 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 1, Jan-Mar, 2004, pp. 19-25 ORIGINAL ARTICLE RESULTS OF “EPHESOS”CORONARY STENT IMPLANTATION IN PATIENTS WITH UNSTABLE OR STABLE ANGINA Igor Pershukov1, Talantbek Batyraliev2,Anatolii Samko3,Yuri Belenkov3, Zalema Niyazova-Karben2, Oleg Calenici4 Regional Clinical Hospital1, Sani Konukoğlu
Medical Center2, Myasnikov’s Clinical Cardiology Institute
of CRC HM RF3, Institute of Cardiology4, Kishineu Code Number: gm04006 This is an open non-randomized study designed to evaluate clinical and angiographic short-and long-term results of the EPHESOS stent implantation in 457 patients (M/F=348/109) with unstable angina (UA) or stable angina (SA) and native lesions. In SA group 268 stents were implanted in 231 patients. In UA group 271 stents were implanted in 226 patients. 46% of lesions were complex. The length of stenosis was 12.9±6.7 mm in SA group, and 14.1±7.4 mm in UA group. The rate of long stenosis was 30%. Coronary Stenting success rate appeared to be 99% of cases free from acute thrombosis. 1.3% of patients in UA group suffered a non-fatal myocardial infarction (MI) during the in-hospital period. Major adverse cardiac events (MACE) rate including mortality rate and the occurrence of recurrent angina, MI and restenosis as well as repeat revascularization during 6-month follow-up, was 15.6% in SA group and 18.1% in UA group. Angiographic 6-month control revealed the loss index of 0.22±0.20 in SA group and 0.30±0.27 in UA group. 18-month follow-up did not reveal any significant differences in MACE rate between the groups (21.6% for SA and 22.6% for UA group). These results indicate the efficacy and safety of EPHESOS stent with reasonable rates of stent thrombosis and restenosis in SA and UA patients undergone high risk endovascular interventions. Key words: Unstable angina, stent, major adverse cardiac events, restenosis, target lesion, revascularization. INTRODUCTIONUnstable angina (UA, acute coronary syndrome without ST-segment elevation) represents a continuum of acute ischemic episodes that have also been called preinfarction angina, premonitory angina, intermittent angina, winking and blinking angina, and stuttering angina (1). The majority of patients with UA do not usually suffer the full closure of a coronary artery, and thus some cardiologists (2) think their efforts should primarily be aimed not at the myocardium revascularization, but at the drug treatment of myocardial ischemia and prevention of intracoronary thrombus development. Until recently percutaneous coronary interventions (PCI) were reported to cause more complications in patients with UA than with stable angina (SA) (3,4). On the other hand, early PCI resulted in to considerable shortening of in-hospital period for patients with UA (3,5). Coronary stents implantation became a leading technology among PCI after the establishment of optimum regimen of antiplatelet therapy and the rates of acute and subacute thrombosis after implantation had been lowered (6). Besides, coronary stents significantly improved the long-term outcomes. Unfortunately used stents for the study of the long-term effectiveness of coronary stenting (CS) in patients with UA were not currently avaliable and new types were emerged (7). This is the reason why we decided to estimate the outcome of the EPHESOS coronary stent implantation in patients with SA or UA. The stent is produced by NEMED Ltd. (Turkey) and is currently available in Turkey, Russia and other countries. We already studied the results of the EPHESOS implantation in few groups of patients with favorable short and long-term outcomes (8,9). The goal of the present study is to evaluate in hospital, six and 18 months outcomes of CS including rates of restenosis and repeate target vessel revascularization (TVR). MATERIAL AND METHODSPatients Selection Criteria All 457 patients in this study were hospitalized between January 1998 and March 2002. They had stable angina (CCS class III or IV) or unstable angina (Braunwald classification IIB/C or IIIB/C). We included patients with one or more hemodynamically significant coronary stenosis (binary level over 50% of the vessel diameter) in one or more coronary artery revealed by X-ray coronary angiography. 109 of 457 patients were women and 348 were men, mean aged 56±12. They were divided into 2 groups. The first one consisted of 231 patients with SA, and the second one consisted of 226 patients with UA diagnosed at hospitalization or developed before CS. Exclusion criteria were as follows; any previous PCI in the target vessel, previous coronary artery bypass grafting (CABG), first seven days of acute myocardial infarction (MI) with Q-wave, reference vessel diameter (RVD) of target lesion less than 2.5 mm, and glycoprotein IIb/IIIa antagonists usage prior to CS. All the patients involved in the study were informed of the treatment and their written informed consent was obtained. Stent Characteristics The EPHESOS is a laser cut 316 L stainless steel balloon-expandable stent. Longitudinal symmetry of the stent structure prevents heterogeneity of expansion at low pressure (8 atm). The EPHESOS stent is available in 9, 12, 15, 18 and 21 mm lengths. The stent expansion does not lead to its considerable (>0.5mm) shortening. The stent is mounted on a coronary balloon catheter (TROYA, NEMED Ltd, Turkey). Stenting Procedure The stent was deployed with a single dilatation at 8 atm within 20-30 seconds. Reference artery diameter was achieved through additional dilatations at 10-16 atm. Medical Regimen Acetylsalicylic acid 80-325 mg per day to be taken on a regular basis was administered to all the patients at hospitalization and was continued indefinitely after discharge. Clopidogrel 75 mg per day was administered, whenever possible, either a day prior to, or right before CS. 17% of patients in SA group, ticlopidine was administered instead of clopidogrel, 500 mg daily, a week prior to CS. The same dosage of clopidogrel or ticlopidine was continued for a month after CS. Follow-up CS outcome analysis included four end points. The primary end point included immediate angiographic results, such as mortality rate and the occurrence of acute CA occlusions and MI. The secondary end point included in-hospital clinical results –freedom from MACE (mortality rate, the occurrence of MI and TVR). The third end point was a composite one consisting of clinical and angiographic results during the first 6 months after CS. These results were analyzed as soon as any of the events took place or when the period of follow-up was over. Clinical results (MACE) included mortality rate, repeat TVR or CABG, the occurrence of MI and recurrent angina associated with the target vessel. The rate of restenosis and late loss were determined by angiographic controls done after six months. The results of 18 months were also analyzed. Angiographic analysis included defining X-ray morphology of the coronary artery stenosis on the basis of American College of Cardiology and American Heart Association joint classification (3). Quantitative coronary analysis (QCA) was made by ANCOR or QuantCor automatic edge-detection systems (Siemens, Germany). QCA included the minimal lumen diameter (MLD) calculation prior to CS; RVD; percentage of the stenosis and lesion length. Any MLD changes were registered immediately after CS and after the six months follow up. We defined acute gain of the lumen diameter (postprocedural MLD minus preprocedural MLD), late loss (postprocedural MLD minus MLD at follow-up), final luminal diameter (MLD at follow-up minus preprocedural MLD) and loss index (ratio between late loss and acute gain). Statistical analysis Continuous variables are expressed as means ± SD. Differences between the groups were evaluated on the basis of Chi-square test, Fisher exact test, Z-test or Student’s t-test. An estimate of survival was determined with the help of Kaplan and Meier method. Cox F-test was used to define the differences between the groups of SA and UA patients free from MACE. A p-value of < 0.05 was considered statistically significant. “Statistica for Windows Release 5.5A”(StatSoft Inc) package software was used in the analysis. Table 1. Baseline clinical and angiographics features
SA: stable angina, UA: unstable angina, MLD: minimal luminal diameter, RVD: reference vessel revascularization RESULTSThe baseline clinical and angiographic characteristics of the groups were summarized in Table 1. It was figured out that patients with UA were more likely to have had prior MI, whereas patients with SA were prone to single vessel lesions and type A/B1 stenosis. Forty one percent of patients had hemodynamically significant stenosis in two coronary artery or two segments of the same coronary artery. In 18% of these patients lesions were stented in one procedure. The immediate results of CS are presented in Table 2. A total of 536 EPHESOS stents were successfully implanted in 454 patients. After CS only 2 patients with UA and 1 patient with SA needed an immediate implantation of the second stent due to significant elastic recoil in the area near the stent. The second CS was successful in all the three patients, with one stent partially overlapping the other.
TIMI: Thrombolysis in myocardial infarction, RVD: reference vessel revascularization, MLD: minimal luminal diameter Table 3. In-hospital outcome (%)
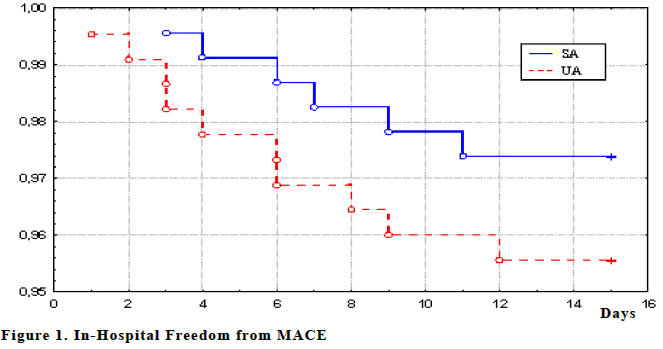
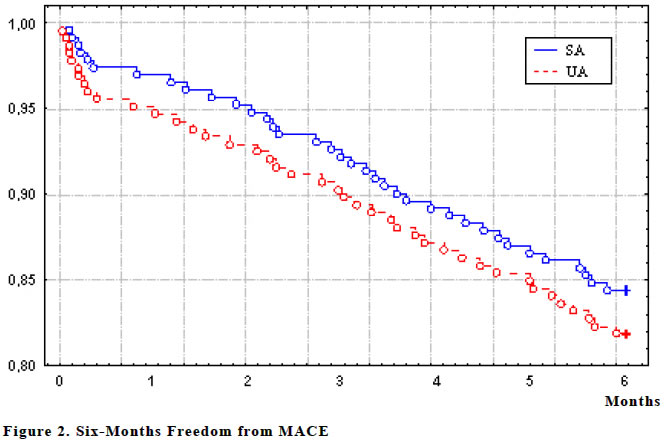
The rest of the patients (454) no acute complication was developed after CS. Thus, the implantation of 539 stents in 457 patients did not lead to the occurrence of D-F dissections, acute occlusions or ‘no reflow’phenomenon. Most of the patients from both groups had TIMI 3 blood flow. Other 5 patients with SA and 9 patients with UA had the final blood flow corresponding to grade 2 of TIMI classification. The final balloon-to-artery ratio was 1.0±0.1. There were no significant differences in CS results between the two groups. During the time of hospital follow-up 2 patients from SA group and 3 patients from UA group died. They developed MI with cardiogenic shock within the first 1-3 days after CS. Repeat PCI with intraaortic balloon pump support was ineffective. Besides, 3 patients from SA group and 6 patients from UA group had coronary artery occlusion with non-fatal MI within the first 2-9 days after CS. That was successfully treated by repeat PCI. Thus, 97.4% patients from SA group and 95.6% patients from UA group were MACE-free (p>0.05). Table 3 presents hospital outcomes, and Figure 1 shows curves of a cumulative rate of patients without MACE. Further follow-up during the 6-month period (Table 4) showed that 1 patient in each group died due to fatal MI associated with the target vessel. Recurrent angina and non-fatal MI occurrence associated with the target vessel were registered in 24 patients from SA group and 29 patients from UA group. All the patients with recurrent angina were successfully treated by repeat revascularization (TVR or CABG). Table 4. Six and eighteen months clinical outcome (%)
CABG: coronary artery bypass grafting, MI: myocardial infarction, TVR: target vessel revascularization, UA: unstable angina Table 5. Six month angiographic outcomes
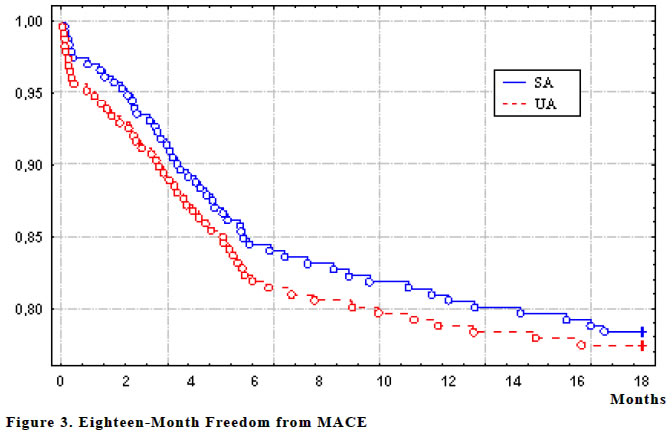
RVD: reference vessel diameter, MLD: minimal luminal diameter Angiography was performed at six months in 218 patients (48%) and revealed silent restenosis of the stented artery in 3 patients in each group. That was successfully treated by repeat PCI. Thus, during the first 6-months period, repeat interventions were performed in SA group as 11.7% and in UA group as 14.2%. Consequently, there were 84.4% MACE-free patients in SA group and 81.9% in UA group (p>0.05). MACE-free cumulative rate is shown in Figure 2. Table 5 displays the results of angiographic control at six months. After the 6-month follow-up period, 7 patients were excluded (3 patients from SA group and 4 from UA group). During the following year (up to 18 months) 5 cardiac deaths were registered (3 in SA group and 2 in UA group). 3.9% patients in SA group suffered acute MI in the target vessel. 4.4% of patients in SA group and 4.5% in UA group were treated by repeat revascularization. Thus, MACE-free rate at 18-month follow-up was 78.4% in SA group and 77.4% in UA group. There were no significant differences between the groups for MACE rates at 18 months. Figure 3 represents MACE-free cumulative rate. For clinical control results at 18 months see Table 6. DISCUSSIONPrevious studies showed that stent design and its coating influence the rate of thrombosis and neointimal hyperplasia in the target lesion (10-13). Previous results of the EPHESOS stent implantation were associated with a high rate of success of the implantation itself, a number of MACE-free patients and a low rate of restenosis. In the present study, EPHESOS stents were successfully implanted in all attempted lesions. The success rate in both groups exceeded 99% of cases. Stent restenosis rate at 6 months was 12% in SA group and 14% in UA group. Due to the given rate of restenosis the EPHESOS stent can be considered as a safe and effective stent types (10,14-16). This rate shows that EPHESOS has an advantage over different types of stents (7,10,17,18). A low rate of restenosis can somewhat be explained by a large mean RVD of the sample. On the other hand, similar results were obtained in both groups of patients with SA and UA, the majority of which had lesions with high risk of restenosis (B2 or C stenosis, long lesions). Although there were differences in SA and UA patients’ initial status, we did not find any significant differences in MACE rate associated with CS during 18 months. UA group was more prone to MACE during the first two weeks after CS (Figure 1). This rates may be effected by the lack of glycoprotein IIb/IIIa antagonist usage. At 6 months the difference in MACE rate was 2.5% (p>0.05), and at 18 months MACE rate was tended to decreased (1%, p>0.05). Thus, we came to a conclusion that UA did not have any significant unfavorable effect on the short- and long-term outcomes after CS. The study was not designed to compare the EPHESOS stent with other types of stents. Besides, it was not our goal to compare the stenting procedure and the routine coronary balloon angioplasty. Nevertheless, the results of the study indicated the benefit of EPHESOS stent for complex coronary lesions in SA and UA patients with favorable short- and long-term outcomes. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04006f1.jpg] [gm04006f3.jpg] [gm04006f2.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}