 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 11-14 ORIGINAL ARTICLE ANTITHYROID ANTIBODY LEVELS IN PATIENTS WITH BREAST CANCER Haluk Dülger1, Süleyman Alıcı2, Ekrem Algün3, Ömer Etlik4, Mehmet Sayarlıoğlu5, Ekrem Doğan5, Hayriye Sayarlıoğlu5, M. Ramazan Şekeroğlu1 Yüzüncü Yıl University, Faculty of Medicine, Departments
of Biochemistry1, Medical Oncology 2, Endocrinology3,
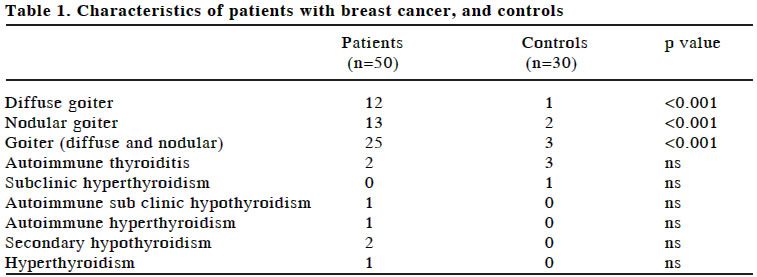
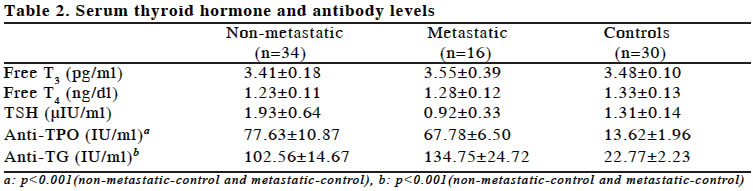
Radiology4 and Internal Medicine5 Code Number: gm04013 Breast cancer is a hormone-dependent neoplasm. Conflicting results regarding the clinical correlation between breast cancer and thyroid diseases have been reported. The aim of this study was to determine the goiter prevalence, thyroid hormones and antithyroid antibody levels in patients with breast cancer. For this purpose, thyroid ultrasonography was performed and serum levels of free triiodothyronine (FT3), free thyroxine (FT4), thyroid-stimulating hormone (TSH), anti-thyroid peroxidase antibodies (anti-TPO ab) and anti-thyroglobulin antibodies (anti-TG ab) were determined in 50 operable breast cancer patients at the time of diagnosis and 30 healthy individuals as control group. Goiter prevalence was found to be significantly higher in the study group (50% vs 10%). FT3, FT4, and TSH levels of patients were not different compared to controls, whereas anti-TPO ab and anti-TG ab levels were significantly higher in patients than in the control group. In conclusion, goiter prevalence and thyroid antibody levels were found to be increased in breast cancer patients and thyroid functions should be monitored. Key words: Breast cancer, thyroid peroxidase, thyroglobulin antibodies INTRODUCTION Breast carcinoma affects millions of women every year. Some studies suggested an association between breast carcinoma and thyroid diseases, including thyroid carcinoma. Both diseases occur primarily in women and some studies imply that their coexistence in women may be more than chance. The potential impact of treatment of one disease for the development of the other remains unclear (1-5). It has been demonstrated that a direct relationship between thyroid enlargement and breast carcinoma exists (6). An association between autoimmune thyroid disease and breast carcinoma were reported (7,8), but this was not confirmed in other studies (9). Higher frequency of thyroid peroxidase antibodies (TPO Ab) in breast carcinoma patients, compared with control groups were also reported (10); and, more recently, it has been demonstrated (5) that there was an overall increased prevalence of both thyroid disorders and TPO Ab in patients with breast carcinoma (11). In our region a high prevalence of goiter was reported (12). This condition may be related to hormone dependent neoplasms. The aim of this study was to determine the thyroid hormones and antithyroid antibody levels in patients with breast cancer, and whether there is a relationship between their levels and breast cancer. MATERIAL AND METHODS A total of 50 women with breast cancer were enrolled to the study. In all patients diagnosis was histologically or cytologically proven and type of malignancy was invasive ductal carcinoma. The patients were recruited before any treatment (chemotherapy, radiotherapy or surgery). At the first admission patients were divided into two groups according to presence or absence of distant organ metastasis. For patients without distant organ metastasis radical mastectomy and axillary lymph node dissection was performed. Median age of the study group was 40 (range 24-65). Thirty voluntary healthy age-matched (median age 45, range 27-73) women were selected as controls (p>0.05). Ultrasonography was performed in all patients by an experienced radiologist using 7.5 MHz annular array probe (Toshiba SSA-220A, Tokyo, Japan). The patient was supine with neck hyperextended during the ultrasonography examination. Ultrasonography scans were obtained in transverse, longitudinal and multiple oblique planes. The echo texture, border, nodule, and size of thyroid gland were determined on sonographic examination. A total of 5 ml of venous blood was drawn from each subject. Blood samples were then centrifuged at 2000 rpm for 10 min in a refrigerated centrifuge to separate serum samples from the cells. Serum levels of free triiodothyronine (FT3), free thyroxine (FT4), thyroid-stimulating hormone (TSH), anti-thyroid peroxidase antibodies (anti-TPO ab) and anti-thyroglobulin antibodies (anti-TG ab) were determined by using the commercial IMMULITE kits, which are solid-phase, two-site chemiluminescent immunometric assays (Immullite, DPC, USA). Statistical analysis Kolmogrov-Simirnov Goodness of fit test was used to control whether the distribution of parameters are normal or not. Some of parameters had not normal distribution. Thus, groups were compared with the Kruskal-Wallis test, followed by Mann-Whitney U tests for serum thyroid hormone and antibody levels. Also chi-square analysis was performed to compare the groups. Results were given as mean with standard error (SE). RESULTS The clinical and ultrasound evaluation of thyroid gland and thyroid function parameters were given in Table 1. In breast cancer patients, diffuse goiter was identified in 12 cases and nodular goiter in 13 cases. In the control group, diffuse goiter was identified in one patient and nodular goiter in 2 patients. Serum thyroid hormone and antibody levels for metastatic and non-metastatic cancer groups and controls were shown in Table 2. The mean value for serum TPO antibodies and thyroglobulin antibodies were significantly higher for breast cancer patients (for both metastatic and non-metastatic groups). DISCUSSION The relationship between breast cancer and thyroid disease is a matter of controversy. Thyroid function, thyroid antibodies, and clinically relevant thyroid diseases were investigated in several series of patients with breast carcinoma (5,6,13). Although associations with hyperthyroidism, hypothyroidism, thyroiditis and nontoxic goiter have been reported in the literature, no convincing evidence exists of a causal role for overt thyroid disease in breast cancer. Geographical variations in the incidence of breast cancer have been attributed to differences in dietary iodine intake, and an effect of iodine on the breast has been postulated (8,13). The possible interactions between thyroid gland and breast tissue are based on the common property of the mammary and thyroid epithelial cell to concentrate iodine by a membrane active transport mechanism as well as on the presence of TSH receptors in fatty tissue, which is abundant in mammary gland (5,14). Additionally, some endocrine stimuli identified in thyroid products that exert a simultaneous action on the breast and the various thyroid antibodies, which could also interact with receptors on breast tumors, have been postulated to be responsible for the coincidence of mammary and thyroid gland disorders (12,15). Our results indicate an increased prevalence of goiter in patients with breast cancer. The presence of goiter was assessed by ultrasound thyroid examination, which provides an objective means for the evaluation of thyroid size. Higher frequency of thyroid peroxidase antibodies (TPO Ab) in breast carcinoma patients, compared with controls, has been reported and it has been demonstrated that there was an overall increased prevalence of both thyroid disorders and TPO Ab in patients with breast carcinoma (5,11,13). It has been proposed that the presence of thyroid abnormalities may influence breast cancer progression (11). Smyth et al. (11) suggested a better prognosis for breast cancer among patients with increased levels of TPO. It has been proposed that the immune response might be directed both by tumor and by thyroid tissue, or that the tumor and thyroid tissue share common properties, as they both express TPO and the sodium iodide symporter gene (16,17). The sodium iodide symporter (NIS) is a plasma basolateral membrane protein that actively transports iodide to the thyroid follicular cells as the first step of thyroid hormone biosynthesis. NIS also mediates active iodide transport in other human tissues including salivary glands, lactating mammary gland and gastric mucosa (18.19). NIS expression has been recently reported also in several other human tissues but its physiological role is still unclear. Cloning of the NIS gene and the development of specific NIS antibodies have allowed the characterization of the pathogenic role of NIS in thyroid cancer, thyroid autoimmune diseases, congenital hypothyroidism and other, non-thyroidal human diseases. The possibility to increase its levels of expression or to reinduce its expression in thyroid carcinomas that have lost the ability to take up radioiodine is one of the most promising clinically related field of research (18). Although high TPO level has been shown to be a very important factor in antibody-dependent cell cytotoxicity in the thyroid, and there may be a possible association between autoimmune thyroiditis and the immune system, there is no agreement on the significance of its association with breast cancer (13). Present study confirms recent reports of higher TPO Ab positivity in women with breast carcinoma. An increased prevalence of TPO Ab was demonstrated previously (5,10,11,13). Additionally, in this study, it has been shown that not only serum TPO antibody levels but also thyroglobulin antibodies were higher in breast cancer patients than controls. In conclusion, our results showed that in patients with breast cancer, prevalence of goiter and thyroid antibodies were elevated and the thyroid functions of these patients should be monitored. The clinical importance and meaning of this condition should be investigated prospectively in large cohorts. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04013t1.jpg] [gm04013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}