 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 6-10 ORIGINAL ARTICLE PHYSICAL ABUSE DURING PREGNANCY Metta Kuning1, Don McNeil2, Virasakdi Chongsuvivatwong3 Faculty of Science and Technology, Prince of Songkla University1,
Department of Statistics, School of Economics, Macquarie University2,
Epidemiology Unit, Faculty of Medicine, Prince of Songkla University3 Code Number: gm04012
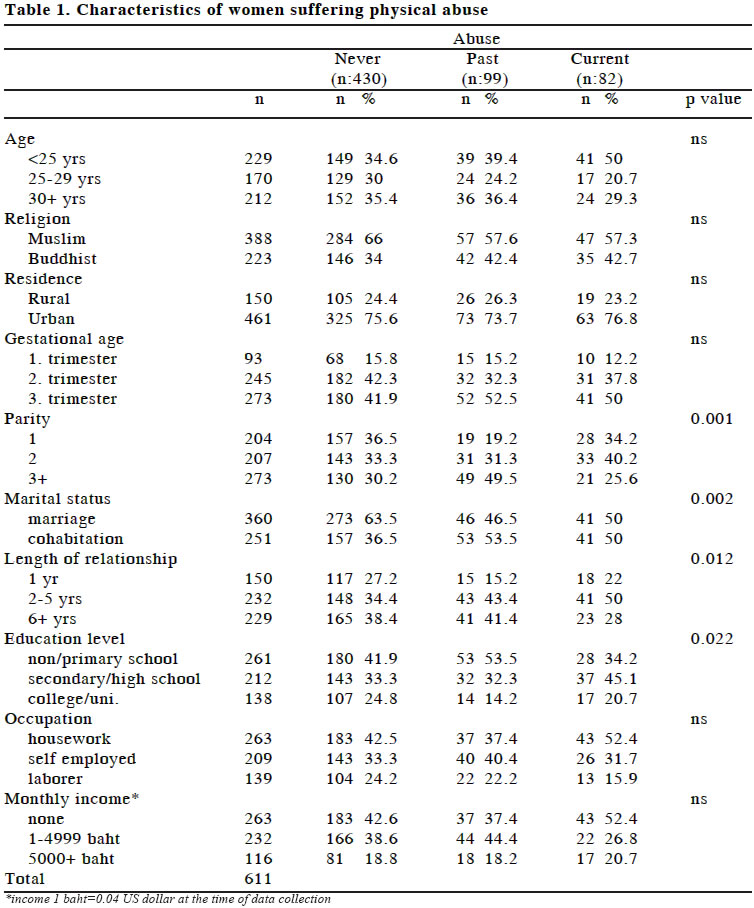
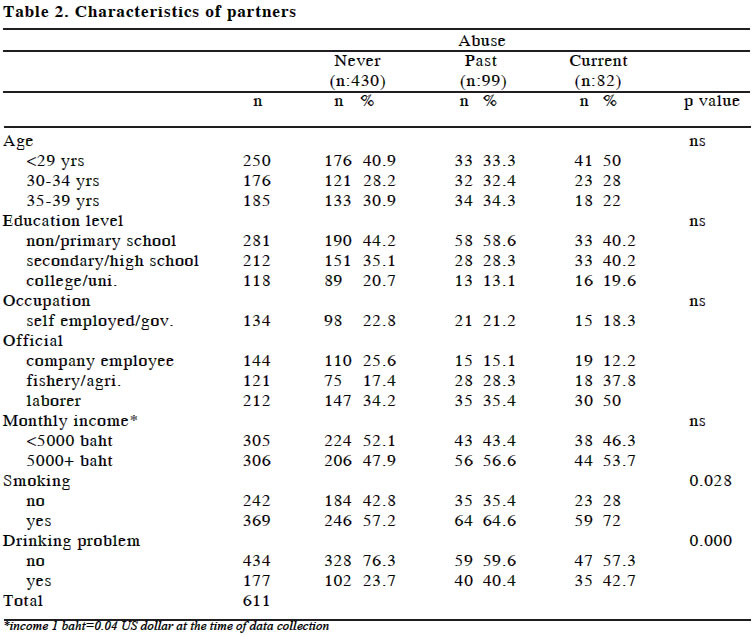
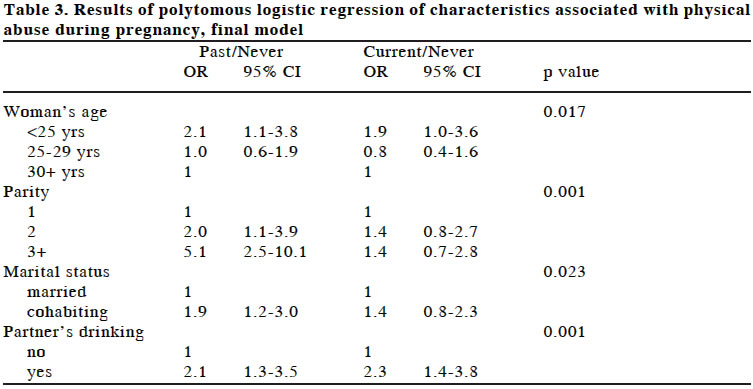
To study the prevalence and predictors of physical abuse among pregnant women in Pattani Hospital, Pattani, Thailand. A total of 611 women receiving antenatal clinic services through Pattani Hospital between July 1, 2002 and November 21, 2002 were interviewed. Information was collected on the women’s sociodemographic characteristics, experience of abuse, demographic characteristics of their partners, partner’s smoking habit and use of alcohol. The women’s experience of abuse was assessed by a questionnaire modified from the Abuse Assessment Scale (AAS). In all, 99 (16.2%) women reported experiencing past physical abuse (during a prior pregnancy or during the preceding year), 24 (3.9%) reported experiencing physical abuse during their current pregnancy, and 58 (9.5%) reported experiencing physical abuse both in the past and during their current pregnancy. Physical abuse was associated with parity, marital status, length of relationship, women’s education, smoking habit and the use of alcohol by their partner. After adjustment for confounding factors, the strongest risk factor for physical abuse during pregnancy was partner with a drinking problem. Women whose partner had a drinking problem were more likely to experience abuse during their current pregnancy than those whose partners did not have a drinking problem. In this study, one in eight pregnant women experienced physical abuse during current pregnancy. All types of abuse should be routinely ascertained in antenatal clinics. Key words: Physical abuse, pregnant woman, Thailand INTRODUCTION Intimate partner violence is not a new phenomenon and usually results in serious health problems in women. The World Health Organization (2002) reported between 10-69% of women had suffered from physical abuse at some point in their lives (1). The violence does not stop when a woman becomes pregnant, and between 0.9% and 20.1% during pregnancy (2). In fact, the frequency of the violence against pregnant women increases and becomes more severe during this period (3). As in many countries around the world, the issue of violence against women in Thailand is unknown in the public sphere. A World Bank-funded study reported that up to 20 percent of Thai husbands have beaten their wives at least once (4). However, the true rate of domestic violence in Thailand is likely to be much higher, because attitudes among the police, prosecutors, judges, society, and even the family of abused survivors encourage women to suffer in silence. In addition, most cases of violence are not reported due to the lack of an effective system of response. With no reliable statistics available, the severity and scope of the problem remains unclear. The combination of underreporting and poor statistical data has helped to limit awareness of the problem in the public sphere (5). The aim is to study the prevalence and predictors of physical abuse among pregnant women in Pattani. The results of this study would be useful for further planning to prevent physical abuse among pregnant women. MATERIAL AND METHOD Study area Pattani is a border southern province of Thailand. It consists of 12 district. The population was about 620,000 in 2002. Most (78%) are Muslim (6). Pattani Hospital is a major public hospital where 50% of pregnant women visit the antenatal clinic here (7). Subjects Sample size calculations were based on the main outcome of physical abuse. This calculation assumed that the prevalence of physical abuse during pregnancy was 14%. To estimate an odds ratio 1.5 with 80% power (5% type I error, two-tailed test) and a significance level set at 0.05, approximately 600 participants are required. Of 1275 pregnant women visiting the antenatal clinics at Pattani Hospital between July 1, 2002 and November 21, 2002, 611 pregnant women aged 15-45 years were randomly selected. The study was approved by the Ethics Committee of the Faculty of Medicine, Prince of Songkla University. Data collection A cross-sectional study was conducted. Verbal consent to participate in the study was obtained from women after assurance of interview confidentiality was given. All participants were interviewed by a designated research nurse in a private setting, in the absence of their male partners. Information was collected on sociodemographic characteristics for the women and their partners, smoking habit and the use of alcohol by their male partner, and the woman’s experience of physical abuse. The Abuse Assessment Scale (AAS) was used to assess the past and current abuse (8). The questionnaire was modified to evaluate the severity of violence. Emotional abuse, physical abuse, severe physical abuse and sexual abuse were observed. The periods of violence experience were also classified as in a prior pregnancy, in the last 12 months before the current pregnancy, and during the current pregnancy. Data analysis The probable determinants of interest are the women’s characteristics (age, religion, residence, gestational age, parity, marital status, length of relationship, educational level, occupation, and monthly income), and their partner’s characteristics (age, educational level, occupation, monthly incomes, smoking habit and drinking habit). The outcome was divided into 3 categories, namely: (a) non-abused, (b) past abuse and (c) current abuse. All the probable determinants of interest were categorical. Pearson’s chi-squared test and 95% confidence intervals were used to assess the associations between the outcome and the various determinants. Multivariate analyses was performed to investigate any independent associations between the predictor variables and physical abuse (both past and current abuse) using a polytomous logistic regression method. Stata software version 7.0 (STATA Corporation, College Station, Texas) was used for all analysis. RESULTS A total of 611 pregnant women consented to participate in the study and all were included in the analyses. Three groups determined by the Abuse Assessment Scale (AAS). Among them, 430 (70.4%) reported never being abused, 99 (16.2%) had a history of physical abuse, and 82 (13.4%) had suffered physical abuse during their pregnancy. The characteristics of the women are presented in Table 1. There were no significant differences between non-abuse, past abuse and current abuse with respect to age, religion, residence, gestational age, occupation, and monthly income. Women with parity greater than two were more likely to have been abused in the past. There was a significantly greater representation of women living in de facto relationships in both the past abuse and current abuse groups. There was a higher proportion of women suffering the past abuse and current abuse who had a relationship between two and five years. Women with a lower educational level were significantly more likely to suffer past abuse. Regarding the characteristics of partners (Table 2), no associations were found between physical abuse and age, educational level, occupation, and monthly income. Women living with a partner who smoked or had a drinking problem were likely to suffer from both past abuse and current abuse. Table 3 gives the results after fitting a multiple logistic regression model to the data with all determinants included, and then reducing the model by eliminating determinants with p-values above 0.05, using backward elimination. The outcome was divided into three groups, giving two sets of odds ratios, corresponding to women having past abuse and women experiencing physical abuse during pregnancy. The baseline outcome was never having been abused. For the comparison between past abuse and non-abuse, parity and marital status were associated with past physical abuse after adjusting for the other determinants. Women aged less than 25 were more likely to suffer past abuse (OR 2.1, 95%CI 1.1-3.8). The risk of past abuse increased with parity. Women living in de facto relationships had a higher risk of physical abuse in the past than married women (OR 1.9, 95%CI 1.2-3.0). The risk associated with past abuse was higher for women whose partner had a drinking problem (OR 2.1, 95%CI 1.3-3.5). For the comparison between current abuse and non-abuse, there was no evidence that the woman’s age, parity or marital status were associated with abuse. However, the risks associated with current abuse were high for women whose partner had a drinking problem (OR 2.3, 95%CI 1.4-3.8). DISCUSSION This research studied the prevalence and predictors of physical abuse among pregnant women in Pattani Hospital, Pattani, Thailand. We found that physical abuse among pregnant women by an intimate partner was not rare. The prevalence was 16.2% for past abuse and 13.4% for women suffering physical abuse during their current pregnancy. Compared with other studies (9-13) of similar population, the prevalence of physical abuse during current pregnancy was high. The estimated prevalence of domestic violence depends on the study design, definitions of violence, methods and techniques of data collection, and cultural differences (12,13). However, fear and embarrassment might result in underreporting of abuse. Our study attempted to increase the confidentiality of women’s responses to sensitive question about violence in an intimate relationship by conducting interviews in private. In addition, the interviewers were all antenatal care nurses. However, other biases are likely to occur, including recall bias, selection bias, and misclassification bias. An association was found between physical abuse and parity. Victims of violence had higher parity. This is in accordance with the studies of Berenson (10) and Muhajarine (11). Moreover, Webster (14) reported that the severity of abuse increased with parity. In contrast Hedin (15) found no evidence that parity was associated with physical abuse. We suggest that parity could be associated with abuse because it is linked to economic problems. Women living in a de facto relationship were twice as likely to have been abused. These findings are similar to those reported in other studies (10,11,14-17) and suggest that couples living in a de facto relationship may not be prepared to acknowledge that their relationship is abusive or unstable. The association between the woman’s age and physical abuse is not consistent with previous studies. Webster (14) found that the prevalence of abuse decreased with age whereas others found no association with age (11,15-17). Our study found that age was a confounder. As found in some studies (11,15), partners having a drinking problem was associated with physical abuse, although this contrasts with findings of Berenson (10) and Webster (14). Women living with a partner who had a drinking problem were approximately 2 times more likely than others to suffer violence, and religion was an effect modifier in this association. In conclusion, the prevalence of physical abuse was high in Pattani. The characteristics of victims were higher parity, living in a de facto relationship, and partner having a drinking problem. Antenatal nurses and clinicians should be aware of these risk factors. The violence issue should be addressed in the antenatal clinic. Screening could help clinicians to avoid complications. ACKNOWLEDGEMENTS We would like to thank the staff of the antenatal clinic at Pattani Hospital for assistance with our study. This study was supported financially by the graduate school, Prince of Songkla University and Ministry of University. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04012t3.jpg] [gm04012t1.jpg] [gm04012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}