AIDS scourge has remained a dramatic occurrence since the first HIV case was reported in Kenya in 1984. there were only 109 HIV cases by 1986, HIV/AIDS occurrences have been increasing year after year and by 1987, there were 625 recorded cases; by 1990, 24,000 Kenyans had contracted AIDS and more than half of them had died. The number of AIDS cases has since the 1990s been doubling every nine months and by 1993, the National AIDS Control Programme (NACP) estimated that "between 750,000 to 1,000,000 Kenyans were HIV positive." An estimated 25,000 persons had been struck by HIV/AIDS by 1994, leaving behind 11,500 orphans, a figure which UNICEF predicted had reached 300,000 by 1998. In 1996, the World Health Organisation (WHO) estimated 1.5 million to be living with the HIV virus. Among the 1.5 million HIV positive cases, 650,000 persons were estimated to be with full-blown AIDS. Two out of every 18 persons in Kenya were said to be HIV positive and will die in the next few years. About 300,000 AIDS orphans below 15 years of age were either leading independent lifestyles as 'destitute', as orphan heads of households or were dependent on others for their upbringing. This figure was predicted to reach 1 million by the year 2002, thus raising child mortality by 75% over the next decade. The AIDS pandemic had managed to reduce life expectancy in Kenya from 59-52 years between 1989 and 1998. It was even alleged that, unless solutions were found, HIV/AIDS would reduce life expectancy in Kenya to 40 years, 20 years from now. Table 1 shows the year by year progression of the AIDS situation between 1987 and 1992. Since the early 1990s, Nyanza, Coast and Nairobi provinces have been leading in AIDS cases. The Arabic-Muslim North-Eastern province remained least affected; while variations occurred between urban and rural areas, with HIV positively found in 10-11% of urban adults and in 4.5% of rural adults (UNICEF, Oct. 1993:153). At least four people are buried daily per administrative division in Nyanza from AIDS deaths alone, while 500 people are said to be affected daily. The AIDS pandemic does not only affect the sexually active population. It also affects children, youth, men and women, including those pregnant and lactating. The HIV/AIDS scourge is rather severe among teachers; about 3,000 teachers die annually from AIDS in Nyanza alone. Conservative estimates depicted that close to 600,000 people in Nyanza would be. HIV/AIDS sufferers by the year 2002. It currently harbours close to 30,000 AIDS orphans. Kisumu and Nyando Districts have higher AIDS endemicity, compared to the other districts in Nyanza. Nyando District is leading in HIV/AIDS, with the division such as Katolo, the worst affected. Out of every 10 households visited at random in Luo Nyanza, 3-4 households have an HIV/AIDS widow or an AIDS orphan.
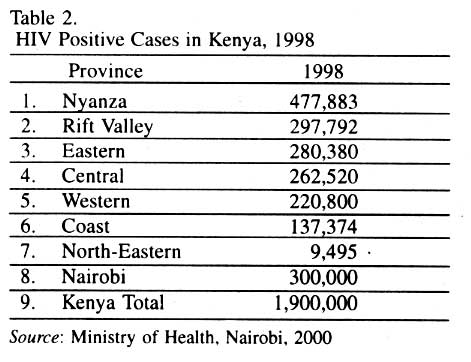
About 2 million people were estimated to be HIV positive in Kenya by the year 2002, while close to 10,000 had full-blown AIDS. In Nyando, HIV/AIDS has reduced life expectancy from 48-40 years between 1988 and 1998. Unless solutions are found, if the HIV/AIDS infection rate continues in the present trend, life expectancy in Kenya will generally be reduced to 40 years, 20 years from now. Today, attitudes, behaviour, habits, adhering to customary norms and certain habits applied in medical practice, remain promotive agents. Coupled with worsening poverty, food insecurity and malnutrition, AIDS sufferers are always on the verge of death (Table 2).
HIV/AIDS Theoretical Perspectives
Efforts to isolate the virus HIV causing AIDS was first done by scientists led by Dr. Robert Gallo at the National Cancer Institute in the USA from homosexuals suffering from human T-cell lymphadenopathy associated virus Type III (HTLV) in 1981. At first, doctors thought it was Kaposi sarcoma. Efforts to isolate the HIV virus continued with serious case definitions and surveillance in the USA throughout 1982. The virus that causes AIDS was finally isolated in 1983 after French scientists at the Pasteur Institute, in Paris led by Dr. Luc Montagnier, had identified from a criminal patient with enlarged lymph nodes who had fled from a California prison in the US, what he called human lymphadenopathy associated virus (LAV). His vision about HIV/AIDS was that:
Like herpes, HIV is a virus. Like syphilis, HIV affects the whole body and can take [a] few or many years before it causes serious damage or kills... and for HIV infection to occur, its virus has to enter the bloodstream. In the bloodstream, HIV attacks the immune system. The immune system is thus what protects the body against disease, producing various cells in the blood to fight it. Among these are T4 cells, whose role is to identify the intruder and to authorize other cells to produce antibodies to kill it. If HIV gets into the bloodstream, it enters and lives inside T4 cells. It replacates by changing the genetic structure of a T4 cell and making it into a virus factory. It is the immune system that is prevented from functioning. Our immune system is therefore our bodyguard. It accompanies us everywhere we go. It defends us so alertly and silently that we are not aware of the thousands of enemy attacks mounted against us by microbes (germs) everyday. If our immune system falters, maybe because of disease or undernutrition or combined effects of both, we become vulnerable to further disease-causing agents and infectious diseases will invariably follow. our immune system of all the body systems, responds most sensitively to subtle changes in nutritional status. The immune system is measured by testing the number of T4 cells (also called CD4+ Lymphocytes) in the blood and is considered to be at an advanced stage of impairment when this count goes below 200 per cubic millimeters of blood.
Thus, by the time the test for detecting antibodies was being developed in 1985, AIDS had engulfed a great deal of the entire world. it had become established in the US, Haiti, France, Holland, Switzerland, Zaire, Angola, Tanzania, Uganda, and Kenya:
The earliest cases of people who died from HIV/AIDS were identified between 1981 and 1983 from stored samples of tissue and fluids related patients had a syndrome (i.e., a group of symptoms or illnesses), with reduced immune system function and one or more serious illnesses. Their health was also characterized by severe loss of weight, abnormally slow growth, chronic diarrhoea for more than one month, prolonged fever for more than one month, generalized lymphadenopathy (i.e., Lymph node enlargement), oro-pharyngeal candida and repeated common infections with other disorders, including complications sometimes with cough and tuberculosis.
No one knew at that time how HIV evolved into its present form, neither was it understood the reasons why these people had become ill and died (Berber and Ray, 1983: 5-9). The same ignorance continued into the mid-1990s, despite the efforts to find AIDS cures. This is part of the reason why no reliable AIDS cure has been found to date. AIDS had become established as a major world disorder by the mid-1980s. The virus was renamed "Human Immune Deficiency Virus" (HIV) in Eastern and Central Africa and/or HIV-2 in West Africa. Between 1983 and 1986, three paradoxical theories were advanced to explain how HIV/AIDS developed into its present form: 1. The Green Monkey HIV Virus Theory This theory was developed by a British virologist, Dr. Max Essex of the Harvard School of Public Health, in collaboration with the scientists from the University of Kinshasa. They argued that, "the HIV virus germ was of Africa's green monkey origin and inferred that there is one type of green monkey with HIV virus that the Africans eat" and that, "when the meat of that green monkey is eaten, AIDS is transferred into the human's blood stream through diffusion after digestion". 2. The Mosquito HIV Virus Germ Theory Two French scientists advanced another theory - 'the Mosquito HIV Virus Germ Theory' and argued that, "the HIV virus germ is transmitted by the African mosquito". This theory was developed after a Kagera region study near the shores of Lake Victoria, in which the two researchers reasoned that: Because green monkeys share acommon environment with the mosquito and the Africans, the mosquito will bite the infected green monkey and then go and bite the human being and transmit the HIV virus germ". 3. Promiscuity HIV Virus Transmission Theory this theory is the leading theory to date. It argues that HIV is transmitted by sexual contact. It was derived after the famous Majengo-Pumwani prostitutes study in which promiscuity was inferred to be the main mode of HIV transmission. The study was led by Danish researchers from Panos Institute. it argues that: Africans by nature are "sexually active". and that "during copulation when both... are stimulated, the HIV virus will easily diffuse from the bloodstream into either ovary or sperm duct from where the virus is released through ejaculation". Transmission is severe in patients with wounds and the possibility of blood contamination. The Danish researchers warned that, "unless the race changes their promiscuous habit, the African race is heading towards extinction."
Methods and Materials
From August to October 1995 a food security study, the Eleven Katolo Villages Food Security Survey (EKVFS) was undertaken in Nyando Division. However, HIV/AIDS which was complicating the study by causing confusion as to whether it was hunger or HIV/AIDS influencing the prevailing low quality of life. In a number of households, the study confronted patients suspected to have been suffering from malnutrition marasmus, but they were told that they were suffering from cultural "chira", HIV/AIDS or some unnamed ailment. It was therefore necessary to refer related patients observed with severe "thinning ailment complications", to nearby Katito Nursing Home, where they were tested for HIV/AIDS using the Elisa Method. Out of the 91 households visited, nine patients were identified at the village level with severe thinning disorder and all turned out to be HIV positive. Results
State of Maternal and Child Health
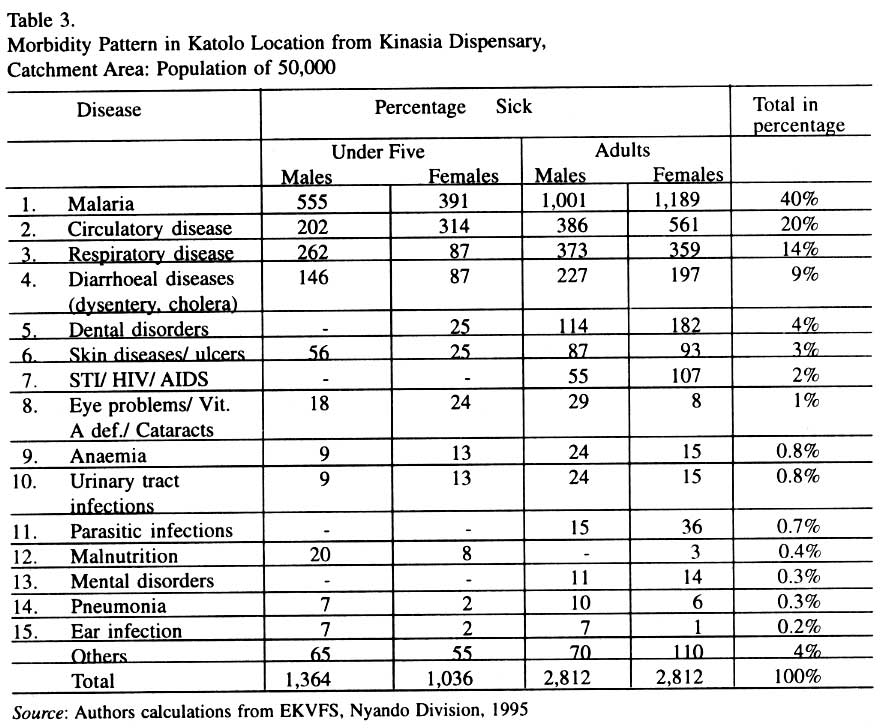
Table 3 shows the state of health at the community level in Katolo Location.
It is clear that the most prevalent disease in the region was malaria, while malnutrition ranked 12th. Other disorders of significance were diarrhoeal diseases, eye infections, anaemia and sexually transmitted infections.
Health status of lactating and pregnant mothers in Katolo Location
Pregnant mothers presented a more special problem. A number of mothers complained of nyasach mon or rariw (pelvis inflamatory disease, PID) and sigeta (maternal severe stomach-ache after sex and during the menstruation period). The causes of these disorders were not clear. Katolo mothers' weight gain during pregnancy studied in 1991-1994 was between 5 and 7 kg, in contrast to the standard 12.5 kg expected for well-nourished mothers. Most deliveries were at home, under the care of traditional birth attendants, since the area lacks a formal delivery system. Because of the general poverty, the majority of the mothers lactated under poor conditions and inadequate nutrition.
Pre-school child health in the household (6 - 36 mos. of age)
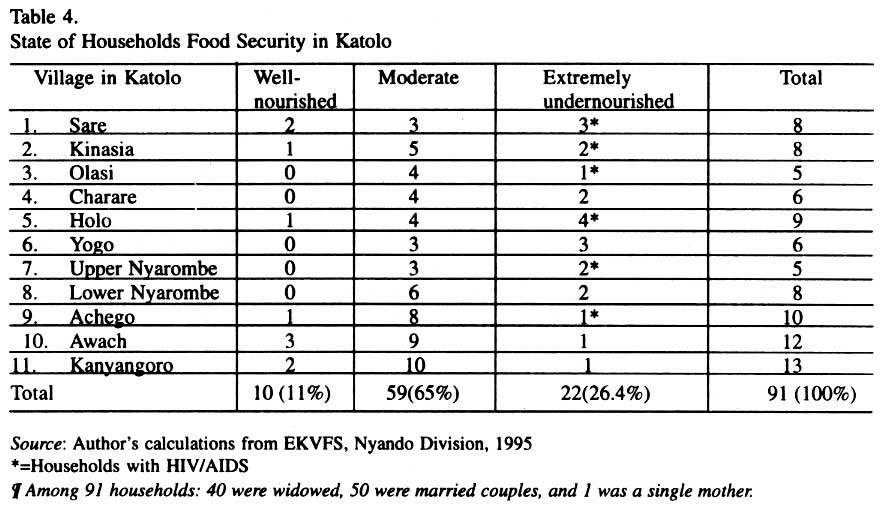
The outcome of the Eleven Katolo Villages Food Security Survey (EKVFS) showed that of the 91 (100%) households visited, food insecurity and hunger was a major problem (Table 4).
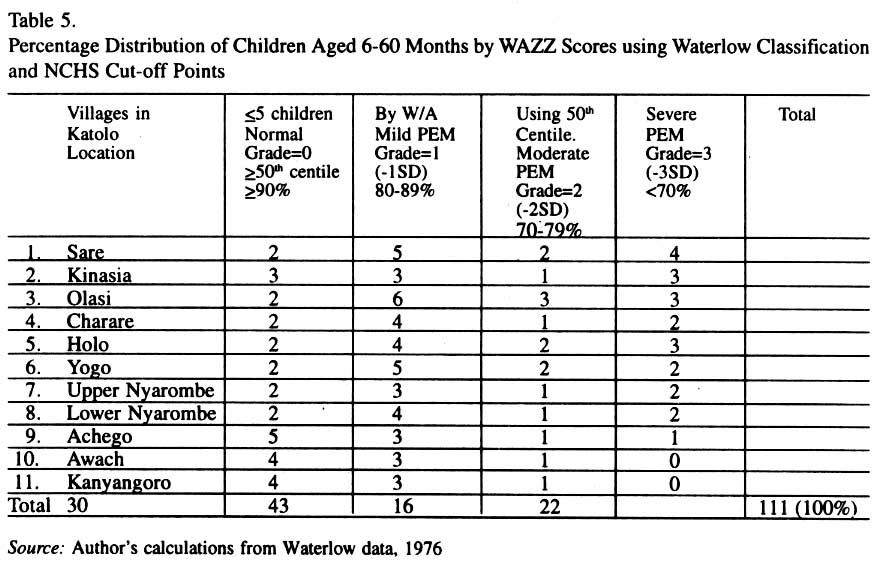
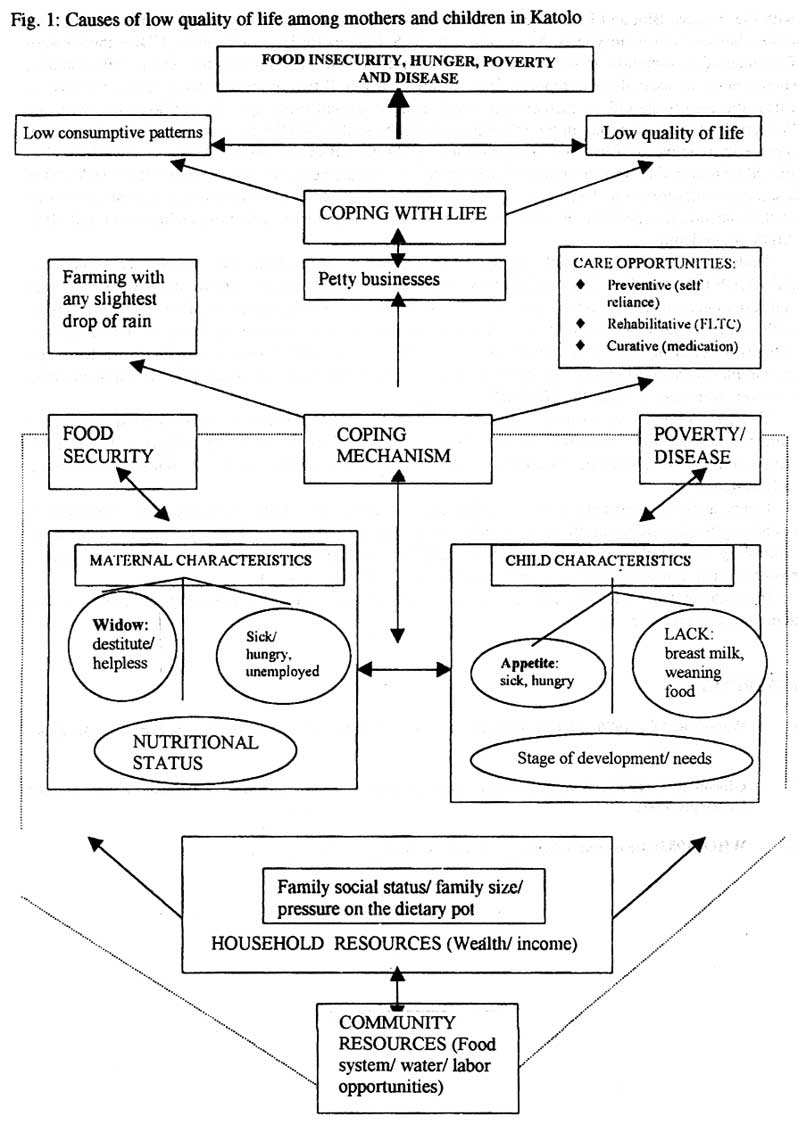
A low quality of life was evident among mothers and children, 22 (26.4%) of the households were extremely undernourished (among whom nine had members reported with HIV/AIDS), 59 (65%) were moderate and 10 (11%) were well-nourished. Nutritional status of pre-school children from the Katolo Village households were calculated using Waterlow's PEM classification1-2 and the NCHS 50th Centiles of Katolo Children W/A indices.3 The conventional Waterlow classification adapted from Gomez grades PEM using WAZ is shown below (Table 5). Out of the 111 pre-scholars examined for ill-health and malnutrition, Katolo children were surprisingly found to depict a growth pattern resembling those of American children using the U.S. National Center for Health Statistics (USA-NCHS) standards. Their growth and development appeared to present a relatively important problem for both sexes, regardless of the household welfare ratio: 30 pre-school children were above the 50th percentile of the NCHS standard, 81were less than the 50th percentile and had weights faltering between the 3rd and 50th percentile. Only 22 children had a growth rate below the 3rd percentile, among whom 10 children were below 12 months, 11 children were between 13 - 24 months and 1 child > 24 months. Out of the 22 children below the 3rd percentile, 18 had severe malnutrition and only 4 were healthy. Malnutrition, vitamin A deficiency and anaemia cases varied from mild to severe. Most pre-scholars falling between the 3rd and 50th percentiles were often suffering from latent hunger. Most malnourished children were from extremely undernourished households, dominated largely by widowed mothers. This latter group deserves most attention: over half of the widowed households tended to have more nutritional disorders than the general population (Fig. 1). Five pre-schoolers were detected with positive adiposity cases, one of whom was from a widowed household and was apparently extremely undernourished. From this, it was deduced that: some children will just grow well, even in the face of a poor diet. Cultural "force-feeding" was commonly practiced, where a child was placed on its back, held between the caretaker's thighs and fed-forcibly with porridge clenched in the left hand while blocking the child's nose with the right-hand fingers. This was suspected to be the underlying factor contributing to the development of an abnormally large percentage of adipocytes among Katolo children in early childhood. Anaemia nutriture was a problem among the general population.
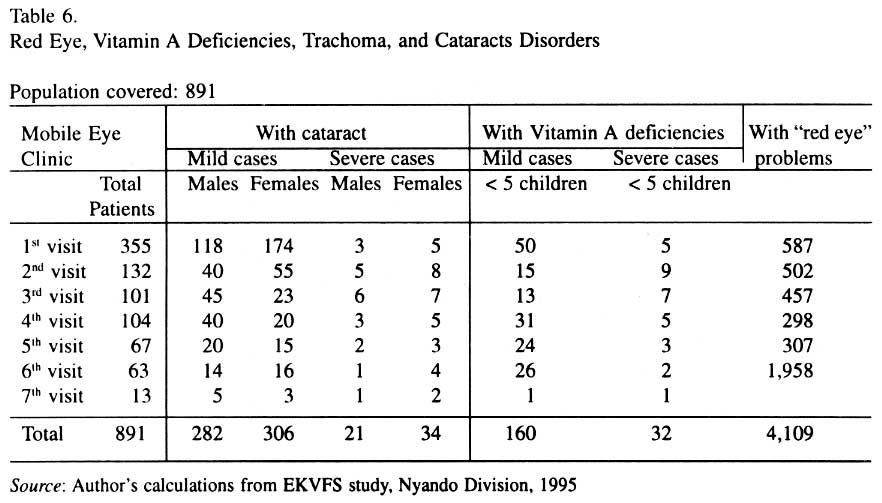
Eye problems and associated disorders in Katolo
Problems of "red eye" (episcleritis, keratitis, herpes simplex, iritis,
glaucoma, ophthalmia neonatorum), vitamin A disorders (keratomalacia), tracoma,
and cataract were shown to be severe. This was reflected in both clinical data
and Mobile Eye Clinic data. Table 6 shows
cases of "red eye", vitamin A deficiencies, trachoma and cataract
that were detected during the Mobile Eye Clinic held in Katolo.
During the community diagnostic work, the authors encountered nine AIDS cases. One case died two days later when transferred to Katito Nursing Home for the Elisa test. Two cases, both males, later died in Sare village as the research process was going on. The remaining six cases died one by one over the course of time, the last of whom died in Sare village in January 2000.
History of HIV/AIDS in Katolo
The first HIV/AIDS case in Katolo was reported in 1989 from a "migrant labourer" then working in Naivasha. He transported it into the village, infected his wife and the entire family died. The next twelve AIDS cases were among migrant labourers. One contracted it in Eldoret and later died in the village; the wife is still alive. The thirteenth AIDS case contracted the disease in Kisumu town, infected his wife and the entire family died. The fourteenth case and five others contracted AIDS at Katito market. They died one after the other. Two females contracted AIDS in Muhoroni township. Both later died in the village. There were several cases of "run-away" wives who respectively contracted AIDS in various places in Luoland, came back, died in the villages and thereafter were followed by their husbands one by one. Today, there is an AIDS death case every third month. As our research was ongoing in the villages, we came across a pathetic HIV/AIDS-chira patient in Achego village, Katolo. The following narrative describes his condition:
Encounter with a Pathetic HIV/AIDS-Chira Patient in Achego Village, Katolo
In front of us lay a patient clumped in a ragged blanket. He was counting his last days on earth. As we came face-to-face with the patient, we asked: "What is his problem?" A neighbourhood girl who had taken us there, whispered: "Don't ask. He is down with Aede" (HIV/AIDS). As we stupifiedly stood watching, we witnessed that the man was severely suffering from an uneasy sensation in his stomach and craving for food, which was apparently not there. We could not stand the sight. AIDS had combined with food, insecurity, poverty and hunger. Apparently, he was not only all bones but too weak, a condition brought about by acute starvation. Hunger had been with this man in walking, in sleep, in his dreams, awake and in sickness. As we kept standing, sorrowfully staring at the sight of a dying body, his bowels kept crying out insistently for food. There was a gnawing pain with rumbling stomach, as if his very vitals were as well being devoured, of course, it was hunger. He wanted to stop it at all costs, for in many instances he looked at us with food-begging eyes as if he would buy a moment's respite. Knowing that even if we were to give him food, he would still die for it was HIV/AIDS pinning him down, we just sorrowfully kept staring at each other like two clever debtors, as the man waited for his death hour. Then the pain was no longer sharp but dull, which gave him a signal of relief. It was at this sort of moment that he thought of food, crying out many times for food assistance, but each time he cried out, the terrible pain again assailed him. He knew that even if he were to be given food, he would not eat because of the powerless throat; he tried to avoid the thought and only kept staring at us with sunken eyes, complaining of ear pain. He wriggled everywhere on the mat on which he lay in hunger-and-"Aede" pains, crying for help until only a great emptiness was left in him, like the sky, like a well in drought. Suddenly, a sign of strength began to drain into his limbs and he struggled to rise up in order to find even water to drink, trying several times to swallow saliva but the throat was powerless. Oh God! He was all bones. Beside him, sat his emaciated wife nursing him in his last days and at the same time, feeding a three-year old kwashiorkor-devastated child on plain red sorghum porridge, without any additive. In this household, sugar was a forgotten thing. This family owned nothing except the mat, the blanket in which the AIDS-ridden person was wrapped, two cooking pots and a calabash. Their house was a hovel. Poverty was too much in the forefront and this destitute family relied on nothing but charity foods. Disgusted to death, I reached into my pocket, pulled out all the money I had, pushed it into the HIV/AIDS-ridden patient's strongly clenched hands and walked away
From the health centre data, malnutrition ranked 12th in terms of causes of mortality, while all sexually transmitted infections (STIs, including HIV/AIDS), ranked 7th, however, because of the difficulty surrounding the distinction between cultural chira (marasmus) and HIV/AIDS, differentiating among the three was not easy. What are these conditions so prevalent in Katolo villages: chira (marasmus), akuodi (kwashiorkor) and akuot ledho (kwashio-marasmus)? Chira is different from malnutritional marasmus in that: marasmus results from acute, degrading starvation and thinning because of the absence of food. Chira, like marasmus, results in severe thinning but chira is thought of as culturally specific, that it comes about because of breaking a taboo. In the Luo society, there are certain customary norms (kweche) which are expected to be strictly obeyed. These include those associated with seasonal seed planting (golo kothmahiga), seasonal ploughing (golo pur), seasonal harvesting (chako keyo), and seasonal eating (chamo mahiga). Most of these are traditionally ritualized. Further, a daughter who had reached menstruation stage was expected to behave decently and not to have sex with a man in her mothers' household. If this happened, it would result in chira. Chicken was not supposed to be eaten by women, neither were eggs eaten by children, nor kidney eaten by men. Modern religious persons eat everything, and discard such traditional habits as old fashioned (timbe achona).
What then, is malnutritional akuodi? Akuodi is different from chira in that it is a severe underweight disease accompanied with edema believed to be caused in either of the following ways:
it was not easy in the field to differentiate among HIV, chira and akuodi cases, because of these symptomatic diagnostic complications. Taking all this in consideration, we were told that during 1989-1995 alone, "HIV/AIDS complex" managed to close nearly 500 village gates in Katolo. When the people were asked the causes of HIV/AIDS in Katolo, they answered that this is a foreign disease and that its mode of distribution was through: "mosquitoes, promiscous sex, blood transfusions, second-hand clothing, and toothbrush sharing. One village elder asserted that the problem is hunger and that if one was to carefully test all those currently suffering from alleged AIDS in his community, deny them drugs for a period and instead nutritionally rehabilitate them, they would all recover. He critically questioned the authenticity of HIV/AIDS screening tools currently used.
In summary, the cause of thinning disorder in this community is hunger, not HIV/AIDS or chira. The majority of Katolo people are starving to death and it is hunger and degrading starvation which is killing people in this community, particularly during drought.
DISCUSSION
This paper has raised certain critical issues that need to be given serious consideration in HIV/AIDS studies in Nyanza today. One clear observation is that, in societies where malnutrition, malaria, tuberculosis, and leprosy are severe, better diagnostic tests for HIV/AIDS are required beyond the Elisa and Western Blot methods, whose results most often turn out to be "false HIV positive". The issue with the Western Blot and Elisa screening methods is that, the two are used mostly as preliminary tests rather than as confirmatory tests. According to the U.S. Centers for Disease Control (CDC), the Western Blot method is somehow more reliable than the Elisa method, nevertheless, the results thus obtained should never be used alone to report a final "positive" result. If two or more blood tests are reactive on Elisa, the results should be further confirmed using a second more specific antibody test with the Western Blot method. Today in the US, a person will be said to be HIV positive only if they have been repeatedly reactive by Elisa and are confirmed by Western Blot. No one in Africa or anywhere else, should be required to bear this ethical burden without a solid guarantee of the veracity of the HIV/AIDS test and its interpretation. This challenges us as to the nature of the tools we use for screening in terms of their accuracy, especially in communities where chronic parasitic ailments, malnutrition and HIV/AIDS are endemic. Hodgkinson (1996), in a book entitled Aids: The Failure of Contemporary Science, has stated that HIV/AIDS tests based on Elisa and Blot methods are completely flawed. He warns that many doctors and researchers in Africa had in the past erroneously declared many people as HIV positive after using such controversial methods of testing HIV without caution. For instance, in Zaire, of the 57 leprosy patients tested using the Elisa method by Dr. Max Essex, 41 tested positive using one Elisa Kit when the samples were retested using Western Blot only 2 of the leprosy patients tested positive. both numbers however, were entered into the HIV/AIDS statistics. Thus, for societies in Nyanza, where figures on HIV/AIDS endemicity seem to be so high, how authentic are the tools used in screening? How representive are the HIV/AIDS figures? Could it be hunger and not HIV/AIDS that is killing the majority of people in Nyanza? This hypothesis needs to be fully tested afresh. It appears that the current low quality of life among mothers and children is rooted in the community's collapsing food system, unsafe water supply, energy crisis, and poverty. Poverty is aggravated by the crumbling household wealth resources. Coupled with large family sizes and pressure on dietary requirements, nutritional status of mothers and children is generally low. In whatever facet we look, eating frequency in most households was poor and the quality of life generally low (see Fig. 1).
REFERENCES
Copyright © Quest and Insight Publishers and Friends-of-the Book Foundation, 2001 The following images related to this document are available:Photo images[fn01007t5.jpg] [fn01007t4.jpg] [fn01007f1.jpg] [fn01007t6.jpg] [fn01007t2.jpg] [fn01007t3.jpg] [fn01007t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}