 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 1-2 REVIEW ARTICLE DEFINING A PHYSIOLOGICAL ROLE FOR THE TUBULIN TYROSINATION CYCLE Haitham T. Idriss Kimmel Cancer Center, Thomas Jefferson University Code Number: gm04010
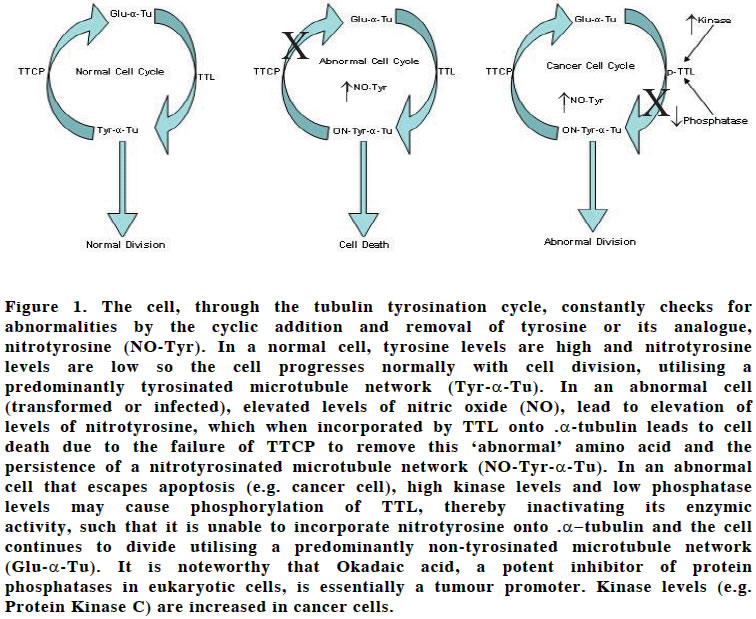
This paper proposes, based on data from other laboratories, that the physiological function of the tubulin tyrosination cycle is to maintain a check for normal physiological milieu within cells, whereby tyrosine and nitrotyrosine act as markers for normality and abnormality, respectively. Incorporation of nitrotyrosine is postulated to initiate apoptosis to facilitate elimination of abnormal cells. Key word: Tubulin tyrosination The tubulin detyrosination/tyrosination cycle is one of the first observed posttranslational modifications of a-tubulin. The modification involves the cyclic removal and re-addition of a tyrosine residues to the c-terminus of a-tubulin by the enzymes tubulin tyrosine carboxypeptidase (TTCP) and tubulin tyrosine ligase (TTL), respectively. No definite function has so far been attributed to this modification, but the majority of cytoplasmic microtubules consist of tubulin in the tyrosinated form (1). Recently, it has been demonstrated that nitrotyrosine is a substrate for TTL and is irreversibly added to the c-terminus of a-tubulin leading to microtubule dysfunction and cell death (2). A recent study contradicting this observation (3) most likely overlooked coordination between the tubulin assembly/disassembly, tubulin detyrosination/tyrosination and TTL dephosphorylation/phosphorylation cycles. I propose the physiological function of the tyrosination cycle is a check-point for abnormality in cells, whereby tyrosine and nitrotyrosine act as the markers for normality and abnormality and incorporation of nitrotyrosine initiates apoptosis to eliminate abnormal cells. Nitric oxide (and nitrotyrosine, a product of a biochemical reaction between NO and tyrosine) is elevated in abnormal cells such as cancer and/or infected cells. I previously hypothesised that cancer cells that are insensitive to the actions of TNF-a, may escape a-tubulin nitrotyrosination-mediated damage of microtubules (4). Recent studies showed that a major aspect of TNF-mediated cell cytotoxicity is the disruption of the cytoskeletal network, including microtubules (5). Interestingly, inhibition of protein kinases with H-7 potentiated TNF-mediated apoptosis, suggesting that depressed protein phosphorylation enhances TNF-mediated cell killing. Furthermore, microtubule disrupting drugs such as taxol also accelerated TNF-mediated cell-killing and somewhat enhanced the sensitivity of HeLa cells transfected with Bcl2 for apoptosis (5). I believe this supports the original hypothesis for the following reasons. H7 is likely to suppress the postulated phosphorylation of TTL, thereby preventing tubulin nitrotyrosination. Taxol have been shown to enhance apoptosis and cause hyperphosphorylation of the anti-apoptotic protein Bcl2 by activating protein kinase A, further accelerating cell death (6). This may also induce TTL phosphorylation (7), diminishing tubulin nitrotyrosination as a consequence. Therefore, microtubule damage, whether induced by taxol or mediated by the incorporation of nitro-tyrosinated tubulin seems to lead to apoptosis commensurate with the hypothesis that have been proposed herein. TTL may well turn out to serve an apoptotic role in abnormal cells. The tubulin detyrosination/tyrosination cycle may therefore serve as a biological sensor of cellular abnormalities using nitrotyrosine as a marker. I postulate, during each cell cycle detyrosination and re-tyrosination occurs through the actions of TTCP/TTL to serve this function. Once a cell becomes abnormal, TTL irreversibly adds nitrotyrosine, leading to microtubule dysfunction and leading to cell death e.g. through non- productive microtubule/microtubule-motor interaction. Only when hierarchical suppression of TTL function through phosphorylation, an abnormal cell propagates. This may therefore define the physiological role for the tubulin tyrosination cycle (figure 1). Cancer and/or infected cells most probably escape a -tubulin nitrotyrosination (8). REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04010f1.jpg] |
| |||||||||

{kind=link}