 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
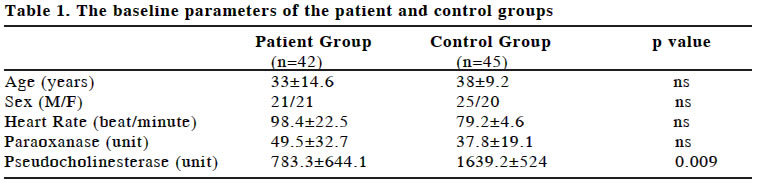
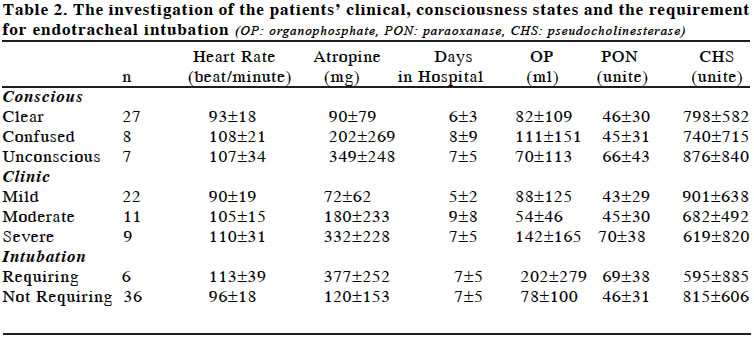
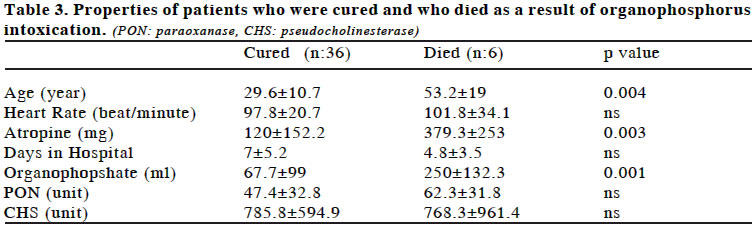
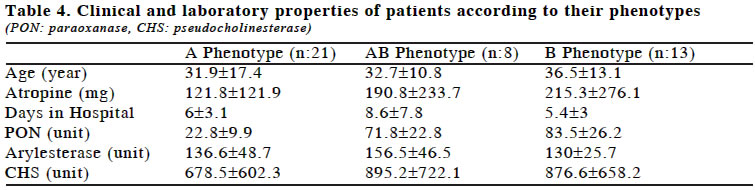
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 32-37 ORIGINAL ARTICLE THE RELATIONSHIP OF CLINICAL SIGNS WITH THERAPY AND BIOCHEMICAL PARAMETERS IN PATIENTS WITH ORGANOPHOSPHATE INTOXICATION Mehmet Tanrısev, Ömer Toprak Department of Third Internal Medicine, Ataturk Training and Research Hospital Code Number: gm04017 Organophosphate containing insecticides, especially those widely used in the agricultural field, have harmful effects on human. In this study, our aim was to study the relation among clinical and laboratory findings and the parameters such as amount of organophosphate, serum paraoxanase (PON) and pseudocholinesterase (CHS) concentration and the phenotype of PON, in patients with pesticide intoxication. Forty two patients with organophosphate intoxication (OPI) and 45 healthy volunteers as control were included in this study. Patients were divided into groups according to the severity of their clinical conditions and treated after vital examinations and routine blood tests were done. Serum PON activity, arylesterase activity, PON phenotype determination and acetylcholinesterase activity tests were carried out for both the patient and the control groups. No statistical difference was detected in either group in terms of basal PON values and phenotypes. Acetylcholine values in the patient group were significantly lower. The atropine usage in conscious patients was significantly lower than unconscious patients. A significant difference was detected in the dose of used atropine between the clinically mild and moderate patients and the clinically mild and severe patient groups. The atropine requirement in the patient group needed endotracheal intubation was significantly higher than the patient group who did not require intubation. The average age of the recovered patients were significantly lower than those who died. The dose of organophosphate was lower in the recovered patient group when compaired to died patients. In conclusion, higher atropine requirements is associated with the clinical severity and entubation requirement in organophosphate intoxication. Advanced age is associated with higher mortality. PON phenotype has no relation with clinical condition and various biochemical parameters. Key words: Acetylcholine, atropine, organophosphate intoxication, paraoxanase. INTRODUCTION Intoxication with insecticides containing organophosphate occur either as a result of accidental or suicidal use of the agent. The main substances which have an effect towards reducing the effects of organic phosphate derivatives in the serum are paraoxanase and pseudocholinesterase enzymes. These are enzymes which hydrolyse organophosphates (1-3). PON has undertaken antioxidant properties and by breaking the oxane or paraoxane ring, transforms the toxin into an inactive form (4,5). Organophosphate compounds are strong inhibitors of cholinesterase (6). In cases of organophosphate intoxication (OPI), the levels of PON in the serum has been shown to be a parameter which determines the degree of which a patient is effected by toxins (4,5,7). Nicotinic and muscarinic findings will be observed when the agent shows its effect on the nerve-muscle conjunction. The effects of anticholinesterase agents expected in the cortical and subcortical regions of the central nervous system and in the autonomic target regions can be blocked by atropine (8,9). Atropine will also block some of the nicotinic and muscarinic effects originated from the autonomic ganglions. The clinical condition of the patient can vary from slight exhaustion, headache and salivation to severe tremor, generalized convulsions, inflammation of the lungs and even to death (10-14). The severity of intoxication can be determined by looking at the serum and erythrocyte cholinesterase levels. At the beginning, atropine can be used as an antidote for the muscarinic effects. In order to control nicotinic and central nervous system symptoms, oximes can be used as antidote (1,2,6,8). In this study, we first examined the clinical and laboratory findings of patients who were intoxicated with pesticide agents such as organophosphate or carbamate compounds. We later aimed to find a relation between how these findings were affected by such parameters as, the blood level of the substance, concentration of PON and cholinesterase in the serum and PON phenotype. MATERIAL AND METHODS Fourty two patients aged between 16 and 70 years old presenting with intoxication signs who took organophosphate either for suicidal use or accidentally and who were admitted to Izmir Ataturk Training and Research Hospital and 45 healthy volunteers as control were included in our study. Patients were divided into groups according to the severity of their clinical conditions and treatment was given after vital examinations and routine blood tests. First of all, atropine and pralidoxime (PAM) were administered 1000 mg of PAM was given via IV route lasting 5 minutes on admission. Blood samples were taken before the administration of PAM. PAM was continued for 3-5 days, according to the clinical condition of the patient. The first dose of atropine was 2-4 mg via IV route. According to the clinical condition of the patients, 2 mg was administered at every 15-20 minute intervals and than every hour without exceeding a total dose of 40 mgs. Apart from this administration, taking into account that the drug may have been taken via a dermal route or may have come in contact with the skin during vomiting, the patient was undressed and cleaned with soap and water. If the substance was taken orally and if the patient’s conscious state was suitable, the patient was vomited or the stomach was washed. Two doses of active charcoal were given. Postural drainage was applied to those patients whose bronchial secretions were more than normal. Mechanical ventilation via intubation was applied to those patients whose respiration either arrested or wasn’t efficient. The baseline serum PON activity, the stimulated PON activity, arylesterase activity, acetylcholinesterase activity and PON phenotype of all patients were determined. Basal PON Activity First PON was prepared as 120 mM stock, it is dissolved in acetone, and diluted with water. To the buffer of 0.1 M of TRIS-HCl (pH:8.0) containing 6 mM PON and 2 mM calcium chloride, serum was added and evolution rate of 4-nitrophenol at 412 nm wave length for 3 minutes was monitored. First 20 microliters of eserine was added to 180 microliters of serum, then 10 minutes later, 0.050 ml serum was added to the buffer and were monitored. Arylesterase Activity It was determined by monitoring the phenol quantity evolved from phenyl acetate. Phenol quantity which was evolved by adding serum to TRIS-HCl buffer (pH:8.0) containing 1 mM phenyl acetate and 0,9 mM calcium chloride, at 270 nm wavelength was monitored for 3 minutes. 1 unit is phenol quantity in micromoles evolved from 1 ml serum in one minute at room temperature. For calculations, extinction coefficient of the phenol was used. PON Phenotype Phenotypes were determined by using stimulation percentage with salt and stimulated PON/arylesterase ratio. Phenotypes were classified from trimodal distribution obtained by drawing histograms according to the stimulated PON ratios. If the ratio was <0.62, called as class AA, if the ratio was between 0.62 and 1.0 , as class AB, and if the ratio was >1.0 as BB. Acetylcholine Esterase Activity It is based on destruction of acetylthiocholine by CHS and conversion of the evolved product with (dithionitrobenzene) DTNB into a colored product. 0.1 M phosphate buffer (pH=8), acetylthiocholine iodide (0.075 M) and DTNB (0.01M) were mixed just before the test. 3 mls of it was added to this substrate and increase in the absorbance was monitored for 3 minutes at 412 nm wave length of the spectrophotometer. It is defined that enzyme quantity providing conversion of 1 micromole substrate in 1 minute at standard conditions is one unit and calculated by means of extinction coefficient. In order to study the factors which may have affected the patient’s clinical condition to be mild, moderate or severe, we initially divided the patients with OPI into three groups according to their consciousness state, as clear, confused and unconscious, and than we compared these groups according to the total amount of atropine, the amount of organophosphate ingested, plasma levels of PON and anticholinesterase, the patient’s heart rate and the number of days staying in hospital. We later divided these patients into two groups according to the requirement of mechanical ventilation. We also classified the patients into mild, moderate and severe cases according to their clinical condition. Among all the patients who were intoxicated with organophosphate, we compared the recovered patients with those who died at the end of the treatment, a comparison of patients according to their PON phenotypes was also made. Statistical Analysis SPSS 10.00 package software was used in the analysis. Continuous variables were expressed as means ±SD. Differences between the groups were evaluated on the basis of Chi-square and ANOVA tests. The value, p< 0.05 was accepted as a meaningful statistical result. RESULTS Baseline pseudocholinesterase activity of the patient and control group, was found to be significantly higher (p<0.01), (Table 1). When patients were divided according to their consciousness states, used atropine dose in the patient group with clear conscious was lower than other groups (p<0.001). When grouping patients according to their clinical signs and laboratory parameters, meaningful differences were observed in terms of the total dose of atropine used between the moderate to severe case group (p<0.001), and the mild to moderate case group (p<0.02). However, serum PON activity was found to be higher in the clinically severe group than in the clinically mild group (p<0.05). The required dose of atropine in the intubation required group was higher (p<0.01), (Table 2). The average age of died patients were found to be higher (p<0.01). The atropine dose used in the recovered patients was lower (p<0.01). The dose of organophosphate exposure in the recovered patients was lower (p<0.001), (Table 3). No significant difference was observed among the groups of patients who were divided into three groups such as A, AB, B according to their PON phenotypes (Table 4). DISCUSSION A relationship was observed between increased atherosclerosis and levels of PON in some patients (15-18). A great risk will be carried by the genetically present low PON activity patients with organic phosphorus intoxication and this will result in a worse clinical state (19,20). It is known that animals with low serum PON activity are more susceptible to OPI (2). In our study, no difference was detected in terms of PON activity between the control group and the patient groups. Therefore, our patients with OPI did not show any special susceptibility. The serum PON activity, of those with severe clinical signs, was found to be significantly higher than in the other two groups. This situation may be the reason why the ratio of death in patients with severe clinical signs are equal to those with moderate clinical signs. High PON activity may be protective against OPI (6,7). The ranking of organophosphate intoxication is made according to the decrease of CHS activity. Because organophosphate compounds inactivate acetylcholinesterase by binding to it. It is for this reason that in our study the observed low acetylcholinesterase level in the patient group was an expected finding. The high CHS levels will enable the organophosphate to bind before reaching the nerve conjunction and will provide a protective effect against intoxication (21). It is not realistic to make an assumption on the required atropine dose or on the prognosis, simply by taking into account the patients’consciousness state. The accompanying disturbed consciousness state in OPI, is an indication that the clinical state is severe (1-3). This condition has been shown in other studies (3,4,14,21). However, this condition may not always be true. It has been observed that in the grouping we have made, the unconscious group required more atropine than the conscious group. This shows that the unconscious state worsens the clinical state of OPI. However, despite the fact that the averages of the confused group with the conscious group and the confused group with the unconscious group were obviously different, this difference did not turn out to be significant. This may be due to the high standard deviation of the groups. Another matter is whether or not the CHS levels will show a difference according to the consciousness state of the patients. The CHS levels will also give an idea of whether or not the patients were really intoxicated with organophosphate and also how severe the efficacy is by looking at to which degree the enzyme has decreased (3,7,8,21,22). In our study, no relationship was found between the patients CHS levels and their consciousness states. According to our findings no relationship was found between the patients CHS level with severity of the clinical state and the consciousness state. In actual fact it was necessary, in this study, to measure the blood level of the oganic phosphorus taken and to observe whether or not this showed a correlation with the CHS level. We, however, tried to verify the amount of toxin taken, by roughly finding out from the patient or from their relatives. Naturally, under these circumstances, it was not possible to quantitate the intoxication by the dermal or respiratory routes. Also, the patients did not always bring the packaging of the drug they had taken and so the dosage of the drug was not identified. May be therefore, in our study we found that there was no correlation between CHS and the clinical condition of the patient. In terms of atropine requirement, significant differences were found between the mild, moderate and severe groups. The atropine dose increased with worsening clinical condition. When however, evaluating the patients’condition only in terms of whether or not the patient requires intensive respiratory support, independent of the patients clinical signs and CHS levels, it was observed that those patients requiring intubation required a higher dose of atropine. According to these results, the cases who needed respiratory support, will require more atropine doses. This was not an absolute rule. Although severe clinical conditions progress, the respiratory functions may not be disturbed but the patient may need a high dose of atropine requirement. We have not come across enough studies concerning this subject. In some cases whose intoxications are mild but the intervention have been delayed, and presenting with a respiratory arrest situation due to increased bronchial secretions, have taken intensive respiratory support and have dramatically taken advantage of this. In these patients although the toxin they took were of small amounts and the CHS levels were at a degree to show slight effectiveness, severe respiratory failure was the dominant feature. Whether or not these patients should be included into the clinically severe state patient group can be discussed but it is known that these patients were generally included into the severely affected group by the emergency service team. When our patient groups were divided into those who were cured and those who died, the age of those in the latter group were older. Alongside the finding that organophosphate intoxication has a more mortal progression at older ages, it will be useful to keep in mind that although we used nonparametric tests, due to the fact that we only had six death cases, there is a chance that this could be a coincidental finding which may mislead us. The amount of the drugs taken, which we determined to be of low quality and safety, together with atropine requirement was higher in the group where the patients died. We can say that this was also an expected finding. A significant difference among groups was observed as a result of dividing patients according to their phenotypic properties and by investigating them in terms of various parameters. However, this outcome may have been observed as a result of the fact that our study design was not appropriate for this kind of investigation. We hold the view that in the continuation of this study and with the aid of a design which will aim to determine the patients genotypic and phenotypic structures will help provide better answers. In conclusion, higher atropine requirements is associated with the clinical severity and entubation requirement in organophosphate intoxication. Advanced age is associated with higher mortality. PON phenotype has no relation with clinical condition and parameters suggest hospitalization duration atropine requirement, PON activity, aryl esterase activity and cholinesterase levels. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04017t3.jpg] [gm04017t2.jpg] [gm04017t1.jpg] [gm04017t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}