 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 1, Jan-Mar, 2004, pp. 31-33 CASE REPORT CAROTICO-CAVERNOUS SINUS FISTULA: DUPLEX DOPPLER FINDINGS Ömer Etlik1, Ali Bay2, Mustafa Harman1,Osman Temizöz1, Mustafa Kayan1, M. Emin Sakarya1 Yüzüncü Yıl University, Faculty of
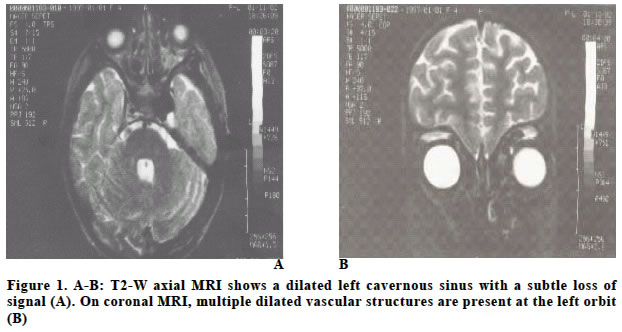
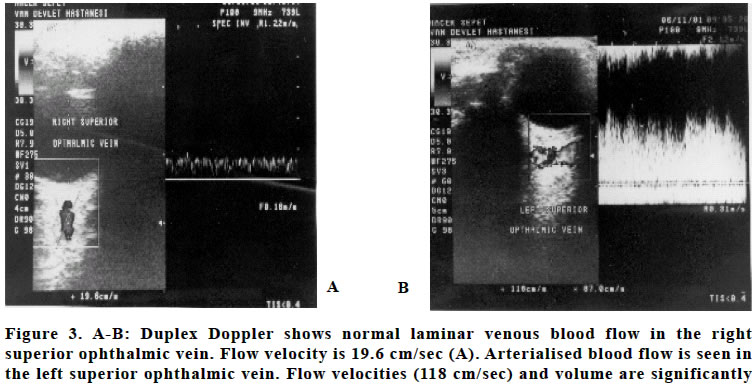
Medicine, Departments of Radiology1 and Pediatric Diseases2 Code Number: gm04009 We report a case of an 8-year-old child with traumatic carotico-cavernous fistula. The diagnosis was obtained by magnetic resonance imaging, magnetic resonance angiography and Doppler imaging and the fistula treated by percutaneous embolisation. We emphasize the duplex Doppler findings of superior ophtalmic vein in this study. Key words: Carotico cavernous fistula, duplex Doppler, INTRODUCTIONCarotico cavernous sinus fistula (CCF) is an abnormal communication between the carotid artery and the cavernous sinus and is classified angiographically as dural or direct. Spontaneous CCF is a dural arterio-venous fistula at the cavernous sinus which is different from traumatic CCF or CCF associated with a ruptured aneurysm at the cavernous internal carotid artery. Cerebral angiography is required in order to differentiate these conditions (1,2) .We report a case of traumatic CCF, in which Doppler sonographic evaluation of the superior ophthalmic vein (SOV) corresponded with that of magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA). CASE REPORTA 8-year-old child had deteriorating visual activity and ocular pain in her left eye. Ocular examination showed exophthalmos, vascular tinnitus, 6th cranial nerve palsy, exposure keratopati, decreased ocular motility in all direction and chemosis several weeks after a minor closed head injury. The right eye was normal. There was no demonstrable fracture on brain computerized tomography at the time of original trauma. MRI showed an enlarged left cavernous sinus and enlarged periorbital vessels (Figure 1-A,B). The existence of a fistula was first diagnosed by brain MRI and MRA. Brain MRI showed an abnormal flow-void signal in the left cavernous sinus and dilated left cavernous sinus and periorbital veins. The MRA of the internal carotid artery system revealed an abnormal flow-related enhancement in the left cavernous sinus with extension anteriorly (Figure 2). Duplex Doppler demonstrated normal laminar venous flow in the right SOV. Doppler imaging demonstrated arterialised venous blood flow in the enlarged left SOV suggestive of a direct arterio-venous communication. The maximum velocity was elevated at 118 cm/sec (Figure 3-A,B). For comparison maximum velocity was 19.6 cm/ sec in the right SOV. In conclusion a CCF was diagnosed by MRI, MRA and duplex Doppler. The patient was referred to a specialist center and treated with endovascular approaches. We observed the improvement of clinical symptoms in 1 year follow up period. DISCUSSIONTraumatic CCF are almost always direct and are caused by laceration of the internal carotid artery (ICA) within the cavernous sinus, or rupture of its intracavernous dural branches. The cavernous ICA is fixed to the dura mater at the skull base, limiting its mobility and therefore predisposing it to injury. Arteriovenous shunting leads to arterialisation of the cavernous sinus and venous channels that drain into or out of it (3). Depending on the amount and direction of venous drainage from the cavernous sinus, the upper cranial nerves maybe affected. When the shunt drains posteriorly into the petrosal sinus, an isolated oculomotor, trochlear, or abducens nerve palsy may develop (4). We observed a 6th cranial nerve palsy in our patient. Enlargement of the SOV, although usually considered a sign of CCF, may be found with other disorders such as Graves ophthalmopathy, orbital pseudotumor, and parasellar meningioma (5), however arterialised flow in a dilated SOV is seen only in CCF, both of which were seen in our patient. Previous reports have demonstrated that MRI is useful in detecting this condition. Swollen extraocular muscles, proptosis, a dilated superior ophthalmic vein and signal loss in the involved cavernous sinus on T2-weighted MRI due to rapid blood flow within the arteriovenous shunt have all been described in CCF (2). In three dimensional-time of flight-magnetic resonance angiography (3D TOF MRA), magnetically unsaturated blood flowing into the imaging volume produces flow-related enhancement which distinguishes it from adjacent stationary tissue. Low blood flow that normally exists within the cavernous sinus does not produce flow-related enhancement normally; an increased blood flow velocity within the cavernous sinus is therefore suggestive of an arteriovenous fistula (6), as observed in our patient. Although MRA has some limitations compared with selective angiography, including lower spatial resolution, presence of saturation artifact, and lack of transit time information (7), our results clearly indicated that MRA was of value in the evaluation of CCF. Duplex Doppler imaging is a useful technique to diagnose CCF by showing the characteristics of arterial rather than venous blood flow in an enlarged SOV (8). In this case, we demonstrated arterialised high-velocity blood flow in the left SOV while normal venous flow was seen in right SOV. We found characteristic duplex Doppler findings associated with a high-flow CCF, but perhaps more importantly, found this technique to be an excellent tool also for detecting and following treatment results in low-flow CCF. The low-flow fistulae exhibit less specific clinical signs and are harder to distinguish using the non invasive radiological methods of MRI and MRA. Duplex Doppler parameters (arterialised blood flow in the ophthalmic vein, increased blood flow velocity) for CCF are specific, and are thus valuable in the hemodynamic assessment of these lesions; as dural CCF feature more subtle hemodynamic changes the MRA and MRI findings may be normal (9). These cases pose a diagnostic challenge. In these situations, orbital duplex Doppler reveals specific diagnostic findings and allows the examiner to determine whether cerebral angiography is indicated. Doppler imaging will not replace cerebral angiography, but it represents a valuable adjunctive imaging technique. We believe that duplex Doppler imaging is the most easily applicable method to monitor the clinical course of CCF and that it should be performed prior to cerebral angiography. To our knowledge, there are few reports of duplex Doppler imaging in CCF. This non-invasive technique represents a potential alternative method to invasive vascular studies in the diagnosis and evaluation of CCF. REFERENCES
Copyright 2004 - Medical Investigations Society
The following images related to this document are available:Photo images[gm04009f2.jpg] [gm04009f1.jpg] [gm04009f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}