 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 3-5 REVIEW ARTICLE REMITTING SERONEGATIVE SYMMETRICAL SYNOVITIS WITH PITTING EDEMA (RS3PE) SYNDROME
AND MALIGNANCY
Mehmet Sayarlıoğlu Yuzuncu Yıl University, Faculty of Medicine,
Department of Internal Medicine, Division of Rheumatology Code Number: gm04011 Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome is a definite subset of the seronegative symmetrical polyarthritis of the aged, characterized by dramatic pitting edema of the hands, male predominance, old age and exquisite response to corticosteroids. RS3PE syndrome is a rare but well-defined syndrome known to be associated with solid tumors and haematologic malignancies. Recent research has shown that it is not a specific entity but rather a syndrome that can represent the inaugural form of various types of rheumatic disease and neoplastic conditions of the elderly. A thorough examination in elderly patients with RS3PE syndrome, and heightened suspicion of potential underlying malignant disease is necessary. In 1985, McCarty et al. (1) described first Remmitting Seronegative Symmetrical
Synovitis with Pitting Edema (RS3PE) syndrome which is characterized
by symmetrical distal synovitis, tenosynovitis of the mucous sheaths
of the flexor and extensor tendons of the hands, pitting edema of the
hands and/or feet, seronegativity for the Rheumatoid Factor (RF) and
benign prognosis, mainly affecting the elderly and the males, exquisite
response to corticosteroids, and long term remission after withdrawal.
There is no joint erosion. Magnetic resonance imaging studies have demonstrated
severe extensor tenosynovitis believed to be the principal lesion responsible
for the edema of the subcutaneous and peritendineous soft tissues of
the dorsum (2). Although the RS3PE syndrome appeared as a well characterized
entity, in the recent research has shown that it is not a specific entity
but rather a syndrome that can represent the inaugural form of various
types of rheumatic disease and neoplastic conditions of the elderly (3).
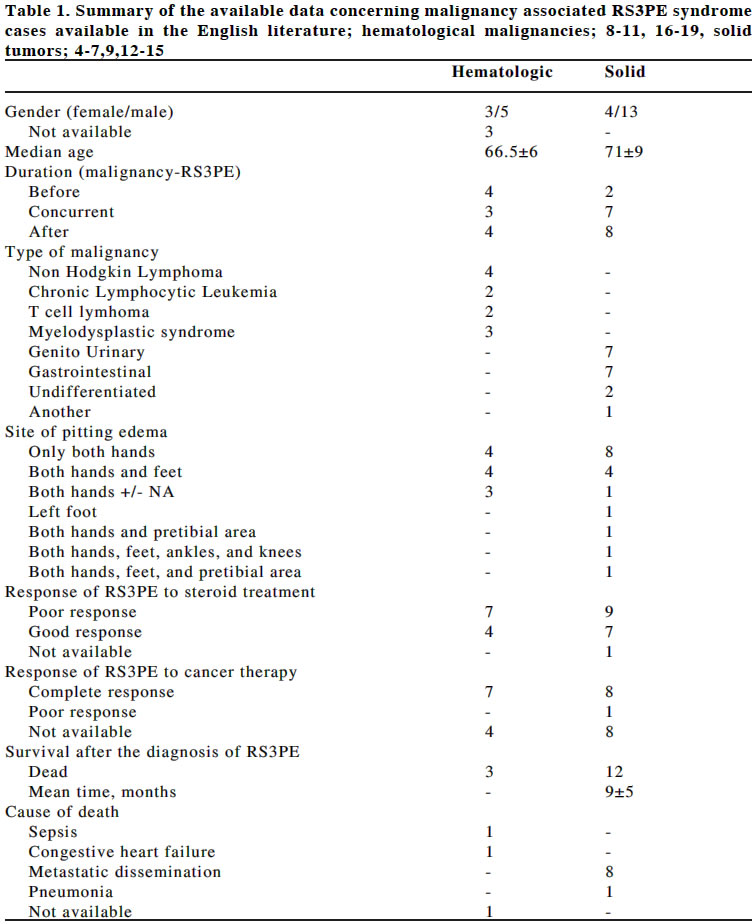
RS3PE syndrome has a good prognosis. Nevertheless, there have been reports of apparently classic RS3PE syndromes that were complicated by other rheumatic disease such as polymyalgia rheumatica and temporal arteritis, polyarteritis nodosa or other vasculitides, late onset rheumatoid arthritis, ankylosing spondylitis, acute sarcoidosis and spondyloarthropaties. RS3PE syndrome has also been described as a potential paraneoplastic condition in some recently documented cases (2-11). An association of the RS3PE syndrome with solid tumors such as prostatic, rectal, gastric, colic, endometrial, hepatocellular, ovarian, pancreatic, and undifferentiated adenocarcinoma and fibrohictiocytoma was reported (4-7,9,12-15). Among solid tumors seven gastrointestinal system and seven genitourinary system tumors, one fibrohistiocytoma in the iliac bone and two undifferentiated carcinomas were detected. In a few cases this syndrome was associated with haematologic malignancies. Among haematologic malignancies three with Myelodysplastic syndrome, four Non-Hodgkin’s lymphoma (NHL), two T cell lymphoma, and two chronic lymphocytic Leukemia (8-11,16-19) (Table). RS3PE syndrome mainly affects the males and the elderly. Its true incidence or prevalence is unknown. In table, RS3PE cases associated with solid and haematologic malignancies were summarized. In the cases of solid malignancies: female/male 4/13, median age 71±9(46-82). In the cases of haematologic malignancies: female/male 3/5, median age 66.5±6(60-75). RS3PE syndrome may represent a musculoskeletal manifestation of malignancies (7). In 53% of cases associated with solid tumors and 64% of cases with haematologic malignancies the diagnosis was established before or concurrently the diagnosis of RS3PE (Table). Response to steroid treatment for RS3PE was poor in 53% of cases with solid tumors and in 64% of cases with haematologic malignancies (Table). Patients with idiopathic RS3PE showed an excellent response to low doses of corticosteroids compared to the poor response of the RS3PE patients with associated neoplasia. In some reported cases while RS3PE was relieved with steroid treatment before treatment of malignancy (5,16-18), some others either did not respond to steroid treatment or recurred under this treatment (4,6-11,13,14). In almost all case reports with treatment response details available, after successful treatment of underlying malignancy complete recovery of the joint findings were noticed (4,9-12,14,17). In all but one distal swelling with pitting edema rapidly remitted, confirming the paraneoplastic nature of the condition. Since cancer is also common in the elderly, the association of RS3PE and malignancy may well be a coincidence. However, unlike several reports of RS3PE with a benign course and good response to low dose corticosteroid, RS3PE associated with cancer only seems to respond or resolve after successful treatment of the underlying malignancy. Thus in patients with RS3PE, in elderly who fail to respond to low dose steroid treatment, one must consider a paraneoplastic syndrome (13). Eleven cases with solid tumors were reported to be died (8 with metastases) 9±5 months after the diagnosis of RS3PE. Also three cases with haematologic malignancies were died after RS3PE (One case due to sepsis, other congestive heart failure and unreported reasons) (Table 1). Due to high rate of mortality after the appearance of RS3PE, presence of this syndrome may be considered as a bad prognostic factor for malignancies. In conclusion, RS3PE is a rare but well-defined syndrome known to be associated with solid tumors and haematologic malignancies. This possibility should be considered in the absence of other associated rheumatic conditions and resistance to corticosteroid therapy. Literature findings emphasize the need for a thorough examination in elderly patients with RS3PE syndrome, and heightened suspicion of potential underlying malignant disease. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04011t1.jpg] |
| |||||||||

{kind=link}