 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 25-31 ORIGINAL ARTICLE COMPARISON OF THE EFFECTS OF METFORMIN AND GOSERELIN IN PATIENTS WITH POLYCYSTIC OVARY SYNDROME Ayfer Bala, Kazım Gezginç, M. Nedim Çiçek, Cemalettin Akyürek Selçuk University, Faculty of Meram Medicine, Department of Obstetrics
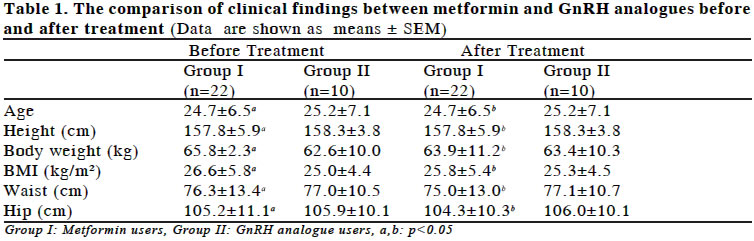
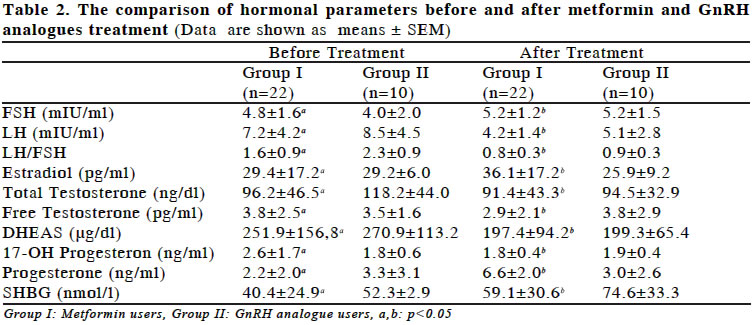
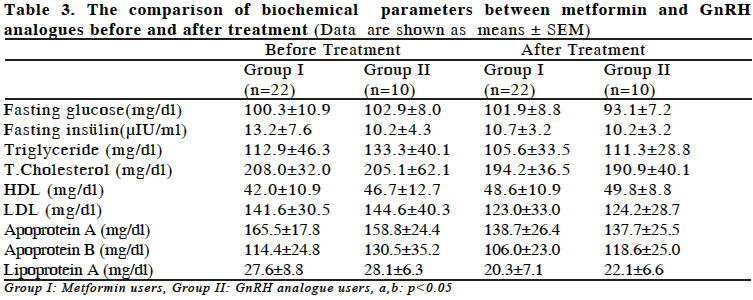
and Gynecology Code Number: gm04016 The aim of this study was to compare the effects of metformin and GnRH analogues on lipid metabolism and hormonal parameters in women with polycystic ovary syndrome (PCOS). The study population consisted of 40 women with PCOS. Patients were divided into two groups. Metformin (850 mg, two times per day) was administered to the first group and GnRH analogue (goserelin 3.6 mg, every 28 days) was given to the second group. Only 32 women completed the study and their results were evaluated. Insulin resistance was not ascertained in patients. Metformin treatment resulted in a significant decline in mean body mass index, body weight and circumferences of waist and hip. In addition, there was a significant decrease in LH levels and a significant increase in FSH, progesterone and sex hormone binding globulin (SHBG) concentrations. Although there was an improvement in lipid abnormalities, no changes in starving glucose and insulin levels were observed. GnRH analogue resulted in a significant increase in FSH and SHBG levels and a significant decrease in LH, total testosterone, DHEAS levels and LH to FSH ratio. In patients treated with GnRH analogue, there was an improvement in lipid metabolism but there was no change in clinical features. Metformin and GnRH analogue use appears to improve endocrinological features and lipid abnormalities which consequently result in cardiovascular diseases in PCOS, independent from insulin resistance. Key words:PCOS, metformin, GnRH analogue, hormones, lipid metabolism. INTRODUCTION PCOS is a common clinical condition that occurs about 5% to 10% in women of reproductive age (1). The association of amenorrhea with bilateral polycystic ovaries was first described in 1935 by Stein and Leventhal (2). Although there was a lot of study, its etiology remains unknown. PCOS is diagnosed if there are any two of the following; presence of polycystic ovaries on ultrasound examination, clinical or biochemical evidence of hyperandrogenism and menstrual dysfunction with anovulation (3). PCOS is characterized by increased androgen production, oligomenorrhea or amenorrhea, infertility, hirsutismus and obesity (4). In addition to reproductive consequences of the syndrome, metabolic disorders such as peripheral insulin resistance, hyperinsulinemia, hypertension and lipid abnormalities are also characteristics of PCOS. Some studies suggest that PCOS may increase the risk for several conditions, including type II diabetes mellitus and cardiovascular disease (5). Intraovarian autocrine and paracrine regulators, especially the insulin like growth factor (IGF) system is thought to have an important role, both in normal and polycystic ovary. IGFs and insulin together play a critical role in modulating gonadotropin-mediated folliculogenesis and steroidogenesis. Circulating levels of IGFs are not associated with menstruation although follicular fluid concentrations of IGFs exhibit variation. This feature shows the importance of IGF system in modulating ovarian functions (6). Because of the structural similarity of insulin and IGF receptors, at higher concentrations, insulin binds to IGF receptors. Activation of IGF receptors by insulin would lead to increased androgen production in thecal cells (7). There are two other important actions of insulin which contribute hyperandrogenism in the presence of hyperinsulinemia: inhibition of hepatic synthesis of sex hormone-binding globulin (SHBG) and inhibition of hepatic production of IGF binding protein (8). Insulin help IGF system and strengthen their effects (9). After the investigation of metabolic abnormalities in PCOS, medications that improve insulin resistance by reducing serum insulin levels, have been administered to women with PCOS (5,10). The purpose of our study was to compare the effects of GnRH analogues and metformin in hormone levels and lipid profile in PCOS and to pay attention to increased risk of cardiovascular disease. MATERIAL AND METHODS This study was performed with 40 women, aged 18-42, who had any two of the following; presence of polycystic ovaries on ultrasound examination, clinical or biochemical hyperandrogenism, menstrual dysfunction with anovulation. Patients were selected randomly. Informed consent was obtained from all women before the study and study received the approval of the Human Ethics Committee of the Medical Faculty, Selçuk University. The patients with adrenal, thyroid, pituitary and hypothalamic endocrinologic disorders, diabetic patients were excluded from the study. Hormone measurements were performed on the second or third days of spontaneous menstrual cycle or withdrawal bleeding. FSH, LH, LH/FSH ratio, estradiol, total testosterone, free testosterone, DHEAS, 17-OH progesterone and SHBG levels were measured and recorded. Progesterone levels were measured and recorded between 21st to 23rd days of menstrual cycle. Hirsutismus was evaluated by determination of androgen sensitive regions of the body as Ferriman Gallwey scores by the same clinician (11). All patients had total hirsutismus scores of 12 or over. Anthropometric measurements were made prior to treatment and at the end of treatment by the same observer. Body weight, height, waist and hip circumferences were measured. Obesity was defined by a cut-off value of 27kg/m² (12). After an overnight fast, glucose, insulin, triglyceride, HDL, LDL, total cholesterol, apoprotein A and B, and lipoprotein (a) levels were measured and recorded. Insulin resistance was detected by using the fasting glucose/insulin ratio. Below 4,5 was considered as an insulin resistance (13,14). In the first group, patients were received metformin 850 mg twice daily (Glucophage retard tb, İlsan, İstanbul, Turkey). In the second group, patients were received goserelin 3.6mg/28 day, IM injection (Zoladex, Astra Zeneca, Istanbul, Turkey). In the first group, 3 of 26 patients were excluded from the study because of gastrointestinal side effects and in the second group 4 of 14 patients because of their own desire were abandoned the study. During the study, a patient who received metformin, conceived and withdrew from the study at the 7 th week after pregnancy. Twenty two patients in the first group and 10 patients in the second group, totally 32 patients completed the study and their results were investigated for the study. The patients evaluation after the treatment was made in the early proliferative period of the first spontaneous menstrual cycle after the treatment. The patients menstrual cycles restarted between 1st and 6th month of the last treatment. The duration for spontaneous cycle after treatment were not considered in the study. Parity and infertility were not evaluated because half of the patients were virgin. Ultrasonography was performed with Hitachi 3.2 EUB 3.5 mHz convex probe for abdominal examination and 5 mHz vaginal probe in early follicular phase. Statistical analysis was performed using Mann-Whitney U test and Wilcoxon signed Rank test with SPSS software. P<0.05 was accepted as statistically significant. RESULTS The mean age (24.7±6.5 and 25.2±7.1 years) and body Mass Index (BMI) before treatment (26.6±5.8 and 25.0±4.4kg/m²) were similar in group I and II, respectively. In group I, there were 5 and in group II there were 4 obese (BMI>27kg/ m²) patients. There were no statistically significant difference between two groups for several variables including height, body weight, BMI, waist and hip circumferences before treatment (p>0.05). When two groups were compared after the treatment, there were not statistically significant differences between the groups in terms of clinical manifestations (p>0.05). Clinical characteristics of the patients before and after treatment were presented in Table 1. All of the endocrine characteristics also were similar before the treatment between two groups (p>0.05). At the end of the study plasma concentration of progesterone in group I were higher than group II and this difference was statistically significant (p<0.05). There were no significant differences in the levels of FSH, LH, estradiol, total testosterone, free testosterone, DHEAS, 17-OH progesterone, SHBG and LH/FSH ratio after the medical treatment (p>0.05). Table 2 shows the serum FSH, LH, estradiol, total testosterone, free testosterone, DHEAS, 17 OH progesterone, SHBG levels and LH-FSH ratio before and after treatment. None of the patients had hyperinsulinemia and insulin resistance. fasting glucose and insulin concentrations were 100.3±10.9 mg/dl and 13.2±7.6 µIU/ml in group I and 102.9±8.0 mg/dl and 10.2±4.3 µIU/ml in group II. These results also showed no significant differences. There were no significant differences between two groups concerning triglyceride, total cholesterol, LDL cholesterol, HDL cholesterol, apoprotein A, apoprotein B and lipoprotein (a) levels (p>0.05). There were no significant differences between two groups in biochemical parameters after the treatment except fasting glucose levels (p>0.05). In group II, the concentration of fasting glucose was higher than group I and it was statistically significant (p<0.05). Table 3 summarizes some biochemical parameters of the patients of two groups before and after the treatment. In addition to compare the results between the two groups, also the baseline and the after treatment findings are compared within the groups separately. In metformin treated patients, there were significant differences concerning body weight, BMI, waist and hip circumferences. After the treatment these variables were lower than baseline (p<0.05). There were no significant differences in clinical characteristics in group II (p>0.05). After the metformin treatment, LH levels decreased and FSH, progesterone and SHBG levels increased significantly (p<0.05). GnRH analogue treatment made significant improvements in endocrine profiles. At the end of the treatment, in this group, the levels of LH, total testosterone, DHEAS and LH-FSH ratio were decreased and the levels of FSH and SHBG were increased. These were statistically significant (p<0.05). Biochemical values were improved by metformin treatment. There was an increase in the level of HDL cholesterol and a decrease in LDL cholesterol, apoprotein A, apoprotein B and lipoprotein (a) levels (p <0.05). In this group no statistically significant differences were recorded in fasting glucose and insulin concentrations (p>0.05). GnRH analogue treatment was also associated with an improvement in biochemical parameters. The latter values of fasting glucose, triglyceride, apoprotein A and lipoprotein (a) concentrations were significantly decreased (p <0.05). DISCUSSION In this study, two different medical agents were used in women with PCOS. We evaluate the endocrinological and biochemical effects of these two medications. Obesity has been defined by a cut-off value of 27kg/m² in studies for many years (12). In this study there were 5 obese patients in group I and 4 obese patients in group II. The prevalence of obesity that we found was slightly lower (31.2%) than the prevalence reported by Laure et al (35-60%) (12). The mean BMI of two groups were beneath 27 kg/m ². There was no significant difference in terms of BMI. The similarity of BMI values has excluded the effects of obesity in the study. The prevalence of insulin resistance detected by using different screening method has been reported as 40% to 70% approximately. In our study, no patient had insulin resistance which was detected by using the glucose /insulin ratio (13). This discordance is probably due to the lower sensitivity of the glucose /insulin ratio compared with the euglycemic clamp technique and CIGMA test (12,15). In a study, the glucose/insulin ratio has been correlated with insulin sensitivity measured by using euglycemic clamp, the minimal model technique and oral glucose tolerance test (13). In contrast, result of another study (16) failed to demonstrate the correlation between euglycemic clamp technique and CIGMA test. The hyperinsulinemic euglycemic clamp technique is considered to be the gold standard for evaluation of insulin sensitivity. However the procedure is expensive, invasive and time consuming. In the present study, we aimed to define insulin resistance with glucose/insulin ratio which is more practical than the others and easily applicable in medical centers. We decided to treat patients with metformin although we did not ascertain insulin resistance, depending only on the patients clinical diagnosis of the PCOS. The discordance for the prevalence of insulin resistance may be due to the lower prevalence of obesity. Some authors demonstrated a correlation between insulin resistance and obesity, and their results confirmed earlier contentions (12). In contrast, some investigators reported that obesity did not coexist with alteration of insulin secretion and insulin resistance (17). These differences may be due, at least in part, to heterogeneity of the populations studied and study protocols. In this study, the weight-loss after the use of metformin was a secondary effect of metformin by inhibiting intestinal glucose absorption. Independent from PCOS, the obesity is associated with hyperinsulinemia and hyperandrogenism. The best treatment for women with PCOS is weight loss which reduces androgen levels (6,10,18). Weight–loss was suggested as a first line treatment for women with PCOS with an elevated BMI in the treatment of infertility (19). Studies have shown that as little as 5% loss of total body weight is often associated with an increased numbers of ovulatory cycles. A rapid improvement in hyperandrogenism, a decrease in BMI and weight-loss has been demonstrated with metformin treatment in women with PCOS (20). Not all studies have shown an effect of metformin treatment on body weight in women with PCOS. Some authors have reported no significant decrease in body weight, BMI, circumferences of waist and hip after metformin treatment (21). More investigators have studied the effects of GnRH analogues in PCOS. Especially the alterations in androgen levels, hirsutismus score and insulin resistance have been elevated (22,23,24). But there are not enough and appropriate clinical trials to confirm the effect of GnRH analogues on clinical features among women with PCOS. In our study, metformin increased serum progesterone levels significantly. This alteration in the level of progesterone was similar to other studies. It has been reported that a significant number of anovulatory women ovulate and achieve pregnancy by metformin treatment (25). In this study, one patient conceived during treatment and withdrew from the study at the 7th week of her pregnancy. Her pregnancy continues healthy, fetal development is in normal range, and the results of triple test and amniocentesis is normal. Some investigators demonstrated that metformin had beneficial effect abnormal ovarian function and steroid metabolism in hyperandrogenic women with PCOS. A significant decline in both testosterone and LH concentrations and an increase in ovulation rate had been recorded. Ovulation had been considered to be occurred when the serum progesterone was greater than 3,5 ng/ml in luteal phase (26). Kolodziejczyk et al. (20) had reported that metformin treatment resulted in a significant decrease in total testosterone and a significant increase in SHBG. According to the authors, responses to metformin were related to the severity of the hyperandrogenemia. Subjects with elevated DHEAS had exhibited less improvement than subjects with normal DHEAS. In this study, in metformin treatment group, the association of the improvement in endocrine features to weight-loss could not be distinguished particularly from each other because we did not investigate insulin resistance and we did not record an alteration in fasting insulin and glucose concentrations after metformin treatment. In this group, although there was not a significant decrease in androgen levels, because of the improvement in FSH and LH levels, different mechanisms were thought to be effective other than weight-loss. In previous study, GnRH analogues resulted in increase in FSH, SHBG levels and decrease in LH, LH to FSH ratio, total testosterone, DHEAS levels. By decreasing LH concentrations a decrease in total testosterone levels was observed. But we could not explain the effects of GnRH analogues on DHEAS levels which is secreted by adrenal cells. Shaw et al (27) reported that GnRH analogues ascertained a significant decrease in LH, estradiol, testosterone and androstenedion. Following cessation of GnRH analogue treatment serum LH, estradiol, total testosterone levels had again begun to increase and after treatment reached to pretreatment values. Some authors (23,24) had demonstrated that GnRH analogues treatment resulted in decrease in LH, estradiol and androgen levels. On the basis of the theory that insulin may be an important contributor to the pathophysiology of PCOS, it is postulated that insulin sensitizers might improve the endocrinologic and biochemical imbalances and clinical features associated with PCOS. Metformin lowers blood insulin and makes an improvement in insulin resistance. It impedes androgen biosynthesis which is promoted by hyperinsulinemia (20,28) Previous studies on the effects of metformin on PCOS have produced conflicting results. Although most of the reports described an improvement in insulin resistance in PCOS, others failed to observe a statistically significant effect in insulin resistance (29,30).These differences may be due to heterogeneity of the populations studied (genetic basis, the dose of treatment, study protocols and etc.) Gonadal steroids are believed to influence glucose metabolism, estrogens induces improvement and androgens or progestins cause deterioration. Because of these informations it has been postulated that, in women with PCOS, the enhanced levels of androgens may induce insulin resistance. However, studies evaluating the role of androgen suppression on glucose metabolism of women with PCOS have obtained conflicting results, and either no effect or improvements have been reported. Furthermore, the GnRH analogues induced reduces gonadal estrogen by eliminating their possible beneficial effects on glucose metabolism may have counterbalanced the eventual advantages deriving from androgen suppression. In our study, GnRH analogues induced a decline in fasting levels of glucose but not of insulin. We could not explain exactly the mechanism and the reason of this decline. Cagnacci et al. (15) studied effects of ovarian suppression with GnRH analogue on glucose metabolism in women with and without ovarian hyperandrogenism. They demonstrated that strong suppression of ovarian activity improves peripheral insulin sensitivity while it is without relevant effects on glucose metabolism of non-hyperandrogenic women. Hypertension and lipid abnormalities are responsible for the increased risk of cardiovascular disease in women with PCOS. Compared with normally cycling controls, women with PCOS have been noted to have significantly higher levels of total cholesterol, LDL cholesterol and triglyceride and lower levels of HDL cholesterol. Dyslipidemia which is a consequence of hyperandrogenism, is known to vary directly with hyperinsulinemia, obesity and increased waist to hip ratio (10). In PCOS high levels of lipoprotein (a) and apoprotein A have been noted which are responsible from atherosclerotic cardiovascular disease and low levels of apoprotein B (10,31). Relative estrogen insufficiency and androgen excess have also been linked to increased risk of cardiovascular heart disease (10,31). However the data were insufficient to determine the effects of medical agents which were used for the treatment of PCOS on lipid abnormalities. In our study, we observed an improvement in lipid abnormalities with metformin and GnRH analogue treatment. Metformin treatment resulted in increased levels of HDL cholesterol and decreased levels of lipoprotein (a), apoprotein A and B and LDL cholesterol. We suggest that although there were no significant improvement in hyperandrogenism, weight-loss, decreased levels of estrogen and suppressed androgen secretion, may be responsible for the improvement in lipid metabolism. There were significant decreases in serum levels of lipoprotein (a), apoprotein A and triglyceride in GnRH group, after treatment, possibly because of suppression of androgens. For the treatment of PCOS, we are using different medical agents which have special and different activities according to patient’s main complaint and desires. Close follow- up of women with PCOS and encouragement of lifestyle practices likely to reduce disease risks should be the standard practice. The present data demonstrate that metformin and GnRH analogues are effective and safe for the treatment of endocrine and biochemical characteristic of PCOS. Because of their different mechanisms, we do not prefer one of them as more effective than the other. Individual treatments should be planned for patients with PCOS. Since GnRH anologues are expensive compared with metformin and since they lead to medical menapause and ostoporosis in their prolonged used, these are accepted as disadvantages of GnRh analogues. It is known that most of the patients with PCOS are infertile so to put these patients into menapause is another disadvantage. In conclusion, we demonstrated an improvement in endocrine and lipid abnormalities with metformin, an insulin sensitizing agent and ovarian suppression with GnRH analogues. The exact mechanism by which GnRH analogues and metformin can improve these features is poorly understood. Long-term prospective studies are needed to better delineate the nature of PCOS and to investigate the role of established and emerging PCOS therapies, including insulin sensitizers and GnRH analogues. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04016t2.jpg] [gm04016t1.jpg] [gm04016t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}