 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 1, Jan-Mar, 2004, pp. 28-30 CASE REPORT GOLDENHAR SYNDROME ASSOCIATED WITH BILATERAL OCULAR CHORISTOMAS AND CARDIAC ABNORMALITIES* Murat Özdemir1, Mesut Garipardiç2, Aytekin Güven3, Gökhan Özdemir1 Sütçü �mam University, Faculty
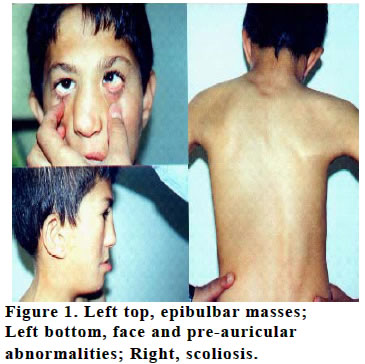
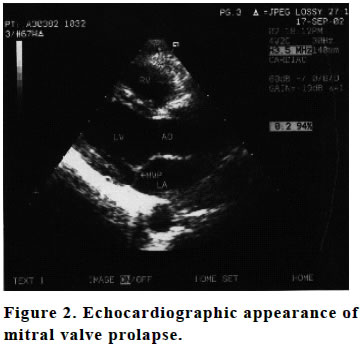
of Medicine, Departments of Ophthalmology1, Pediatric Diseases2 and Cardiology3 *This report presented in 36th National Congress of Turk Ophthalmology Society in October 2002, Ankara, Turkey. Code nUmber: gm04008 This study presents a report on a 14-year-old male with Goldenhar syndrome featuring bilateral epibulbar mass, right hemifacial microsomia, deafness, and right scoliozis. Cardiac disorders including systolic murmur, sinusoidal arrhythmia, and prolapse of mitral valve were detected in the case. Goldenhar syndrome needs to a multidisciplinary approach regarding craniofacial and cardiologic associations. Ophthalmologists should focus on visual sequels and amblyopia. Key words: Goldenhar syndrome, epibulbar dermoids, mitral valve prolapse INTRODUCTIONGoldenhar syndrome defines a group of disorders characterized by oculo-auriculo-vertebral (OAV) developmental anomalies. OAV anomalies demonstrate a wide range of variations from isolated pre-auricular skin tag to total atresia of ear and hemifacial microsomia coexisting with microphtalmia (1). Pulmonary and cardiovascular system anomalies may accompany Goldenhar syndrome (2,3). In this report, a deaf-mute case with Goldenhar syndrome associated with bilateral epibulbar mass and cardiologic manifestations is presented. CASE REPORTBilateral limbal mass and facial microsomia were defined in a 14-year-old deaf-mute boy (Figure 1). Physical examination revealed bilateral maxillomandibular hypoplasia (prominent on the right), facial asymmetry and hypoplastic ear tragi. Painless, irregularly demarcated, slightly mobile multiple masses giving cartilage sensation on palpation with a diameter of 3-4 mm were detected in preauricular region just underneath the skin. Operated cleft palate and lip were present. Malocclusion of tooth arches and mixed type hearing loss were detected. A systolic murmur was heard in mitral area at cardiologic examination. Sinusoidal arrhythmia in ECG, mitral valve prolapsus (Figure 2) with mild mitral insufficiency were detected in echocardiography. Right scoliosis was present in vertebral examination (Figure 1). Genitourinary system, extremities and the level of intelligence was normal. Ocular findings Inferotomporal epibulbar limbal mass overcoated with hair, consistent with dermoid cyst was present in both eyes (Figure 1). Fibrovascular invasion of 2.5 mm on the cornea at 6 o’clock location was present in the left eye causing against-the-rule astigmatism of 1.5 diopters. Anterior segment and fundus examinations were normal. Visual acuity was 10/10 in both eyes and globe movements were full. DISCUSSIONGoldenhar syndrome is seen once every 3000 live born with slight (3:2) male predominance (4). It is usually sporadic but may present as an autosomal dominant or autosomal recessive condition with marked variability in expression. Main manifestations are mainly related to ocular, auricular and vertebral system, but other organ manifestations can also be seen. OAV malformations have heterogeneous etiology and originate from the anomalous development of tissues derived from the first and second branchial arches. The pathophysiology appears to be related to vascular occlusion and/or neural crest disruption (5). Epibulbar choristomas are the most frequent (32%) ocular finding in Goldenhar syndrome (6). Motility disorders, blepharoptosis, palpebral fissure, eyelid colobomas, anomalies of lachrymal drainage system and retina and optic nerve anomalies (7) were also reported. No other ocular pathology except bilateral epibulbar masses were seen in our case. Bilateral ocular involvement is very rare. The frequency of bilateral lesions had been reported as lipodermoids, 12%; lachrymal anomalies, 11%; and upper lid coloboma, 3% (8). Epibulbar choristomas in Goldenhar syndrome are congenital tumors demonstrated characteristics of dermoid or lipodermoid with a rather limited potential of enlargement and usually has inferotemporal localization. Most of the limbal epibulbar dermoids are superficial and very few of them show invasion on sclera or cornea. Surgical considerations depend on tumor extent and associated features such as astigmatism, cosmesis, irritation, and exposure keratitis. All contribute variably to central visual axis obscuration and resultant amblyopia (8). Lipodermoids tend to extend posteriorly in the orbit and may benefit from radiographic delineation if surgical excision is contemplated. Management of ocular adnexial choristoma tends to be conservative. Surgery itself should be limited to superficial debulking when possible as incomplete excision can lead to an intense chemically induced fibrosis from intralesional lipid, leading to restrictive squints and relative dry eye, all deleterious to visual development (6). In our case, the mass in the left eye showed invasion on the cornea for almost 2.5 mm and caused against-the-rule astigmatism. The corrected visual acuity of the patient was 10/10 and the lesion did not cause any motility disorders of the eyeball and eyelids. No exposure keratopathy was detected. Patient was all right with the cosmetic appearance and we decided not to excise the mass. Mixed type hearing loss is frequently encountered in Goldenhar syndrome due to stenosis, deformity or even total atresia of the external auditory tube (9). Audiologic examination of our patient who in fact was a student in a specific deaf-mute school, mixed type hearing loss was determined. Multiple subcutaneous masses with a diameter of 3-4 mm (probably dermoid) were also seen in the pre-auricular region. Bony deformities related to the face, jaw and vertebrae are frequently reported in Goldenhar syndrome (10). Right maxillomandibular hypoplasia, cleft palate and lip, and right scoliosis were found in our patient. Frequency of cardiovascular malformations in this syndrome varies between 5-58% (2,3). Cardiovascular developmental anomalies in Goldenhar syndrome are usually severe, such as tetralogy of Fallot, ventricular septal defect, Wolf-Parkinson-White syndrome and other vascular anomalies (2,3). The association of mitral valve prolapsus with Goldenhar syndrome was reported only one study previously (11). We wanted to emphasize the presence of mitral valve prolapsus in addition to mild mitral insufficiency and sinus arrhythmia in our cases. Since the patient was asymptomatic, only follow-up was advised. Goldenhar syndrome requires multidisciplinary approach. Ophthalmologists should focus on visual sequels and closely follow the patients for amblyopia, strabismus, astigmatism, retraction in the movements of the eyeball. Since cardiologic manifestations of Goldenhar syndrome may be serious in some case, a detailed cardiologic and other system examinations should be performed for early diagnosis and management. To clear the association of cardiac anomalies to ocular findings, more comprehensive and detailed analysis should be undertaken. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04008f3.jpg] [gm04008f1.jpg] [gm04008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}