 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 1, Jan-Mar, 2004, pp. 14-18 ORIGINAL ARTICLE ANALYSIS OF CARCINOEMBRYONIC ANTIGEN, NEURON SPECIFIC ENOLASE, CYTOKERATIN 21-1 AND FERRITIN LEVELS IN COAL MINERS Ferah Armutçu1, Remzi Altın2, Ahmet Gürel1, Levent Kart2, Murat Unalacak3, Arif H Çımrın4 Karaelmas University, Faculty of Medicine, Departments of Biochemistry1, Pulmonary Medicine2, Family Practice3,
Dokuz Eylül University, Faculty of Medicine, Department of Pulmonary
Medicine4 Code Number: gm04005 Coal miners have an increased risk of pneumoconiosis. Tumor markers that are used in screening, diagnosis and follow-up of lung cancers are also useful to distinguish malignant and benign lung disorders. Carcinoembriyonic antigen, neurone specific enolase, cytokeratin 21-1 and ferritin were studied to compare and examine the possible contribution of CEA, NSE and CYFRA in the diagnosis of early and low-grade pneumoconiosis in coal miners with (34 cases) or without pneumoconiosis (27 cases). There were statistically significant differences between groups concerning NSE and ferritin levels (p<0.001, p<0.001 respectively). No difference was obtained for CYFRA 21-1 and CEA (p<0.05). The relationship of NSE with age and smoking was investigated, but no correlation was found (r=0.224, p=0.204; r=0.291, p=0.095 respecitvely). However, there was a positive correlation between NSE and exposure duration (r=0.425, p=0.012). Similarly, there was no relationship between ferritin levels and age or smoking (r=0.230, p=0.191; r=0.248, p=0.158 respectively), but there was a positive correlation with exposure duration (r=0.390, p=0.023). In conclusion, NSE and ferritin were found to be higher in coal miners with pneumoconiosis. According to these results, tumor markers are neither sensitive nor specific enough for the determination of early and low grade pneumoconiosis. One of the interesting and important findings of this study is that NSE values were higher than 12.5 µg/mL in most of the pneumoconiosis cases (%73.5). So, the NSE cut-off value used in cancer screening of coal workers with pneumoconiosis should increased. Key words: CEA, CYFRA 21-1, NSE, ferritin, pneumoconiosis, coal workers. INTRODUCTIONCoal worker’s pneumoconiosis (CWP) is characterized by coal dust inhalation, deposition in the lungs, and tissue reaction to coal particles (1). The risk of pneumoconiosis is higher in coal miners (2). Tumor markers are used in screening, diagnosis and discrimination of malign and benign lesions of the lung (3,4). In recent studies, it is pointed out that CEA, NSE and CYFRA may be used in the diagnosis of benign pulmonary lesions (5,6,7). In this sudy, we aimed to compare examine the possible contribution of CEA, NSE and CYFRA in the diagnosis of early and low-grade pneumoconiosis in coal miners, with or without pneumoconiosis. MATERIAL AND METHODSPatients The study was performed between June and August 2002 in Zonguldak Karaelmas University Hospital. Early and low grade pneumoconiosis cases (n:34) and controls without pneumoconiosis (n:27) were randomly selected among coal miners. Profusions of pneumoconiosis cases were between 0/1 to 2/2 according to ILO 1980 classification (8). All cases were male. Chest X-ray and pulmonary function tests were performed to rule out lung cancer, COPD, asthma and tuberculosis etc. Workers who had any infection in the previous month were excluded from the study. To obtain the data of demographic features and smoking history, a questionnaire was filled by a chest physician for each worker. Informed written consent was obtained from all subjects. Table 1. The demographic features of pneumoconiosis and non-pneumoconiosis coal workers ( mean±SD)
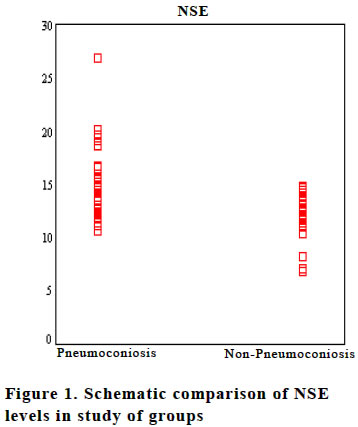
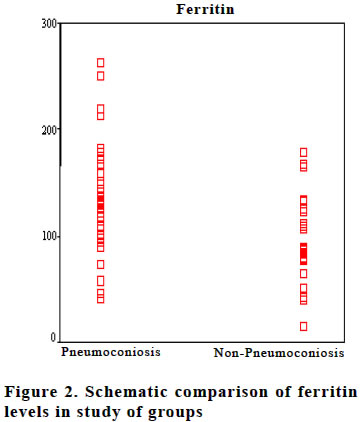
*smoker cases Tumor markersFive cc venous blood was taken from each worker after 12 hours fasting and stored at -20 Co. NSE, CEA, CYFRA 21-1 and ferritin levels were measured by electrochemiluminescence methods by using commercial kits (Elecsys 2010 immunassay, Roche Diagnostics, USA). Statistical analysis Analytic results were obtained by using SPSS programme (11.0 version, SPSS Inc., Chicago, IL, USA). The difference between the means of variables in two groups was tested by Mann-Whitney U test (nonparametric). The relationship between tumor markers and age, smoking and exposure duration were analysed by Spearman correlation test. Significance was set at 5% level (p< 0.05). All measured values were given as mean ± SD (standard deviation). RESULTSDemographic characteristics of the coal workers are given in Table 1. There was no difference concerning age, smoking and exposure duration between coal workers with or without pneumoconiosis (p>0.05). The measurements of CEA, NSE, CYFRA 21-1 and ferritin levels are shown in Table 2. When NSE and ferritin levels were analyzed there were statistical differences between groups (p<0.001, p<0.001 respectively; figure 1 and 2). However, no difference was obtained for CEA and CYFRA 21-1 (p>0.05). The relationship between NSE and age, smoking and exposure duration were investigated. There was a positive correlation for exposure duration (r=0.425, p=0.012), but no correlation was found for age and smoking (r=0.224, p=0.204; r=0.291, p=0.095, respectively). Similar results were obtained for ferritin levels and age (r=0.230, p=0.191), smoking (r=0.248, p=0.158, respectively) and exposure duration (r=0.390, p=0.023). The cut-off value of NSE used to distinguish malign and benign lesions is accepted as 12.5 µg/mL. According to our data, the number of cases over 12.5 µg/mL was 25/34 (73.5%) in the group with pneumoconiosis and 11/27 (40.7%) in workers without pneumoconiosis. If the value of 12.5 µg/mL was taken as the reference cut-off, the sensitivity of NSE was found to be 70.6% and specificity to be 61.5%. From the study results, the cut –off value to distinguish coal miers without pneumoconiosis and early and low grade pneumoconiosis was found as 16.5 µg/mL. Table 2. The comparison of NSE, CEA, CYFRA 21-1 ve ferritin measurements in coal workers with pneumoconiosis and non-pneumoconiosis (mean±SD)
*p<0.001, **p>0.05
In this case, sensitivity and specifity were 65% and 81.3% respectively. DISCUSSION Coal workers’pneumoconiosis (CWP) is characterized by coal dust inhalation, deposition in the lungs and tissue reaction to coal particles. There may be no symptoms in early and low grade CWP (1). Additionally, there are inter and intra reader differences in chest X-ray evaluation (9,10). CEA, NSE, CYFRA 21-1 and ferritin, used in lung cancer diagnosis, have also been found increased in benign lung diseases (11,12). In the literature, there are no data that these tumor markers are used to distinguish early and low-grade pneumoconiosis. Carcinoembryonic antigen is used in the diagnosis of colorectal, gastrointestinal, breast and lung cancers. It is found to be elevated in some benign diseases such as cirrhosis (45%), pulmonary emphysema (30%), rectal polyps (5%), benign breast diseases (15%) and ulcerative colitis (15%) (11,13). In our study, although there was a proportional difference between pneumoconiosis and non-pneumoconiosis cases, it was not statistically significant (p>0.05). Neuron specific enolase is a glycolytic enzyme also known as phosphopyruvatehydr atase. It is found in neuroendocrine cells that have precursor uptake and decarboxilation. It is detected in neuroendocrine tumors (SCLC, neuroblastoma, pheochromacytoma, carcinoid, thyroid medullary carcinoma and pancreatic neuroendocrine tumors). The cut-off value for NSE is 12.5 µg/mL (14). NSE is especially important in staging of small cell lung cancer. It is increased in 60-81% of SCLC patients. An increased NSE level has also been shown in benign lung diseases (15). There was a statistically significant difference of NSE level between pneumoconiosis and non-pneumoconiosis cases (p<0.001). If the value of 12.5 µg/ mL was taken as reference, the sensitivity was found to be 70.6% and specificity to be 61.5%. From the study results, the cut –off value to distinguish coal miers without pneumoconiosis and early and low grade pneumoconiosis was found as 16.5 µg/mL. In this case, sensitivity and specifity were 65% and 81.3% respectively. When correlation analyses were performed between NSE and age, smoking and exposure duration, it was shown that the only statistical difference was obtained for exposure duration. As the number of study cases was low in number, this might affect the results about smoking. On the other hand, as our study cases were in middle age, it is reasonable to expect that age did not affect the results. In our study, cut-off values were exceeded in 25 of 34 (73.5%) cases. Cut-off values are important in differentiation of malign and benign diseases. These values may change according to the methods and kits used. In the study of Pina et. al., NSE cut-off values were measured as 9.8 µg/mL by EIA method in lung cancer screening patients (16). Kuralay et al. found this cut-off value as 8.7 µg/mL by EIA in malign and benign pleural effusions (12). In our study, we used an electrochemiluminescence method and, according to this method, the accepted cut-off level was as 12.5 µg/mL. From our results, it is possible to say that the NSE cut-off level must be taken higher than 12.5 µg/mL in patients with early and low grade pneumoconiosis in discrimination of malign and benign lesions. Ferritin, one of the tumor markers, is also a nonspecific acute phase reactant, which increases in case of inflammation, infection, trauma and cancer. The reference interval for adults is 20-250 µg/L (11,17). There was a statistically significant difference of ferritin levels between pneumoconiosis and non-pneumoconiosis cases (p<0.001). But, as only a few workers had high levels of ferritin over 250 µg/L (only two cases), it seems that ferritin may not be useful in discrimination of normal coal workers without pneumoconiosis and coal workers with early pneumoconiosis. Cytokeratins are structural proteins that form subunits of filaments. In measurement of CYFRA 21-1, monoclonal antibodies are used and fragments of cytokeratin-19 are measured. CYFRA 21-1 is an important marker in follow-up of Non SCLC patients (18,19). The cut-off value of CYFRA 21-1 is 3.3 ng/mL. It is increased in cases of acute pneumonia, tuberculosis, interstitial lung diseases, cirrhosis and renal failure (20). There was no difference between pneumoconiosis and non-pneumoconiosis cases. In addition, none of the cases had a value higher than the cutoff limits used for malign and benign lesions discrimination. In conclusion, NSE and ferritin levels were found to be higher in coal workers with pneumoconiosis. According to our results, tumor markers are neither sensitive nor specific enough for the determination of early and low-grade pneumoconiosis. One of the interesting and important findings in this study is that NSE values were higher than 12.5 µg/mL in most of the pneumoconiosis cases (73.5%). The NSE cut-off value used in cancer screening of coal workers with pneumoconiosis should be increased in this setting. REFERENCES
Copyright 2004 - Medical Investigations Society
The following images related to this document are available:Photo images[gm04005f2.jpg] [gm04005f3.jpg] [gm04005f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}