 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 38-42 ORIGINAL ARTICLE PLASMA HOMOCYSTEINE LEVELS IN PATIENTS WITH METABOLIC SYNDROME Aytekin Güven1, Fatma İnanç2 Sütçü İmam University, Faculty of Medicine, Departments
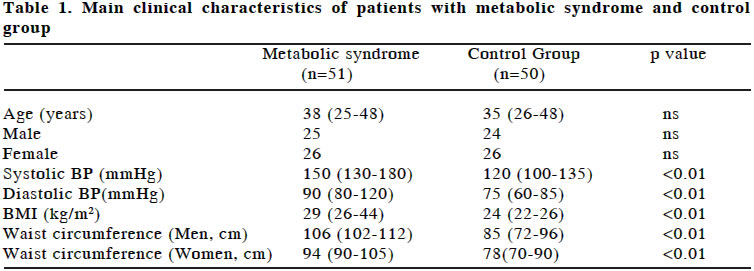
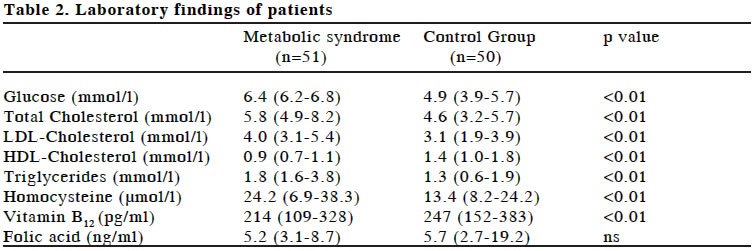
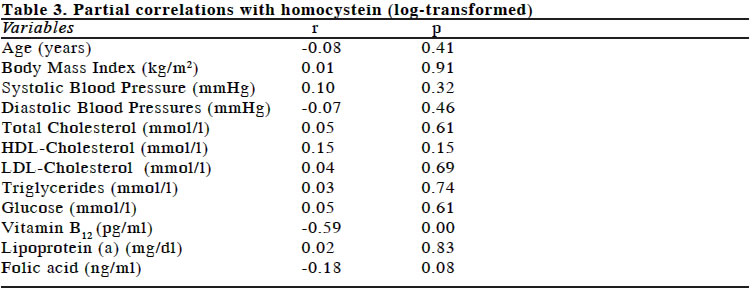
of Cardiology1 and Biochemistry2 Code Number: gm04018 A high serum total homocysteine (tHcy) level is an independent risk factor for cardiovascular disease. In this study, we examined the relationship of tHcy levels with the components of the metabolic syndrome. Fifty one patients diagnosed as metabolic syndrome (median age: 38 (25-48) years) and 50 healthy subjects (median age: 35 (26-48) years) were included in the study. Total homocysteine levels were significantly higher in metabolic syndrome group than in the control group (24.2µmol/l vs. 13.4µmol/l). Vitamin B12 levels were significantly lower in metabolic syndrome group than in the control group (214pg/ml vs. 247pg/ml). In partial correlation, tHcy concentrations were unrelated to metabolic syndrome or to the components of the metabolic syndrome, including fasting serum triglycerides, HDL-cholesterol, fasting glucose, blood pressure, or body mass index. tHcy levels were only strongly related to the vitamin B12 concentrations. The risk of cardiovascular disease is higher in patients with metabolic syndrome compared to the normal population. High tHcy levels might be evaluated in this group of patients in addition to evaluation of the parameters of metabolic syndrome. Key words: Metabolic syndrome, homocysteine, cardiovascular risk INTRODUCTION Metabolic syndrome is a clinical syndrome in which multiple risks are clustered in an individual and is a common basis of vascular disease in the industrial countries. Metabolic syndrome, dysmetabolic syndrome or insulin-resistance syndrome (or syndrome X as it was initially designated), which is closely linked to insulin resistance, is a condition, which is recognized as raising the risk of cardiovascular disease (1,2). It was originally described by Reaven (2) as quartet of hypertension, glucose intolerance and dyslipidemia (high triglyceride, low high-density lipoprotein-cholesterol (HDL-cholesterol), with insulin resistance or hyperinsulinemia. Central obesity is often associated and other phenotypes, such as impaired fibrinolysis, microalbuminuria, small dense low-density lipoprotein (LDL) particles and markers of acute phase reactants, were later found to be associated (2-4). The risk of atherosclerosis increased in patients with metabolic syndrome (5). Homocysteine (tHcy) is a sulfur-containing amino acid formed during the metabolism of methionine. Elevated levels of tHcy are toxic to vascular endothelium (6), including endothelial dysfunction and contributing to development of atherosclerosis independent of standard cardiovascular disease risk factors in diabetic (7,8) and nondiabetic subjects (9,10). Several observations suggest that there might be links between insulin resistance and hyperhomocysteinemia. Homocysteine levels have been found to be raised in patients with type 2 diabetes, both in the fasting state and after methionine loading, and are positively correlated with microalbuminuria (8,11,12). In rats made insulin resistant with a high fat sucrose diet, tHcy levels rise, and this increase is associated with changes in critical enzymes of tHcy metabolism. During a hyperinsulinemic euglycemic clamp, tHcy levels fall in nondiabetics, but not in patients with type 2 diabetes mellitus (13). It has been suggested that stimulation of insulin-induced elimination of methionine, which is impaired in diabetics, might underlie these relationships (14). In this study, we aimed to evaluate the plasma tHcy levels together in patients with metabolic syndrome and to find whether these values are correlated with the components of metabolic syndrome. MATERIAL AND METHODS Study population A total of 101 patients formed the study population. All subjects were given informed consent. The program included the taking of full medical history and physical examination, urinalysis, complete blood counts, blood chemistry, a glucose tolerance test, and electrocardiogram. The physical examination was performed by cardiologist and internist. Patients with coronary heart disease, significant valvular disease, diabetes mellitus, life-threatening systemic disease, chronic obstructive pulmonary disease and the smokers were excluded from the study. Biochemical analyses Blood samples were taken from all subjects between 8 and 10 AM after a 14-hour overnight fasting. Plasma concentrations of cholesterol, fasting triglycerides, HDL-cholesterol and glucose were determined by the enzymatic dry chemistry method using a Behring apparatus. LDL-cholesterol values were computed according to the Friedewald formula. Homocysteine All specimens were collected in Vacutainer (Becton-Dickinson, Franklin Lakes, NJ) blood-collecting tubes according to standard hospital guidelines for venous puncture and sample collection. Homocysteine specimens were placed on ice and all specimens were transported to the laboratory within 30 minutes of collection. Serum was obtained after centrifugation at 2,000 x g for 10 minutes, frozen, and stored at –20 ºC until analysis. Serum total homocysteine concentrations were measured by using an IMX (Abbott diagn. USA) homocysteine assay. Assay is based on the fluorescence polarization immunoassay (FPIA) technology. Folate and Vitamin B12 Vitamin B12 and folat assay is a paramagnetic particle, chemiluminescent immunoassay for the quantitative determination of Vitamin B12 and folat levels in human serum using the Access (Beckman, USA) immunoassay system. Definition of the metabolic syndrome The definition of the metabolic syndrome was as recommended by the National Cholesterol Education Program (15), and was considered to be present if the subject had three of the following factors: waist circumference >102 cm (men) or >88 cm (women), triglyceride level >1.69 mmol/l, HDL cholesterol <1.03 mmolI (men) or <1.29 mmol/l (women), blood pressure >130/85 mmHg, or fasting glucose >6.1 mmol/l. Statistical Analysis Data were analysed using SPSS 9.0 for Windows software package. Data was expressed as median and range. All variables were log transformed to normalize their distribution before statistical procedures. Student t test was used to compare the log-transformed data of patient and control groups. We used partial correlation coefficients to show the correlation between a variable and homocystein, while controlling for other variables. A value of p<0.05 was accepted as statistically significantly. RESULTS Total of 101 subjects were included in the study. Metabolic syndrome group consisted of 25 men and 26 women (median age: 38 (25-48) years) and the control group consisted of 24 men and 26 women (median age: 35 (26-48) years). There were no differences in age, sex between the two groups. The general characteristics of the study population are listed in Table 1. Blood pressure was found significantly higher in the metabolic syndrome group compared to the control group (150.0/90.0 mmHg vs. 120.0/75.0 mmHg, p<0.01). Body Mass Index (BMI) was higher in metabolic syndrome group than control group (29kg/m2 vs. 24 kg/m2 p<0.01). Waist circumference was higher in both men and women of metabolic syndrome group compared to the control group (Waist (men): 106cm vs. 85cm, p<0.01 and waist (women): 94cm vs. 78cm, p<0.01). When plasma lipid levels of both groups were compared, there was a significant difference between the two groups considering total cholesterol (p<0.01), LDL-cholesterol (p<0.01), HDL-cholesterol (p<0.01) and triglyceride (p<0.01). Fasting plasma glucose level was significantly higher in metabolic syndrome group than in the control group (6.4mmol/l vs. 4.9mmol/l, p<0.01). Baseline tHcy levels were shown in Table 2. tHcy and Lp(a) levels were significantly higher in metabolic syndrome group compared to the control group (tHcy: 24.2µmol/l vs. 13.4µmol/l, p<0,01 and Lp(a): 34.9mg/dl vs. 15.8mg/dl, p<0.01). The distribution of tHcy values ranged from 6.9 to 38.3µmol/l in metabolic syndrome group. Subjects with concentrations >15 µmol/l comprised 45% of men and 38% of women, whereas only 8% of patients had values >30µmol/l in group of metabolic syndrome. Vitamin B12 levels were significantly lower in metabolic syndrome group compared to the control group (214pg/ml vs. 247pg/ml, p<0.01) whereas there was no significant difference between the two groups considering folic acid levels (5.2ng/ml vs. 5.7ng/ml, p>0.05). Partial correlation analysis was performed between the components of metabolic syndrome and plasma levels of tHcy (Table 3). tHcy was not correlated with the components of metabolic syndrome. There was a significant negative correlation between tHcy and vitamin B12 (p<0.001). DISCUSSION An elevated plasma level of tHcy was first suspected to be associated with atherogenic and thrombogenic tendencies in patients with classic homocystinuria. This is a rare autosomal recessive disease caused in many cases by cystathionine β-synthase deficiency that results in very high plasma tHcy levels (as high as 400 µmol/l) and urinary tHcy excretion. This markedly elevated plasma concentration of tHcy is associated with thrombotic episodes (16-18). It has also been shown that milder degrees of hyperhomocysteinemia is associated with increased risk of vascular disease as well. Experimental studies have demonstrated that high plasma concentrations of tHcy may cause vascular damage and alteration in the coagulation process (19-22). There is increasing evidence that tHcy may affect the coagulation system and the resistance of the endothelium to thrombosis and that it may interfere with the vasodilator and anti-thrombotic functions of nitric oxide (23,24). The main results of our study was higher tHcy in patients with metabolic syndrome than the healthy subjects. However, we couldn’t find any correlation between plasma levels of tHcy and the components of metabolic syndrome. Vitamin B12 level was found significantly lower in patients with metabolic syndrome compared to the control group and there was a significant negative correlation between tHcy and vitamin B12 levels. In this study, higher tHcy levels in metabolic syndrome group compared to the control group might be a result of lower levels of vitamin B12. It’s interesting that we found a strong negative correlation between tHcy and vitamin B12 in our study. Various results have been reached in previous studies. Kahleova et al (25) found no correlation between tHcy and vitamin B12 in patients with metabolic syndrome. Jermendy et al (26) found normal tHcy and vitamin B12 levels in their study. In our study, low vitamin B12 levels are probably related with the eating habits of the patients. However, many studies showed negative correlation between tHcy and vitamin B12 (27). So, we think that vitamin supplement may be beneficial for the treatment in addition to a proper diet in such group of patients. Previous studies evaluating tHcy levels in patients with metabolic syndrome concluded differently. In Framingham Offspring Study, increased tHcy levels were shown to increase the risk of cardiovascular disease only in the presence of abnormal proteinuria in patients with insulin resistance. Because hyperhomocysteinemia and microalbuminuria also reflect endothelial injury, these observations also support the hypothesis that endothelial dysfunction is associated with expression of the metabolic syndrome (28). In another study, including 100 healthy men with metabolic syndrome, plasma homocysteine levels were not found significantly correlated with the parameters of metabolic syndrome except diastolic blood pressure (29). Their explanation for this situation was that there was endothelial damage in patients with metabolic syndrome in most of the studies but because their study included only healthy men with metabolic syndrome, they concluded differently. Valentine et al. (30) compared 50 white men aged 45 or younger at the onset of symptoms with age- and race-matched controls. Atherosclerotic risk factors were similar in both groups. These investigators reported no significant interaction between Lp(a) and tHcy in defining risk of cardiovascular artery disease. Because this study was small and included only men <45 years of age, generalizability of these results may be limited. In conclusion, many studies have shown that cardiovascular risk has been increased in patients with metabolic syndrome. We think that raised tHcy levels in patients with metabolic syndrome may increase this risk further. We have found tHcy levels increased in patients with metabolic syndrome; we suggest that these risk factors might be taken into consideration in addition to known risk factors during the evaluation of patients with metabolic syndrome. REFERENCES
Copyright 2004 - Medical Investigations Society
The following images related to this document are available:Photo images[gm04018t3.jpg] [gm04018t2.jpg] [gm04018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}